4706
Optimal combinations of b-values in computed DWI for pancreatic cancer detection1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University Graduate School of Medicine, Kyoto, Japan, 2Human Brain Research Center, Kyoto University Graduate School of Medicine, Kyoto, Japan
Synopsis
There has been no previous report on the optimal combinations of b-values to obtain computed DWI (cDWI) with b-values above 1000 s/mm2 to evaluate pancreatic cancer. This retrospective study involved 30 pancreatic cancer patients with tumor associated pancreatitis. We aimed to evaluate the optimal combination of b-values to obtain cDWI with b-value of 1500 s/mm2 from the combinations of b-values between 0 and 500 s/mm2 (cDWI0-500), 0 and 1000 s/mm2 (cDWI0-1000), 500 and 1000 s/mm2 (cDWI500-1000), and all b-values (cDWIALL). Only cDWI0-1000 demonstrated statistically higher tumor detectability compared to measured DWI, while image quality was preserved in cDWI0-1000 and cDWIALL.
Introduction
The utility of computed diffusion weighted image (cDWI) for the detection of pancreatic cancer has been reported [1]. However, the optimal combination of b-values remains unclear as the material to obtain cDWI with high b-values to detect pancreatic cancer [2]. The aim of this study was to evaluate the optimal combination of b-values to obtain cDWI in pancreatic cancer patients with tumor associated pancreatitis regarding tumor detectability and total image quality.Method
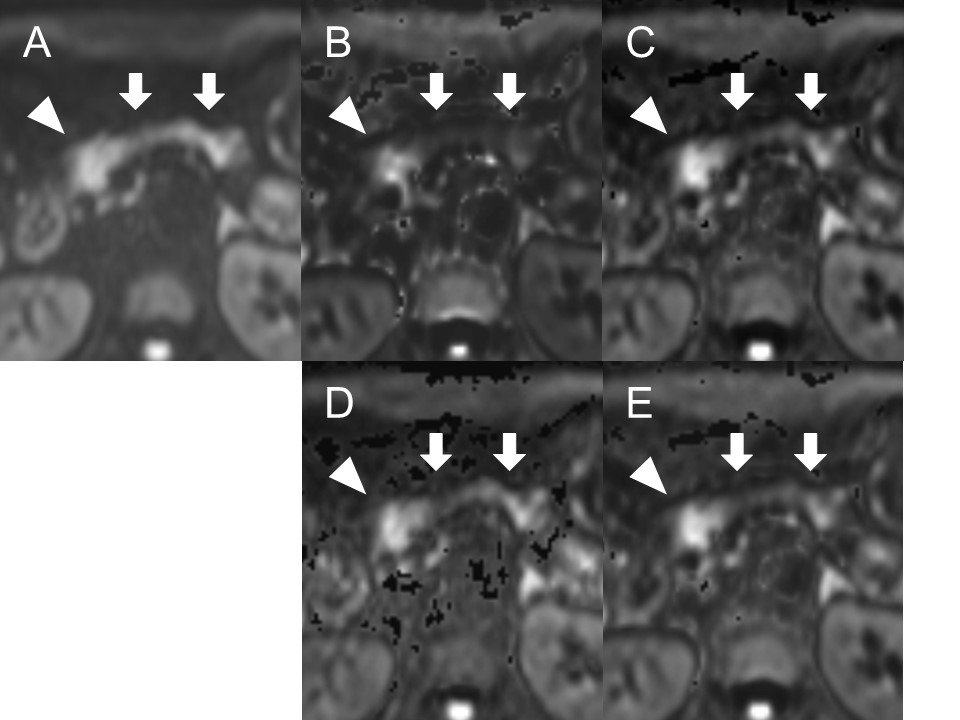
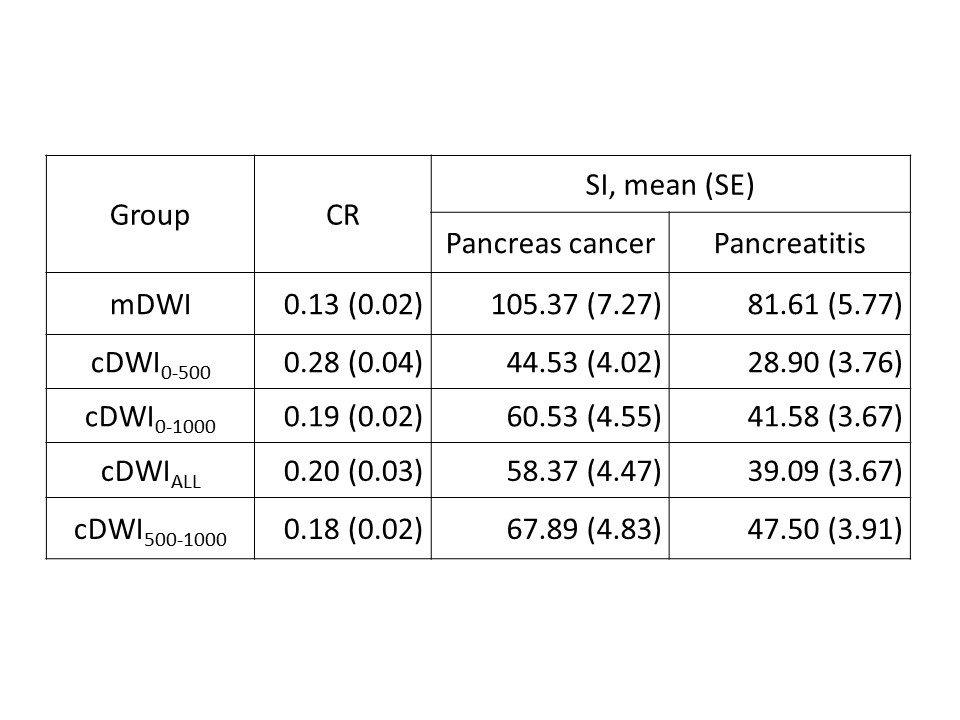
