4799
4D Flow MRI analysis of cerebral blood flow before and after high-flow EC-IC bypass surgery for ICA aneurysm1Radiology, Nippon Medical School, Tokyo, Japan, 2Neurological surgery, Nippon Medical School, Tokyo, Japan, 3Radiology, Nihon University School of Medicine, Tokyo, Japan, 4Healthcare, Philips Electronics Japan, Tokyo, Japan
Synopsis
The purpose of this study was to clarify the change of hemodynamics after high-flow extracranial-intracranial (EC-IC) bypass surgery for ICA aneurysm by using time-resolved 3D-phase contrast (4D Flow) MRI. We enrolled 11 patients who underwent high-flow EC-IC bypass surgery. They underwent 4D Flow MRI before and after the surgery. We evaluated the blood flow direction of the circle of Willis. We measured blood flow volume (BFV) of bilateral ICAs, BA, and bypass artery. Seven of 11 patients exhibited collateral retrograde flow in the circle of Willis after surgery. The BFV of contralateral ICA and BA, and total brain BFV statistically increased after surgery. While, there was no evidence of post-operative hyperperfusion in any cases. 4D Flow MRI could quantify the change of hemodynamics after the high-flow bypass surgery.
Introduction
High-flow extracranial-intracranial (EC-IC) bypass surgery with permanent ligation of the ICA is the single therapeutic option for some patients with complex ICA aneurysm that cannot be treated by conventional strategies such as clipping or catheter embolization (1). Though the cerebral hemodynamics is thought to be changed drastically after the surgery, there has been no published papers performing quantitative evaluation. In the past decade, time-resolved three-dimensional phase contrast (4D Flow) MRI has been introduced to clinical MRI scanning protocols. Several acceleration techniques, including parallel