4716
Conical Ultrashort TE (UTE) MRI in the evaluation of pediatric acute appendicitis1Radiology, Stanford University, Stanford, CA, United States, 2Radiology, First Affiliated Hospital, Chongqing, China
Synopsis
To reduce patient exposure to the ionizing radiation of CT, hospitals are increasing MRI usage in the evaluation of suspected acute appendicitis, particularly in the pediatric population. Our retrospective review of 84 pediatric patients assessed contrast-enhanced conical Ultrashort TE (UTE) of the pelvis. UTE demonstrated better qualitative Signal-to-Noise Ratio (SNR), fewer artifacts, and better overall image quality than both a 3D dual-echo SPoiled GRadient echo (SPGR) sequence and a free-breathing high-resolution 3D SPGR. Our study concluded that UTE is feasible in the evaluation of the pelvis for pediatric acute appendicitis.
Introduction
CT is commonly used to evaluate suspected appendicitis, but its ionizing radiation limits its use in children. To reduce patient exposure to the ionizing radiation of CT, hospitals are increasing MRI usage [1-3]. This study assesses contrast-enhanced conical Ultrashort TE (UTE) MRI acquired during free breathing in the evaluation of the pediatric pelvis for suspected appendicitis. We hypothesize that this sequence is feasible and may be superior to a Breath-Hold 3D dual-echo SPoiled GRadient echo (BH-SPGR) sequence and a Free-Breathing high-resolution 3D SPGR (FB-SPGR) sequence.Methods
84 consecutive patients aged 18 years and under who underwent contrast-enhanced MRI at 3T for suspected appendicitis were retrospectively identified. Each patient underwent three contrast-enhanced MRI sequences of the pelvis (Table 1):
· UTE: free-breathing conical UTE with golden-angle view ordering and intermittent fat suppression [4].
· BH-SPGR: 3D SPGR with dual-echo water-fat separation utilizing parallel-imaging acceleration acquired during an attempted breath hold.
· FB-SPGR: free-breathing high-resolution 3D SPGR acquired without acceleration and using intermittent fat-suppression.
BH-SPGR was performed first on all patients, followed by FB-SPGR then UTE in 69 patients (82%) and UTE then FB-SPGR in 15 patients (18%).
Two radiologists performed blinded and independent evaluations of each contrast-enhanced sequence for image quality, anatomic delineation, and diagnostic confidence. Subsequently, the three sequences were reevaluated for overall image quality and directly compared to each other with simultaneous viewing.
The three sequences were compared using one-way ANalysis Of VAriance (ANOVA), post-hoc Tukey Honestly Significant Difference (HSD) test, and Bonferroni-Holm correction for multiple comparisons. Subgroup analysis using unpaired two-tailed T-test was performed comparing the patients with UTE performed before FB-SPGR to those with FB-SPGR before UTE. Inter-observer agreement was evaluated with Intraclass Correlation Coefficients (ICC).
Results
The mean age of our patients was 11 years; 56% were female. The appendix was visualized in 63 patients (75%). Of the 84 total patients, 14 (17%) were diagnosed with acute appendicitis.
UTE demonstrated better qualitative Signal-to-Noise Ratio (SNR) and fewer artifacts (p=0.00006 and 0.01080, respectively) than both BH-SPGR and FB-SPGR; BH-SPGR demonstrated better contrast (p=0.00002) than both UTE and FB-SPGR. Otherwise, there was no statistical difference between UTE and BH-SPGR in blurring, anatomic delineation, and diagnostic confidence, although both UTE and BH-SPGR performed better than FB-SPGR (Table 2). Direct paired comparisons of overall image quality demonstrated similar results (Table 3): the readers preferred UTE over FB-SPGR (+1.2), while slightly favoring UTE over BH-SPGR (+0.5).
Subgroup analysis determined that FB-SPGR yielded better image quality, anatomic delineation, and diagnostic confidence (p<0.05) when performed before UTE compared to FB-SPGR performed after UTE. Other than better contrast (p=0.04), there was no statistical difference in UTE when performed before FB-SPGR compared to UTE performed after FB-SPGR. Inter-observer agreement was greater overall for UTE and BH-SPGR than FB-SPGR. Both UTE and BH-SPGR had six (out of nine) parameters with good to excellent inter-observer agreement (ICC>0.60), compared to FB-SPGR with four (Table 2).
