4793
Magnetic resonance imaging of the right ventricle: a simple scheme for self-correction of partial volume effect1Institute for Experimental Medical Research, Oslo University Hospital, Oslo, Norway, 2KG Jebsen Center for Cardiac Research, University of Oslo, Oslo, Norway
Synopsis
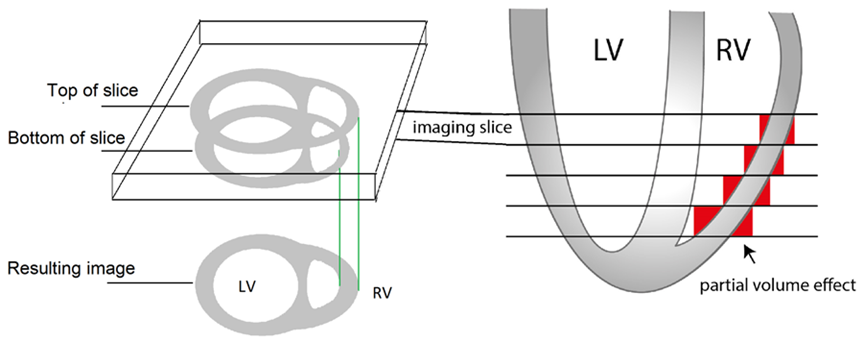
Magnetic resonance imaging (MRI) of the right ventricle (RV) offers important diagnostic information. However, analysis of RV MRI images is hampered by the crescent shape of the RV. In particular, pixels at the blood-myocardium border may contain signal from both blood and myocardium, hindering accurate analysis of ventricular volumes or mass. Here, we propose an easily implementable correction algorithm for analysis of standard CINE MRI image stacks, without the need for special acquisition. The proposed algorithm offers improved accuracy, in addition to more consistent RV mass estimates from CINE images of the heart in end systole and end diastole.
Background
Magnetic resonance imaging (MRI) of the right ventricle (RV) offers important diagnostic information. However, analysis of RV MRI images is hampered by the crescent shape of the RV. In particular, pixels at the blood-myocardium border may contain signal from both blood and myocardium, hindering accurate analysis of ventricular volumes or mass (see Figure 1). The shape of the RV renders it especially vulnerable to these effects. Our purpose was to develop and evaluate a novel self-correcting scheme improving the precision and accuracy of RV MRI image analysis.Materials and Methods
Here, we propose an easily implementable correction algorithm for analysis of standard CINE MRI image stacks, without the need for special acquisition. Briefly, the information from adjacent slices is used to identify the fraction of pixels influenced by partial volume effects, and correct the error introduced by these pixels. The technique relies on the assumption that half the area represented by pixels that is not shared between neighboring slices can be subtracted due to partial volume effects. In more details the process can be described as follows:
- In each slice $$$s$$$, all pixels containing myocardium are identified.
- The total number of myocardial pixels is counted, yielding $$$T(s)$$$.
- All pixels containing myocardium in slice $$$s$$$ that does not contain myocardium in the corresponding positions in slice $$$s-1$$$ are counted, yielding $$$T^{-}(s)$$$.
- All pixels containing myocardium in slice $$$s$$$ that does not contain myocardium in the corresponding positions in slice $$$s+1$$$ are counted, yielding $$$T^{+}(s)$$$.
- The total number of pixels in slice $$$s$$$ subject to partial volume effect is then estimated as $$$T^{-}(s)+T^{+}(s) $$$.
- The corrected number of pixels in slice $$$s$$$, $$$T'(s)$$$, is then estimated as:$$T'(s) = T(s) - \frac{T^{-}(s)+T^{+}(s)}{2}$$
- If the estimated number of partial volume pixels in a slice, $$$T^{-}(s)+T^{+}(s) $$$, is larger than the total number of pixels in the slice ($$$T(s)$$$), then $$$T'(s)$$$ is set to $$$\frac{T(s)}{2}$$$. In other words, no more than half the pixels are removed from a given slice.
- RV mass can then be estimated by multiplying the sum of $$$T'(s)$$$ over all slices with myocardial mass per pixel.
We evaluated this self-correcting segmentation method and compared with conventional (uncorrected) segmentation for measuring RV mass (RVm) in 17 rats without and with congestion (N=6/11, respectively). RVm was measured in both end-diastole (ED) and end-systole (ES). After MRI, the RV was excised and weighed. Measurement precision and accuracy of RVm were assessed by comparing ED and ES measurements, as well as comparing RVm to ex vivo RV weight.