This retrospective study involved 30 consecutive pancreatic cancer patients with tumor associated pancreatitis (18 men, 12 women; range 49-88 years). The diagnosis of pancreatitis was confirmed with contrast-enhanced computed tomography based on criteria used in the literature [3]. MR studies were performed using 3.0 T MR units (Magnetom Prisma, or Skyra; Siemens Medical Solutions, Erlangen, Germany) equipped with spine matrix coil and body matrix coil. Diffusion weighted images were obtained with b-values of 0, 500, and 1000 s/mm2 using a single-shot spin-echo echo-planar imaging sequence in axial plane in respiratory gate. cDWI with b-value of 1500 s/mm2 was obtained from combinations of b-values between 0 and 500 s/mm2 (cDWI0-500), 0 and 1000 s/mm2 (cDWI0-1000), 500 and 1000 s/mm2 (cDWI500-1000), and all b-values (cDWIALL) using an in-house script written with MATLAB (R2013b, The MathWorks, Natick, MA, USA). Qualitatively, tumor detectability and the total image quality was evaluated in all cDWIs with the reference to measured DWI (mDWI) with b-value of 1000 s/mm2 using a 4-point scale: 1, poor to 4, excellent. Quantitatively, contrast ratios (CRs) of cancer and pancreatitis was calculated from the signal intensity (SI) of tumor and pancreatitis (CR = | (SICancer – SIPancreatitis) / (SICancer + SIPancreatitis) |). Apparent diffusion coefficient (ADC) of the tumor and pancreatitis were measured. Steel-Dwass test were used to compare parameters between the combinations. Results were considered statistically significant at a p value of <0.005 regarding Bonferroni’s correction.Results
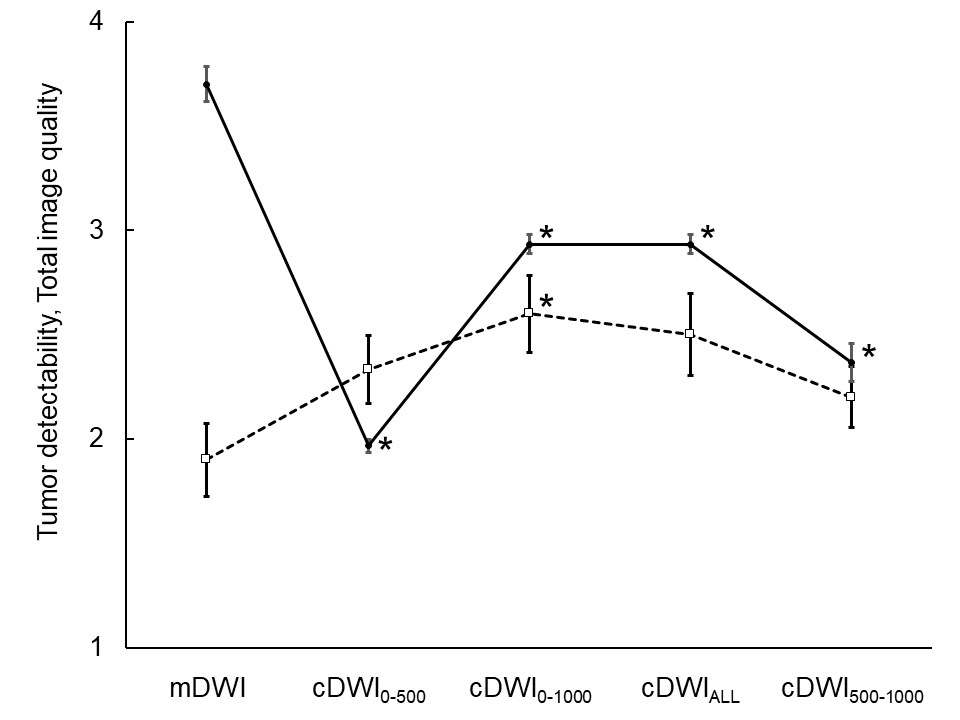
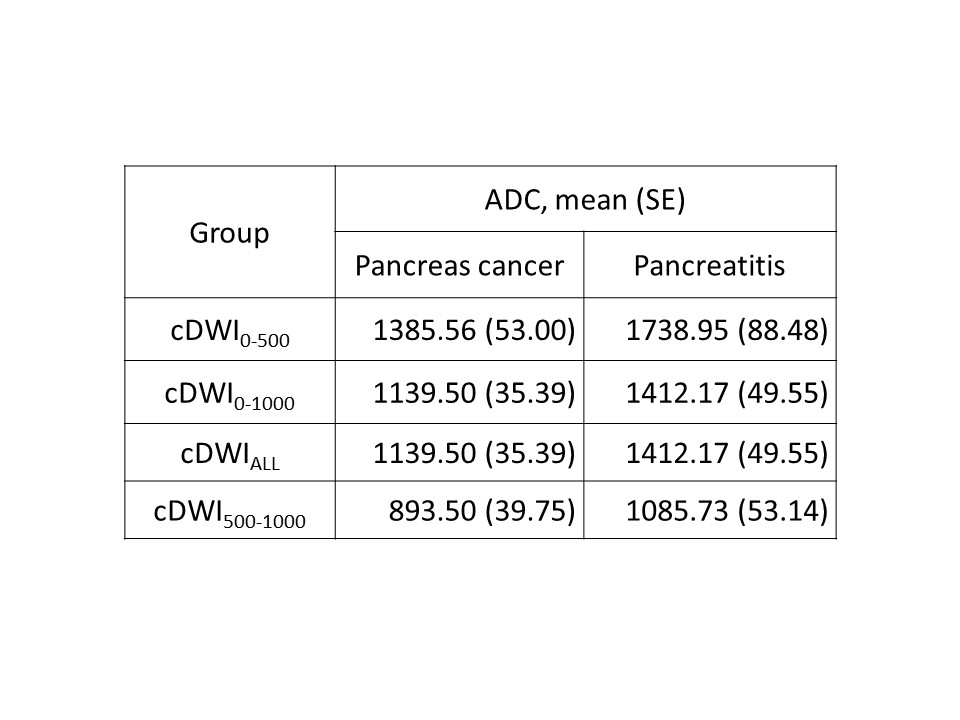
