4767
Feasibility of EPI for cardiac diffusion at 7T1Oxford Centre for Clinical Magnetic Resonance Research, University of Oxford, Oxford, United Kingdom, 2Oxford Centre for Functional MRI of the Brain, University of Oxford, Oxford, United Kingdom
Synopsis
Cardiac diffusion imaging promises new insights into myocardial microstructure and integrity, but is an SNR-starved technique. Imaging at 7T may enable fewer signal averages, but most cardiac diffusion implementations use an EPI readout, which suffers from spatial distortion at higher field strengths. In this work we demonstrate distortion-corrected, EPI-based, cardiac diffusion tensor imaging at 7T using images acquired with forward and reversed phase encoding directions. We find myocardial ADC and FA consistent with previously published 3T data and that, with this acquisition protocol, distortion correction does not lead to statistically significant changes in ADC and FA.
Introduction
Cardiac diffusion imaging has the potential to provide new insights into cardiac microstructure and integrity. One widely used cardiac diffusion method uses an EPI readout after a stimulated echo diffusion preparation, enabling accurate quantification of apparent diffusion coefficient (ADC) and fractional anisotropy (FA)1,2. However, this is an SNR-starved technique and typically 6-10 averages are used at 3T to obtain reliable measures. Cardiac imaging at 7T promises increased SNR, but geometric distortion in EPI images due to B0 field inhomogeneity is also increased. In the brain, this has been mitigated by acquiring diffusion images with forward and reversed phase encoding gradients and combining these images to estimate a B0 field map, thence combining the images to a single undistorted one3. The hypothesis of the present work was that it would be possible to obtain reliable ADC and FA at 7T using this same method in the heart.Methods
Four healthy males were scanned on a 7T whole body scanner (Siemens) using ECG gating, an 8-channel parallel transmit array4,5 with B1+ shimming (maximising minimum B1+ in a region of interest) and B0 shimming (Siemens WIP 452) optimised over the left ventricle in a mid-ventricular short axis slice through the heart. The stimulated echo diffusion sequence was as previously described2, with TR/TE 2 RR intervals/22ms, matrix 128x48, FoV 360x135mm, GRAPPA 2x acceleration, slice thickness 8mm, BW 2242 Hz/pixel, reference b=15 s/mm2, six diffusion directions at b=350 s/mm2, run without fat saturation at peak systole. Eight averages with the phase encoding (PE) running in the default direction were acquired, and four averages with the PE blips reversed. Images were reconstructed in SNR units using the Gadgetron framework6,7 and mean SNR calculated over the left ventricular myocardium. Eight reference images (four in each PE direction) were used to estimate the susceptibility-induced off-resonance field using a method similar to that described by Andersson et al3 as implemented in FSL8 and the eight distorted averages were combined into eight corrected averages. A custom script replicated the single imaging slice 8 times, with two empty slices above and below, in order to enforce motion and B0 field gradients to be zero in the through-slice direction, as the above code expects a 3D dataset. The resulting distortion-corrected diffusion images were processed as described previously2 to obtain ADC, FA and helix angle maps, as were eight averages with consistent PE direction but without distortion correction. Mean ADC and FA over the left ventricle were calculated for each subject and averaged, and compared using an unpaired t-test, with a significance level of p<0.05 after Bonferroni correction, to previously measured ADC and FA for normal volunteers at 3T2. A paired t-test was used to test for significant differences segmentally in ADC and FA calculated from corrected and uncorrected images. In two subjects, the contoured shape of the left ventricle before and after distortion correction was compared to that at the same trigger delay in a GRE cine, with the overlap quantified using the Jaccard index.
