4731
Magnetic resonance cholangiopancreatography using optimized integrated combination with parallel imaging and compressed sensing technique compared with conventional MRCP.1Department of Radiology, Gifu University School of Medicine, Gifu, Japan, 2Department of Radiology Services, Gifu University Hospital, Gifu, Japan, 3Philips Japan, Tokyo, Japan
Synopsis
MR cholangiopancreatography (MRCP) plays an essential role in the noninvasive assessment of the biliary and pancreatic duct systems. The current respiratory-triggered three-dimensional turbo spin-echo MRCP sequence has an excellent duct-to-periductal tissue contrast, however, the long acquisition time and motion artifacts due to the various depth of patients’ breathing limit the benefit of this sequence. We assessed prototype sequence using optimized integrated combination with parallel imaging and compressed sensing technique (Compressed-SENSE) for MRCP. Our results demonstrated that Compressed-SENSE technique enabled significant reduction of acquisition time without image quality degradation compared with conventional method.
Introduction
MR cholangiopancreatography (MRCP) is widely used as a noninvasive modality for the anatomical evaluation of the biliary and pancreatic duct systems. The most common sequence used in three-dimensional (3D) MRCP is a respiratory- or navigator-triggered 3D T2-weighted turbo spin-echo (TSE) sequence1. Respiratory-triggered 3D T2-weighted TSE MRCP has considerably contributed to a wide coverage, a thinner effective slice thickness, and high signal-to-noise ratio (SNR), whereas this sequence has a disadvantage of the weakness in motion artifacts due the various depth of patients’ breathing during the long acquisition time2.
The accelerated parallel imaging (PI) technique, as for instance SENSE (sensitivity encoding), has developed and achieved the significant reduction of acquisition time. Recently, the compressed sensing (CS) image acquisition and reconstruction technique has applied to clinical settings2-4. CS technique can increase acquisition speed by recovering image information from highly under-sampled sparse k-space data5. Since MRCP images are inherently sparse in terms of pixel representation, CS technique can be particularly suitable for MRCP.
In this study, we assessed prototype respiratory-triggered 3D T2-weighted TSE sequence using optimized integrated combination with PI and CS technique (Compressed SENSE) for MRCP. We hypothesized that the use of Compressed SENSE may contribute the significant reduction of acquisition time without degradation of during MRCP. The purpose of this study was to evaluate the feasibility of Compressed SENSE technique in MRCP compared with conventional MRCP.
Methods
This prospective HIPAA-compliant study was approved by our institutional review board. Written informed consent was obtained from all patients. Fifty-eight consecutive patients (30 men, 28 women, age range 17-86 years, mean age 67.2 years) with suspicious having pancreaticobiliary diseases underwent MRCP. All patients underwent breath hold 3D gradient and spin echo (GRASE) MRCP with SENSE (BH-MRCP; SENSE factor, 2), conventional respiratory-triggered 3D TSE MRCP with SENSE (RT-MRCP; SENSE factor, 2) and respiratory-triggered 3D TSE MRCP with Compressed SENSE (RT-MRCPCS; CS-SENSE factor, 7.5) at a 3-T clinical scanner (Ingenia CX; Philips Healthcare, Netherlands) with a 32-channel phased-array receiver coil. For quantitative image analyses, signal intensity (SI) of right hepatic duct (RHD), left hepatic duct (LHD), common bile duct (CBD), three segments (pancreatic head, body and tail) of main pancreatic duct (MPD), peribiliary ductal tissue, and peripancreatic ductal tissue were measured. The relative duct-to-periductal contrast ratios (RCs) of each pancreaticobiliary segments were calculated as (SIduct - SIperiduct) / (SIduct + SIperiduct), respectively. For qualitative image analyses, two radiologists coincidentally graded visibility of central or peripheral RHD / LHD, common hepatic duct, cystic duct, CBD, MPD and pancreatic cystic lesion, motion artifacts, and overall image quality among three sequences using a five-point rating scale. Quantitative measurements and qualitative scales were compared between three sequences using repeated measures ANOVA/pairwise t-test with Bonferroni correction (BC) and Friedman test with pairwise Wilcoxson signed rank test with BC, respectively.Results
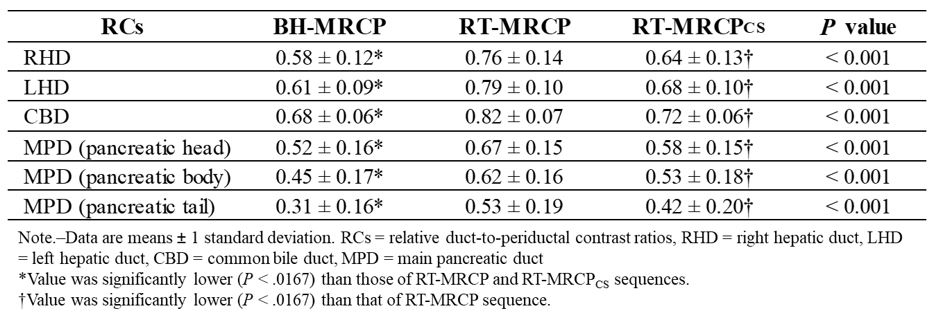
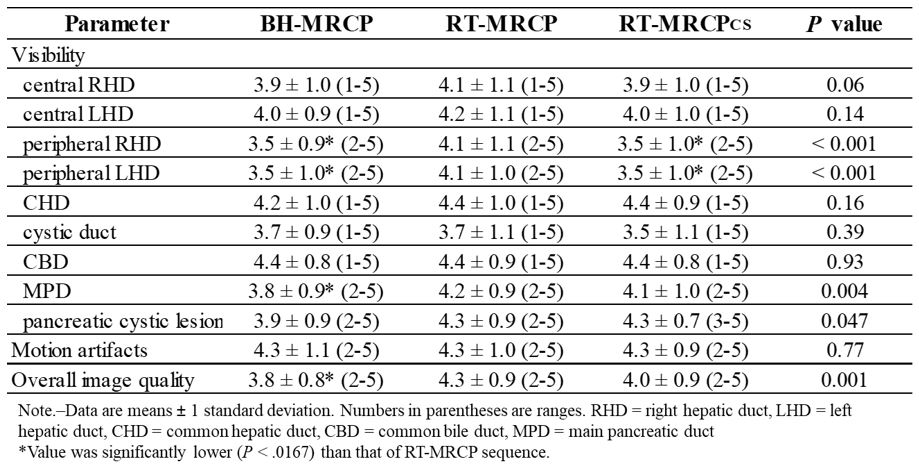
Mean acquisition time in each sequence was 201 seconds in RT-MRCP, 45 seconds in RT-MRCPCS, and 23 seconds in BH-MRCP sequence. Quantitative results were demonstrated in Table 1. RCs of RHD, LHD, and CBD were significantly higher in the order corresponding to RT-MRCP (0.82, 0.76, 0.79), RT-MRCPCS (0.72, 0.64, 0.68), and BH-MRCP sequences (0.68, 0.58, 0.61) (P < 0.001). RCs of all three segments of MPD were significantly higher in the order corresponding to RT-MRCP (0.82, 0.76, 0.79), RT-MRCPCS (0.58, 0.53, 0.42), and BH-MRCP sequences (0.52, 0.45, 0.31) (P < 0.001). Visibility of peripheral RHD and LHD in RT-MRCP sequence (4.1, 4.1) was slightly higher than those in RT-MRCPCS (3.5, 3.5) and in BH-MRCP (3.5, 3.5) (P < 0.001) but was kept within the acceptable range. Qualitative scores of other pancreaticobiliary segments, motion artifacts and overall image quality were comparable between RT-MRCP and RT-MRCPcs sequences.Discussion
Our results demonstrated that total acquisition time in RT-MRCPCS fell by about 78% compared with that in conventional RT-MRCP without significant degradation of image quality. Qualitative scores for visualizations of pancreaticobiliary segments in RT-MRCPCS sequence were kept within the acceptable range and were comparable to those in RT-MRCP in most of pancreaticobiliary segments without thin distal bile duct. We believe that RT-MRCPCS sequence can contribute to improve the throughput time for MRCP and could be valuable in clinical use.Conclusion
RT-MRCPCS markedly reduced scan time by quarter and demonstrated comparable image quality compared with conventional RT-MRCP.Acknowledgements
No acknowledgement found.References
1. Lee JH, Lee SS, Kim JY, et al. Parallel imaging improves the image quality and duct visibility of breathhold two-dimensional thick-slab MR cholangiopancreatography. Journal of magnetic resonance imaging : JMRI 2014;39:269-75.
2. Seo N, Park MS, Han K, et al. Feasibility of 3D navigator-triggered magnetic resonance cholangiopancreatography with combined parallel imaging and compressed sensing reconstruction at 3T. Journal of magnetic resonance imaging : JMRI 2017.
3. Yoon JH, Lee SM, Kang HJ, et al. Clinical Feasibility of 3-Dimensional Magnetic Resonance Cholangiopancreatography Using Compressed Sensing: Comparison of Image Quality and Diagnostic Performance. Investigative radiology 2017;52:612-9.
4. Zhu L, Wu X, Sun Z, et al. Compressed-Sensing Accelerated 3-Dimensional Magnetic Resonance Cholangiopancreatography: Application in Suspected Pancreatic Diseases. Investigative radiology 2017.
5. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic resonance in medicine 2007;58:1182-95.
Figures