4836
Preoperative predictors of hyperperfusion after CEA: a study using vessel selective ASL1Radiology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Peking Union Medical College, Beijing, China, 2Peking Union Medical College Hospital, Beijing, China, 3Institute of Biophysics, Chinese Academy of Sciences, Beijing, China, 4GE Healthcare, MR Research China, Beijing, China
Synopsis
To identify preoperative predictors for cerebral hyperperfusion (CHS) after CEA based on vessel selective ASL. The perfusion volume of each brain feeding artery and the corresponding mean CBF in each perfusion volume before and after CEA were calculated. It was found that the sum of perfusion volumes corresponding to LICA, RICA and VBA (TotalPerVol) and the preoperative territory perfusion of the surgery side (preCBF_surg) was inversely correlated with the degree of CBF increase. The result indicated that tASL and ASL were useful in predicting cerebral hyperperfusion.
Introduction
Cerebral hyperperfusion syndrome(CHS) is a rare and critical complication after carotid endarterectomy (CEA) or carotid stenting (CAS)1. If CHS is not recognized and managed timely, it may further develop to intracerebral hemorrhage. Therefore, early identification of high risk CHS has high clinical value. In this work, vessel selective ASL is investigated as a preoperative predictor for cerebral hyperperfusion.Methods
Methods
A total of 127 patients confirmed with carotid stenosis and further underwent CEA in our hospital between May 2015 and September 2016 were enrolled in this retrospective study. The inclusion criteria was patients who underwent MRI exams including both standard ASL and tASL before and within 5 days after CEA; the exclusion criteria was patients with a large infarction. All MR exams were performed on a 3.0T whole body scanner (GE Discovery 750, Milwaukee, WI) with an eight-channel head coil. Conventional ASL and tASL(terrioty ASL) (LICA and RICA were labeled with super-selective strategy2, VBA was labeled with vessel-encoding stratey3). The scan parameters were: TR/TE 4886/10.5 ms, labeling duration 1450 ms, post labeling delay 2025 ms, FOV 240mm×240 mm, slice thickness 4.0 mm. Perfusion volume of each feeding artery (LICA, RICA and VBA) and its volume fraction in grey matter was calculated using MATLAB and SPM12, data