Results
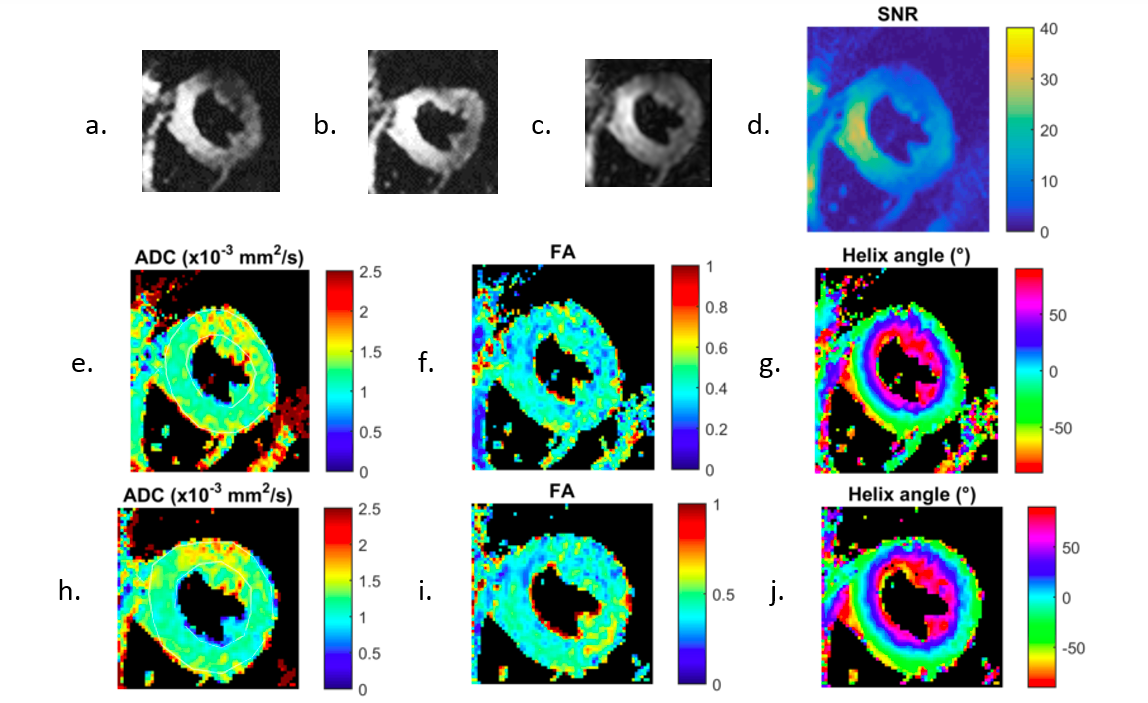
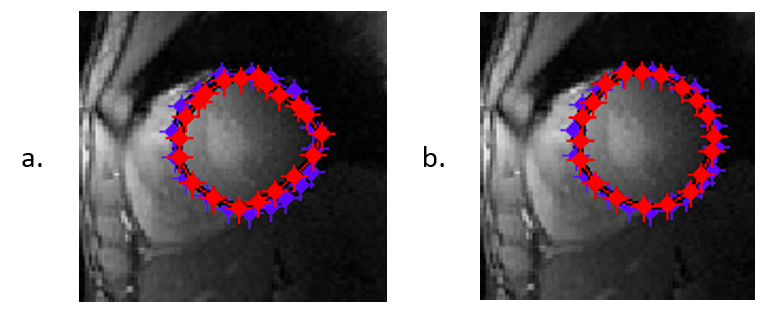
Example reference images and maps from one subject are shown in Figure 1. The mean myocardial SNR in a single average of this mid-ventricular slice for all subjects was 11±2 and was 16±4 septally. Mean ADCs and FAs are shown in Figure 2, which shows that there were no statistically significant differences between 7T and 3T. There were also no statistically significant differences between corrected and uncorrected ADC or FA. The Jaccard indices were 0.87 and 0.92 for contours drawn on uncorrected images and 0.94 and 0.95 for contours drawn after distortion correction, showing improved agreement of the myocardial shape with the reference GRE in the EPI image after correction. Examples are shown in Figure 3.Discussion
The short (12ms) readout employed in this sequence is sufficient to avoid gross distortion of the myocardium, and the distortions which are present can be effectively corrected using the method of Andersson et al3. However, we note that the average SNR is lower than that previously reported at 3T9. This is driven by very poor SNR in the lateral wall, and even in the septum the SNR is only equivalent to that measured at 3T. The use of a 32 channel receive array at 3T but only an 8-channel TR array at 7T may partially explain the reduced SNR and this is an area we are presently addressing.Conclusions
Spatial distortion of the myocardium in EPI-based diffusion imaging at 7T does not significantly alter ADC or FA values and can be corrected using a forward and reversed PE blip method.Acknowledgements
The research was supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre Programme. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.References
1. Edelman RR, Gaa J, Wedeen VJ et al. In vivo measurement of water diffusion in the human heart. Magn Reson Med. 1994;32(3):423-428.
2. Tunnicliffe EM, Scott AD, Ferreira P et al. Intercentre reproducibility of cardiac apparent diffusion coefficient and fractional anisotropy in healthy volunteers. J Cardiovasc Magn Reson. 2014;16:31.
3. Andersson JLR, Skare S, Ashburner J. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. NeuroImage. 20(2):870-888, 2003.
4. Snyder CJ, DelaBarre L, Moeller S, et al. Comparison Between Eight- and Sixteen-Channel TEM Transceive Arrays for Body Imaging at 7 Tesla. Magn Reson Med. 67(4):954-964, 2012.
5. Keith GA, Rodgers CT, Hess AT et al. Automated tuning of an eight-channel cardiac transceive array at 7 tesla using piezoelectric actuators. Magn Reson Med. 73(6):2390-2397, 2015.
6. Kellman P, McVeigh ER. Image reconstruction in SNR units: a general method for SNR measurement. Magn Reson Med. 54(6):1439-47, 2005.
7. Hansen MS, Sørensen TS. Gadgetron: an open source framework for medical image reconstruction. Magn Reson Med. 69(6):1768-76, 2013.
8. Smith SM, Jenkinson M, Woolrich MW et al. Advances in functional and structural MR image analysis and implementation as FSL. NeuroImage. 23(S1):208-219, 2004.
9. McGill LA, Scott AD, Ferreira PF, et al. Heterogeneity of Fractional Anisotropy and Mean Diffusivity Measurements by In Vivo Diffusion Tensor Imaging in Normal Human Hearts. PLoS One. 10(7):e0132360, 2015.
Figures