Discussion
The overall image quality of UTE in the pediatric pelvis was preferred more than those of BH-SPGR and FB-SPGR. UTE demonstrated superior qualitative SNR and fewer artifacts (Figure 1), although UTE had inferior contrast compared to BH-SPGR. The image quality of multiplanar reconstructions was not assessed in our study, but it would be expected that UTE and FB-SPGR are more amenable due to the thinner acquired slice thicknesses (Figure 2).
Current uses of UTE predominate in musculoskeletal MRI due to its ability to image structures with short T2 properties, such as cortical bone and fibrocartilage [5-7]. UTE has also demonstrated value in the head, chest, and liver [8-10]. Our study establishes that UTE is feasible in the evaluation of the pediatric pelvis for suspected appendicitis. The anatomic delineation of the bladder, colon, and small bowel (in addition to the appendix) with UTE is comparable to that of BH-SPGR and superior to that of FB-SPGR; future research to assess UTE in the evaluation of pathology of these pelvic structures may be considered. Also, given that it yields decreased respiratory motion artifact, UTE may demonstrate value in the abdomen.
The limitations of our study include its unequal distribution of patients when timing the FB-SPGR and UTE sequences. FB-SPGR was performed before UTE in 82% of our patients, yielding better image quality, anatomic delineation, and diagnostic confidence during that earlier phase of contrast compared to FB-SPGR performed after UTE. Despite this disparity that biased the study towards FB-SPGR, our study rated UTE superior to FB-SPGR.
Conclusion
UTE in the evaluation of the pediatric pelvis for suspected appendicitis is feasible, yielding better qualitative SNR and fewer artifacts than both BH-SPGR and FB-SPGR.Acknowledgements
This work is supported by NIBIB R01EB009690 and GE Healthcare.References
1. Duke E, Kalb B, Arif-Tiwari H, et al. A systematic review and meta-analysis of diagnostic performance of MRI for evaluation of acute appendicitis. AJR 2016; 206(3); 508-517.
2. Koning JL, Naheed JH, Kruk PG. Diagnostic performance of contrast-enhanced MR for acute appendicitis and alternative causes of abdominal pain in children. Pediatr Radiol 2014; 44: 948-955.
3. Rosines LA, Chow DS, Lampl BS, et al. Value of gadolinium-enhanced MRI in detection of acute appendicitis in children and adolescents. AJR 2014; 203(5): 543-548.
4. Zucker EJ, Cheng JY, Haldipur A, et al. Free-breathing pediatric chest MRI: Performance of self-navigated golden-angle ordered conical ultrashort echo time acquisition. J Magn Reson Imaging 2017; doi: 10.1002/jmri.25776.
5. Chang EY, Du J, Chung CB. UTE Imaging in the Musculoskeletal System. J Magn Reson Imaging 2015; 41(4); 870-883.
6. Siriwanarangsun P, Statum S, Biswas R, et al. Ultrashort time to echo magnetic resonance techniques for the musculoskeletal system. Quant Imaging Med Surg. 2016; 6(6): 731-743.
7. Serai SD, Laor T, Dwek JR, et al. Feasibility of ultrashort TE (UTE) imaging of children at 1.5 T. Pediatr Radiol 2014; 44(1); 103-108.
8. Shu SH, Cao Y, Lawrence TS, et al. Quantitative characterization of ultrashort echo (UTE) images for supporting air-bone separation in the head. Phys Med Biol 2015; 60(7): 2869-2880.
9. Ohno Y, Koyama H, Yoshikawa T, et al. Pulmonary high-resolution ultrashort TE MR imaging: Comparison with thin-section standard- and low-dose computed tomography for the assessment of pulmonary parenchyma diseases. J Magn Reson Imaging 2016; 43(2): 512-532.
10. Doyle EK, Toy K, Valdez B, et al. Ultra-short echo time images quantify high liver iron. Magn Reson Med 2017; doi: 10.1002/mrm.26791.
11. Gurney PT, Hargreaves BA, Nishimura DG. Design and analysis of a practical 3D cones trajectory. Magn Reson Med 2006; 55(3); 575-582.