imaging, partial k-space sampling, view sharing, and k-t acceleration techniques, have reduced scan times to meet clinical work flow objectives (total scan time is reduced to < 10 min to cover the entire circle of Willis as the target field of view) (1, 2). The purpose of this study was to validate the feasibility of 4D Flow MRI to assess the hemodynamic change before and after high-flow EC-IC bypass surgery.Materials & Methods
We enrolled 11 patients (2 men, 9 women; mean age, 69.8 years, range 22–76 years). who underwent high-flow EC-IC bypass surgery. They underwent 4D Flow MRI preoperatively and 3 weeks after the bypass surgery. The imaging parameters; 3.0-T MRI (Aheiva, Philips), repetition time/echo time 8.4/5.4 ms; turbo field echo factor 2; temporal resolution 67.2 ms; flip angle 13°; bandwidth 228.6 Hz; velocity encoding 70 cm/s,; field of view 210 × 210 × 44.8 mm3; 1 slab acquisition; voxel size 0.82 × 0.82 × 1.40 mm; 15 cardiac phases; sensitivity encoding factor 2; k-space shutter “On” (elliptical partial k-space coverage in phase- and slice-encoding direction); and nominal acquisition time approximately 6 min (3, 4). The velocity data were generated from a 4D Flow MRI data set using GT Flow software (GyroTools). 4D Flow MRI was performed to assess the collateral blood flow of the circle of Willis and to quantify the blood flow volume (BFV) of ipsilateral ICA (BFViICA), the bypass artery (BFVbypass), contralateral ICA (BFVcICA) and BA (BFVBA). Subsequently, the total BFV (BFVtotal = BFViICA + BFVcICA + BFVBA (before surgery), BFVcICA + BFVBA + BFVbypass (after surgery)) was calculated. All of these procedures took approximately 10 min per study. The BFV of each vessel and BFVtotal were compared between before and after surgery by using paired t-test. For all analyses, p < 0.05 was considered to be statistically significant. Postoperative hyperperfusion syndrome was evaluated based on clinical symptoms (e.g. severe unilateral headache, seizures, and focal neurological defects) within 3 weeks after the surgery.Results