All cDWI groups showed higher tumor detectability compared to mDWI (Fig.1), but only cDWI0-1000 showed statistical significance (p<0.0001). All cDWI groups presented lower total image quality than mDWI; among cDWIs, cDWI0-1000 and cDWIALL demonstrated higher quality compared to the other two combinations within the cDWIs (p<0.0001) (Fig.2). All cDWI groups improved in CR compared to mDWI, while SI of the tumor decreased in all groups (Table.1). Among them, cDWI0-500 showed highest CR and ADC with lowest SI, cDWI500-1000 showed lowest CR and ADC with highest SI. cDWI0-1000 and cDWIALL demonstrated same ADC (Table.2).Discussion
As far as we know, this study is the first report to investigate the optimal combination of the b-values to obtain cDWI. Our result showed the combination of b-values of 0 and 1000 s/mm2 was optimal for the detection of pancreatic cancer within tumor associated pancreatitis.
The signal intensity on DWI exponentially attenuates with b-value based on a measured ADC value. Therefore, cDWI is a technique to generate high b-valued DWI by extrapolating decaying signal with DWI which was obtained by actual scan [4].
All combinations of the cDWIs presented higher tumor detectability with higher CR compared to mDWI. Within the cDWIs, cDWI500-1000 showed low tumor detectability because of the small CR. However, cDWI0-500 demonstrated the worst tumor detectability despite the best CR. This could be explained with the signal model, that higher ADC induces rapid increase of CR and decrease of SI when b-value rises. Therefore, cDWI0-500 showed the lowest total image quality due to lowest SI, which results in low tumor detectability.
Tumor detectability in cDWI0-1000 was slightly higher than cDWIALL, despite the same ADC. This can be explained by the downward deviation of the whole signal model, from the influence of mDWI with b-value of 500 s/mm2. However, the influence of mDWI with b-value of 500 s/mm2 was not so large enough to lower total image quality.