Figures
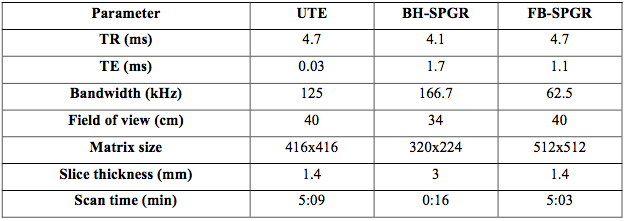
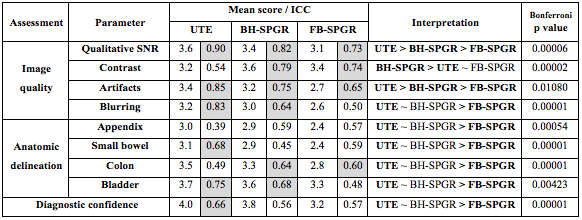

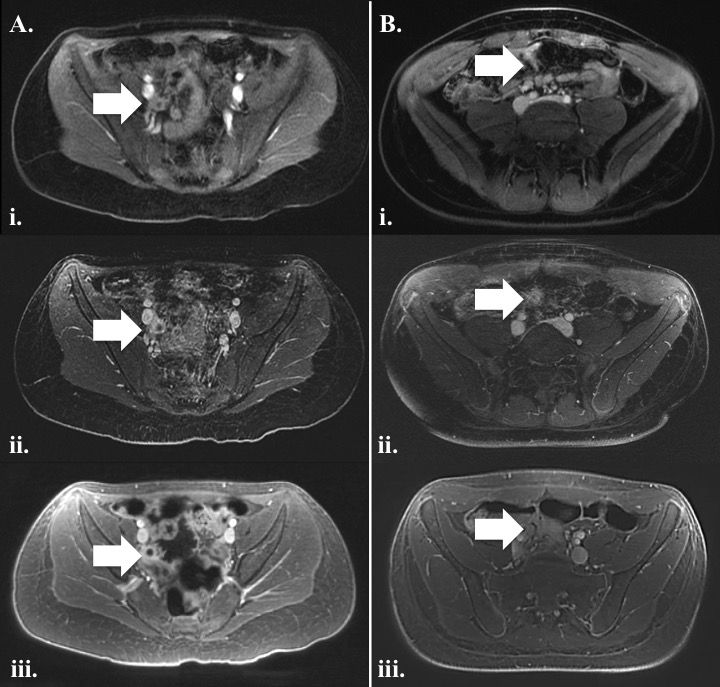
Figure 1: Two representative cases of A. acute appendicitis and B. normal appendix labeled on each sequence with white arrows. Note reduced bowel gas related field inhomogeneity artifact and decreased respiratory motion artifact on UTE.
i. BH-SPGR; ii. FB-SPGR; iii. UTE
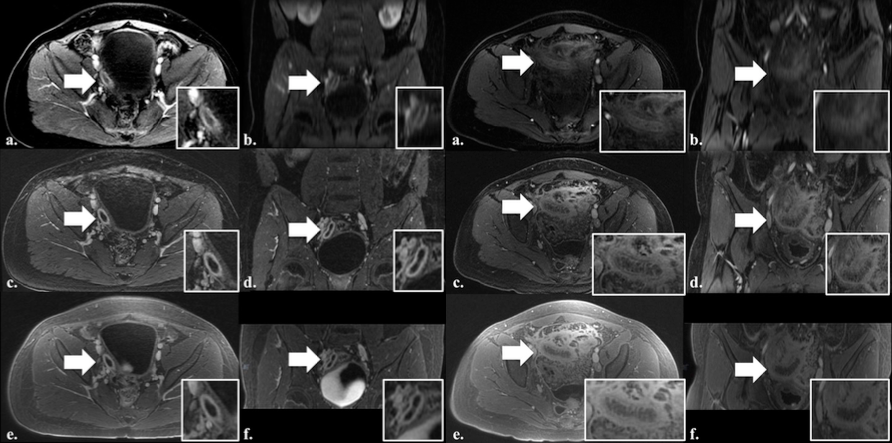
Figure 2: Two representative cases of acute appendicitis labeled on each sequence with white arrows. Note the improved image quality of the coronal reconstructions on FB-SPGR and UTE.
a. BH-SPGR in the axial plane; b. BH-SPGR in the coronal plane; c. FB-SPGR in the axial plane; d. FB-SPGR in the coronal plane; e. UTE in the axial plane; f. UTE in the coronal plane