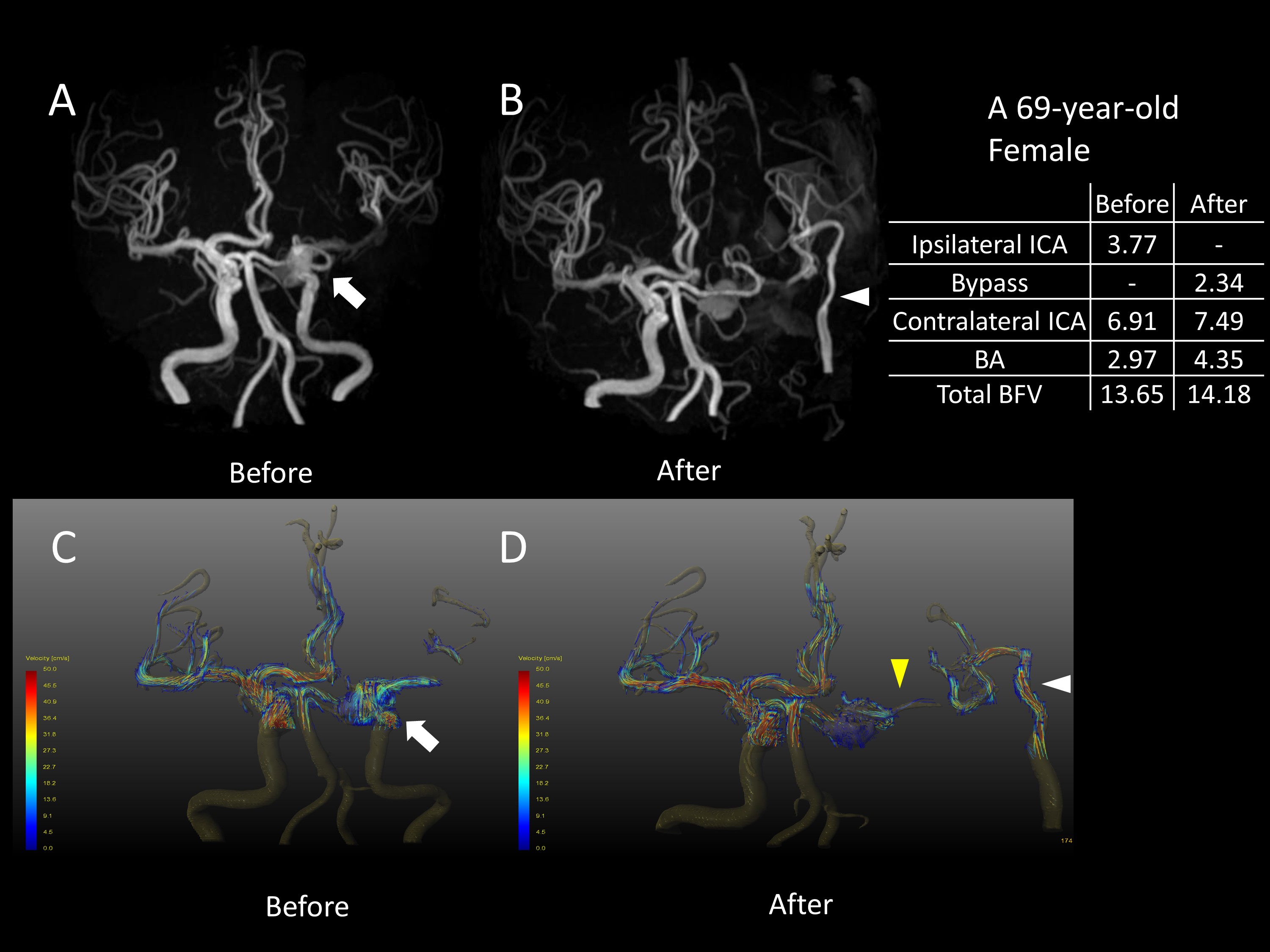
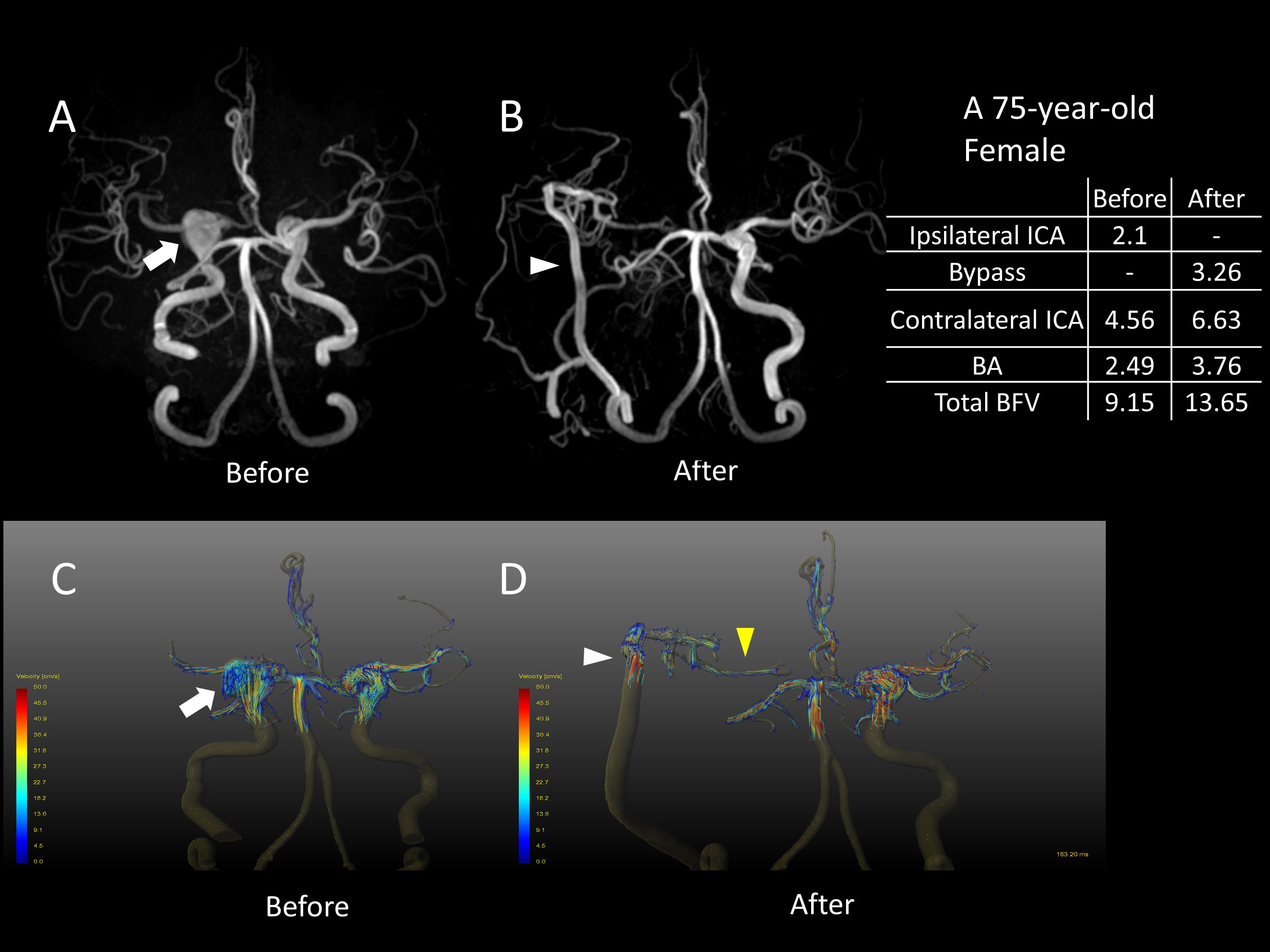
In all patients, the patency of the bypass artery was confirmed by 4D Flow MRI. The retrograde collateral flow on ipsilateral A1 was observed in one patient and that on ipsilateral posterior communicating artery was in six patients. Results of the BFV analysis are summarized in Figure 1 and 2. The BFVbypass was not statistically different but slightly lower than the BFViICA (3.84±0.94 ml/sec vs. 4.42±1.38 ml/sec). The BFVcICA and BFVBA were statistically increased after bypass surgery (BFVcICA 5.89±1.44 ml/sec vs. 7.22±1.37 ml/sec (p=.0018), BFVBA 3.06±0.41 ml/sec vs. 4.12±0.38 ml/sec (p<.001)). The BFVtotal was statistically increased after surgery (13.37±2.58 ml/sec vs. 15.18±1.77 ml/sec (p=.015)). Consequently, the BFVcICA, BFVBA, and BFVtotal increased by 22.6%, 34.6%, and 13.5% respectively. However, there was no evidence of hyperperfusion syndrome in any cases. A representative case is presented in Figure 3 and 4.Discussion
4D Flow MRI could visually and quantitatively verify cerebral hemodynamic changes after high-flow EC-IC bypass surgery with ICA ligation. Seven of 11 patients exhibited collateral retrograde flow in the circle of Willis after surgery. A slightly lower BFV of the bypass artery than in the sacrificed ICA, and increases in BFV of the contralateral ICA and BA, were observed. These qualitative and quantitative observations verify that the bypass artery could not fully compensate for the loss of BFV from the ipsilateral