analysis was as described previously 4. The sum of all three perfusion volumes fraction was defined as TotalPerVol. Then the grey matter perfusion volume was used as a mask in the standard ASL CBF map to generate the mean CBF of the perfusion territory of each vessel. Territory CBF ratio increase (r△CBF) was calculated as following to measure the degree of CBF increase after CEA: Territory CBF increase ratio (r△CBF) = (postCBF-preCBF)/preCBF Patients who had characteristic hyperperfusion symptoms such as headache on the ipsilateral side immediately after surgery with or without focal neurological deficits, and patients who had a postoperative ipsilateral CBF increase larger than 100% than baseline CBF were considered as cerebral hyperperfusion (CH)1. Statistical analysis was performed using SPSS. The spearman rank correlation was used to test the relationship between r△CBF and preoperative perfusion variates, i.e. TotalPerVol, CBF and perfusion volume. Receiver operating characteristic (ROC) curve was constructed and area under the ROC curve (AUC) was used to assess the predictive power.Results
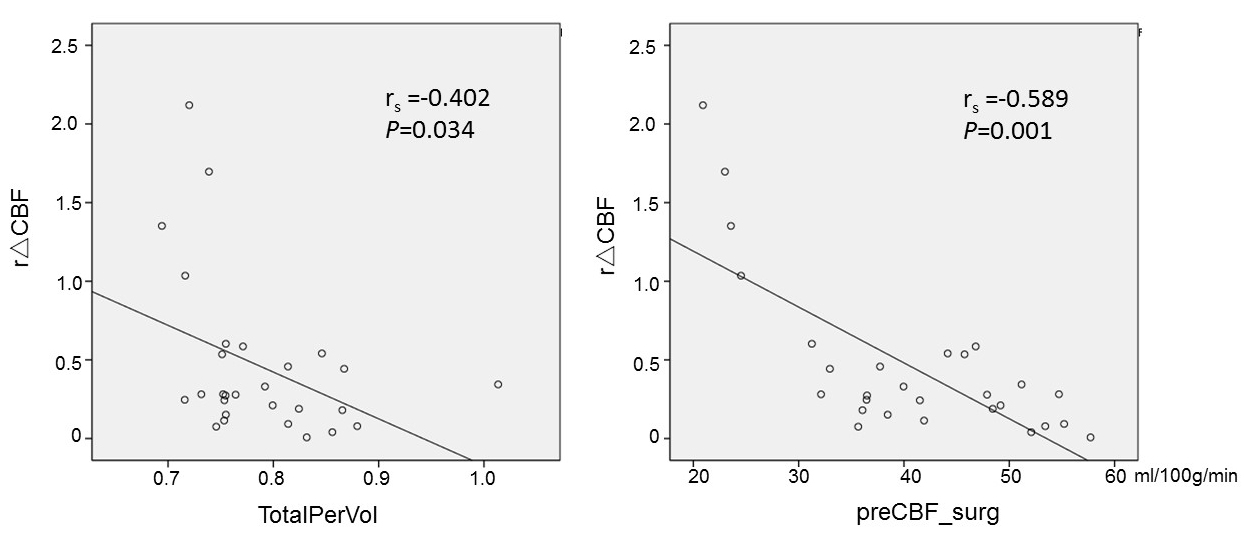
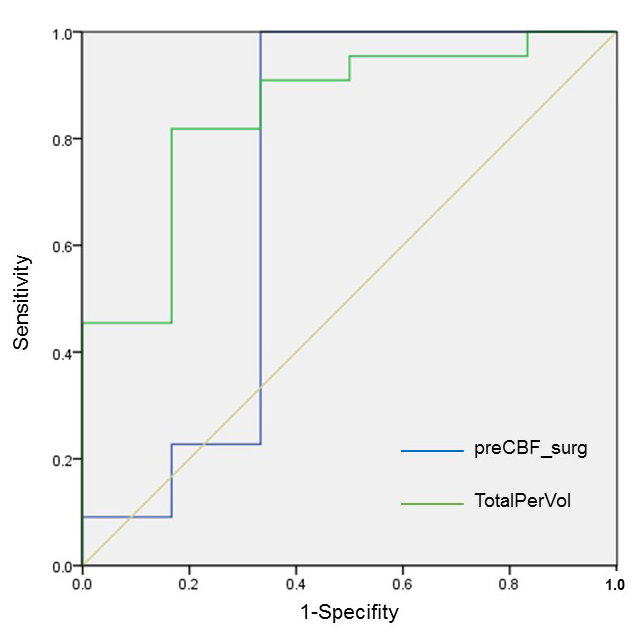
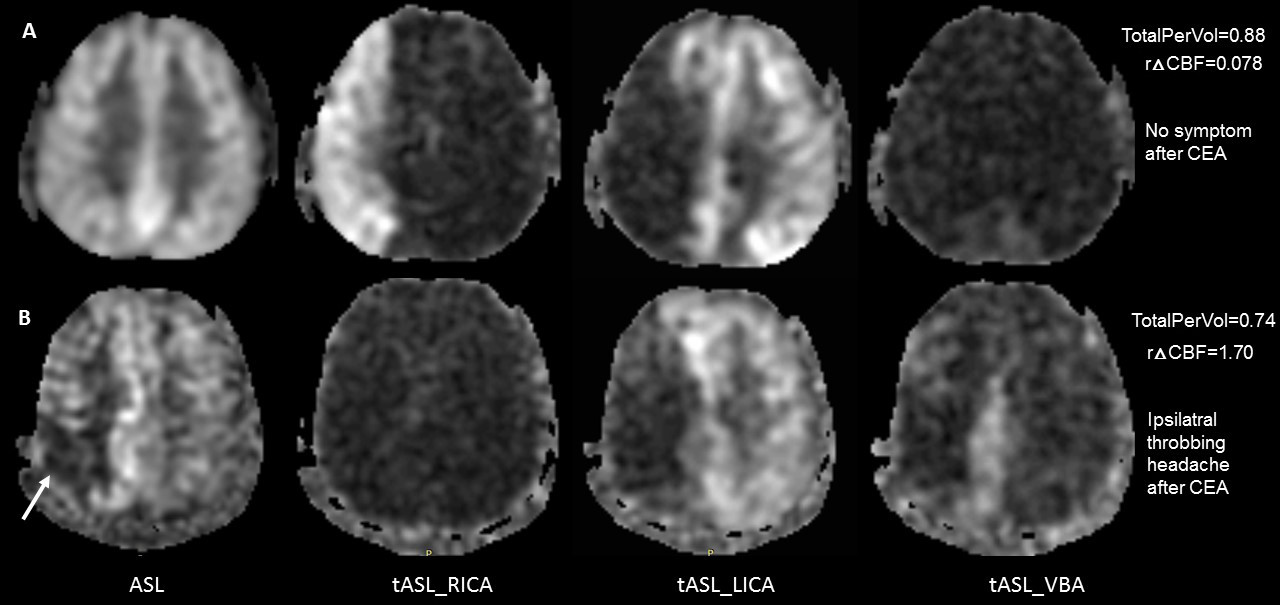
In the end, 28 patients were included in this study. Three patients (10.7%) had hyperperfusion related symptoms after surgery (throbbing ipsilateral or periorbital headache) and received treatment immediately. Among these symptomatic patients, one had ipsilateral CBF increase larger than100% (r△CBF =1.70, 3rd day after CEA), the other two patients showed CBF increase within normal range at the postoperative scan (r△CBF =0.28, 3rd day after CEA; r△CBF =0.21, 5th after CEA). Among the asymptomatic patients, three had ipsilateral CBF increase larger than 100% in the postoperative scan (mean±SD, r△CBF =1.55±0.47, mean 2.5 days after CEA). The TotalPerVol (Figure.1a) and preoperative CBF of the surgery side (preCBF_surg) (Figure.1b) inversely correlate with r△CBF (rs=-0.402, P=0.034, rs=-0.589, P=0.001). The ROC curve of TotalPerVol and preCBF_surg for predicting r△CBF was in Figure.2, AUC was 0.848 (95% CI, 0.674-1.000) for TotalPerVol, and 0.720 (95% CI, 0.396-1.000) for preCBF_surg. The cut-off value of TotalPerVol for predicting was 0.75179. There was no significant correlation between r△CBF and other preoperative variates. Images of two representative patients are shown in Figure.3.Discussion