Results
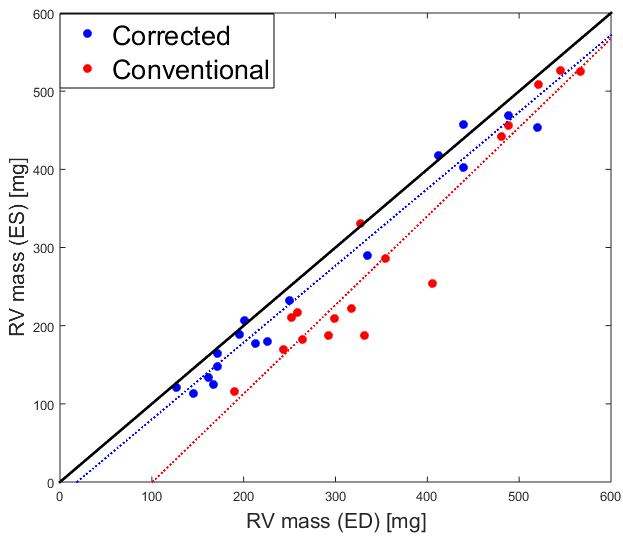
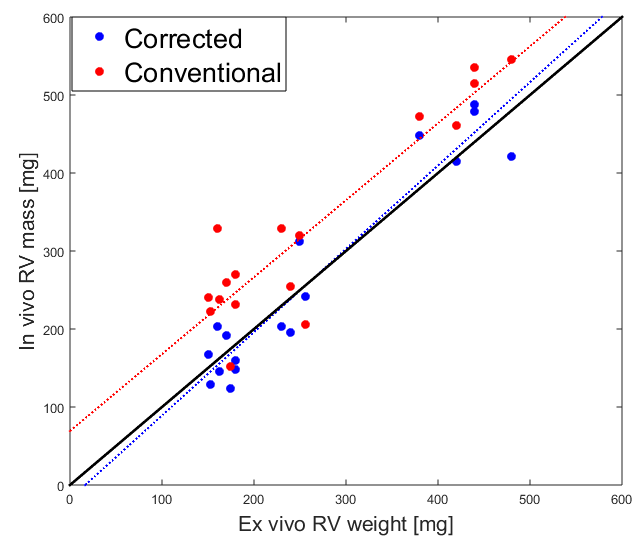
We found that the agreement between ED and ES measurements of RVm was better for the self-corrected scheme compared to the conventional approach (correlation: ρ=0.99 vs ρ=0.96 and limits-of-agreement 22±43 mg/8.7±17% vs 65±85 mg/20±26%, see Figure 2). We also found that RVm agreed better to ex vivo RV weight using the self-correction compared to conventional approach (correlation: ρ=0.95 vs ρ=0.92 and limits-of-agreement -0.2±79 mg/-0.1±30% vs -65±98 mg/-22±33%, see Figure 3).
Conclusion
For MRI RV mass measurements, the proposed algorithm offers more consistent RV mass estimates from CINE images of the heart in ES and ED, compared to the conventional approach. Furthermore, comparison between in vivo RVm and ex vivo RV weight demonstrate that the proposed approach provides improved accuracy compared to the conventional approach.
Acknowledgements
No acknowledgement found.References
1. Beygui F, Furber A, Delepine S, Helft G, Metzger JP, Geslin P and Le Jeune JJ. Routine breath-hold gradient echo MRI-derived right ventricular mass, volumes and function: accuracy, reproducibility and coherence study. Int J Cardiovasc Imaging 20: 509-516, 2004.
2. Strugnell WE, Slaughter l, Riley RA, Trotter AJ and Bartlett H. Modified RV short axis series--a new method for cardiac MRI measurement of right ventricular volumes. J Cardiovasc Magn Reson 7: 769-774, 2005.
3. Wiesmann F, Frydrychowicz A, Rautenberg J, Illinger R, Rommel E, Haase A and Neubauer S. Analysis of right ventricular function in healthy mice and a murine model of heart failure by in vivo MRI. Am J Physiol Heart Circ Physiol 283: H1065-H1071, 2002.
Figures