ICA which was occluded for the treatment of complex aneurysm. The native arteries―the contralateral ICA and BA―function in a complementary manner to compensate for blood flow supply through the circle of Willis. The total BFV was significantly increased by 13.5%. This result suggests that some autoregulation systems in the cerebral artery were slightly disrupted by bypass surgery, although not in a clinically relevant manner.Conclusion
After high-flow EC-IC bypass with permanent ICA ligation, the bypass artery could compensate but not fully the loss of blood flow volume of sacrificed ICA. The increased flow of contralateral ICA and BA supply collateral blood flow through the circle of Willis. 4D Flow MRI with 6 minutes scan is feasible to assess the hemodynamic change after high-flow EC-IC bypass surgery.Acknowledgements
This work was supported by JSPS KAKENHI (Grant Number 17K18160), Kurata Grants from the Hitachi Global Foundation (Grant Number 1309) and research grants from Fukuda Foundation for Medical Technology.
References
1. Hope TA, Hope MD, Purcell DD, et al. Evaluation of intracranial stenoses and aneurysms with accelerated 4D flow. Magnetic Resonance Imaging. 2010;28:41-46.
2. Sekine T, Amano Y, Takagi R, Matsumura Y, Murai Y, Kumita S. Feasibility of 4D flow MR imaging of the brain with either Cartesian y-z radial sampling or k-t SENSE: comparison with 4D Flow MR imaging using SENSE. Magn Reson Med Sci. 2014;13:15-24.
3. Sekine T, Takagi R, Amano Y, et al. 4D flow MRI assessment of extracranial-intracranial bypass: qualitative and quantitative evaluation of the hemodynamics. Neuroradiology. 2016;58:237-244.
4. Sekine T, Takagi R, Amano Y, et al. 4D Flow MR Imaging of Ophthalmic Artery Flow in Patients with Internal Carotid Artery Stenosis. Magn Reson Med Sci. 2017.