In this study, it was suggested that patients with extremely low CBF region or with reduced and uncompensated perfusion territories were more vulnerable to hyperperfusion after carotid surgery. This finding was consistent with previous results that hyperperfusion occurs when ipsilateral perfusion volume was small, escape route (collateral circulation) and cerebral vasoreactivity (CVR) was poor 5, 6. Surprisingly, two patients in this study with CHS symptoms did not show large CBF increase. This may be due to the strict blood-pressure control treatment immediately after the onset of symptoms and the delay of postoperative scan after surgery (5 days and 3 days).Conclusion
The PreTotalPerVol and preCBF_surg parameters derived from tASL and ASL were useful in predicting cerebral hyperperfusion after CEA.Acknowledgements
NoneReferences
1. van Mook WN, Rennenberg RJ, Schurink GW, et al. Cerebral hyperperfusion syndrome. The Lancet Neurology 2005; 4: 877-888. 2005/11/22. DOI: 10.1016/s1474-4422(05)70251-9.
2. Helle M, Norris DG, Rufer S, et al. Superselective pseudocontinuous arterial spin labeling. Magnetic resonance in medicine 2010; 64: 777-786. 2010/07/03. DOI: 10.1002/mrm.22451.
3. Wong EC. Vessel-encoded arterial spin-labeling using pseudocontinuous tagging. Magnetic resonance in medicine 2007; 58: 1086-1091. 2007/10/31. DOI: 10.1002/mrm.21293.
4. Lin T, Lai Z, Lv Y, et al. Effective collateral circulation may indicate improved perfusion territory restoration after carotid endarterectomy. European radiology 2017 2017/09/13. DOI: 10.1007/s00330-017-5020-8.
5. Yamamoto D, Hosoda K, Uchihashi Y, et al. Perioperative Changes in Cerebral Perfusion Territories Assessed by Arterial Spin Labeling Magnetic Resonance Imaging Are Associated with Postoperative Increases in Cerebral Blood Flow in Patients with Carotid Stenosis. World neurosurgery 2017; 102: 477-486. 2017/03/23. DOI: 10.1016/j.wneu.2017.03.037.
6. Katano H, Mase M, Sakurai K, et al. Revaluation of collateral pathways as escape routes from hyperemia/hyperperfusion following surgical treatment for carotid stenosis. Acta neurochirurgica 2012; 154: 2139-2148; discussion 2148-2139. 2012/09/20. DOI: 10.1007/s00701-012-1498-7.
Figures