Introduction of this concept into the clinical settings may help to improve diagnosability and/or early diagnosis of pancreatic cancer, by adding cDWI to routine abdominal MRI study.
There were some limitations in our study. First, the sample size was small. Second, since this was a retrospective study, mDWI with b-values of 50-200 s/mm2 are missing, which could be important when creating more precise signal model considering several parameters such as intravoxel incoherent motion.
Conclusion
cDWI with b-value of 1500 s/mm2 is useful for the detection of pancreatic cancer within tumor associated pancreatitis. The combination of b-values between 0 and 1000 s/mm2 is suitable throughout the combinations of the b-value as the material for tumor detectability.Acknowledgements
The authors have no potential conflict of interest related to this presentation.References
1. Fukukura Y, Kumagae Y, Hakamada H, et al. Computed diffusion-weighted MR imageing for visualization of pancreatic adenocarcinoma: Comparison with acquired diffusion-weighted imaging. Eur J Radiol 2017; 95(10): 39-45.
2. Ueno Y, Takahashi S, Ohno Y, et al. Computed diffusion-weighted MRI for prostate cancer detection: the influence of the combinations of b-values. Br J Radiol 2015; 88(1048): 20140738.
3. Bollen TL, Singh VK, Maurer R, Repas K, van Es HW, Banks PA, Mortele KJ. Comparative evaluation of the modified CT severity index and CT severity index in assessing severity of acute pancreatitis. Am J Roentgenol (AJR) 2011;197(8):386-392.
4. Blackledge MD, Leach MO, Collins DJ, Koh DM. Computed diffusion-weighted imaging may improve tumor detection. Radiology 2011;261(2):573-581.
Figures