Figures
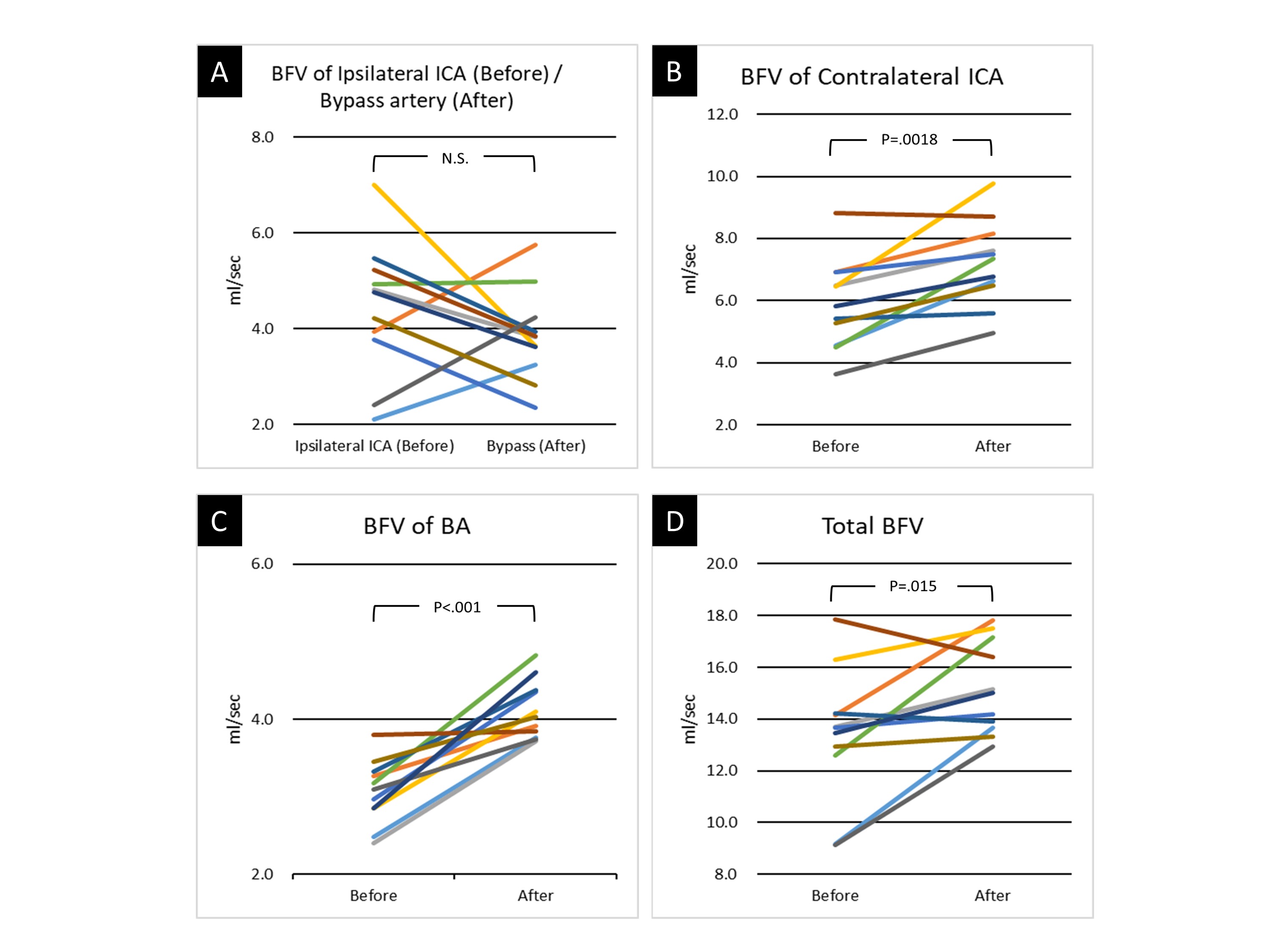
A: Comparison between blood flow volume (BFV) of Ipsilateral ICA (before surgery) and BFV of bypass artery (after surgery)
B-D:
Postoperative changes in BFV of contralateral ICA (B) , BFV of BA (C), and total BFV (D)
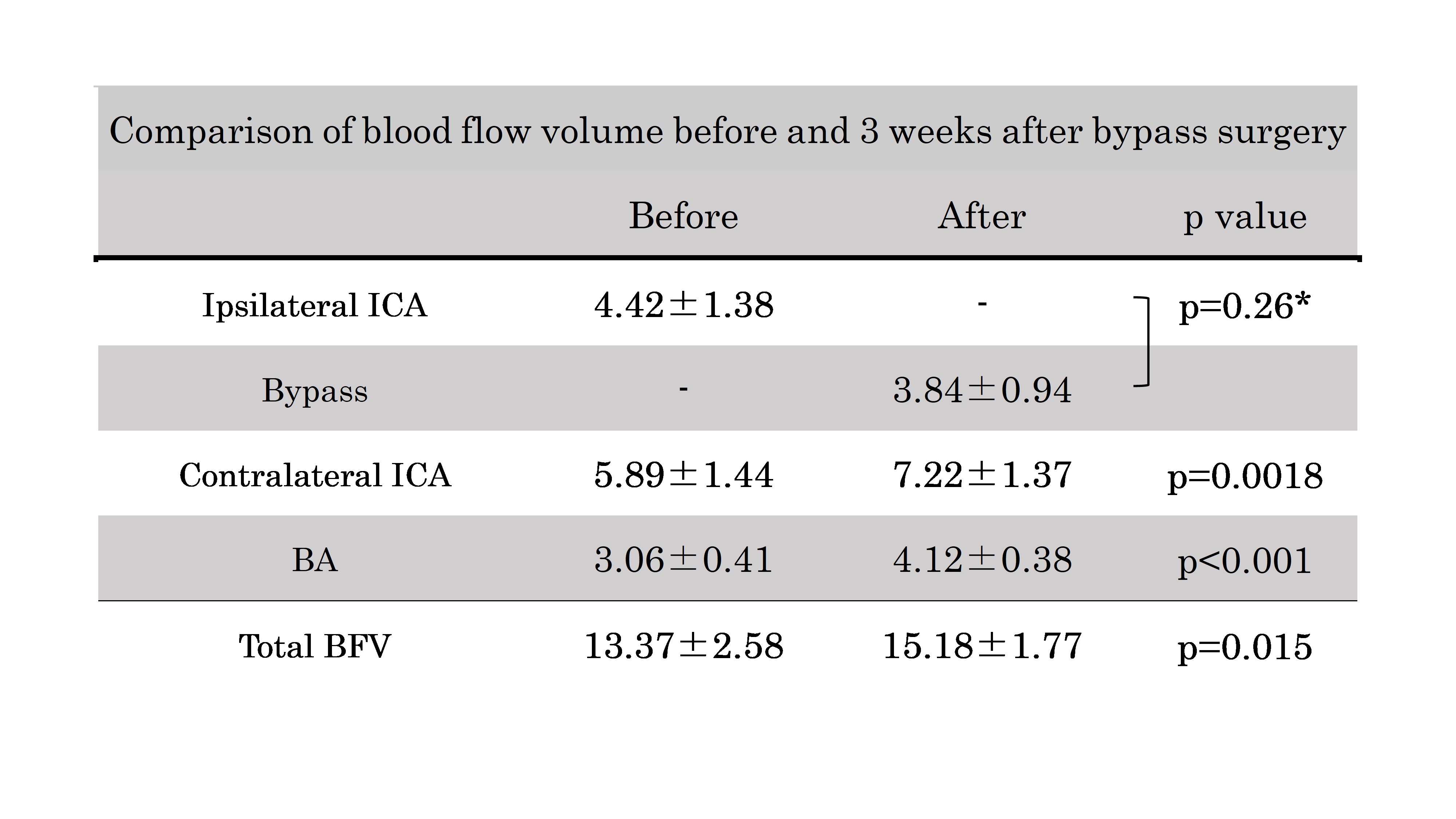
Comparison of blood flow volume (BFV) between before and 3 weeks after bypass surgery
*Comparison between blood flow volume (BFV) of Ipsilateral ICA (before surgery) and BFV of bypass artery (after surgery)