4700
Magnetic Resonance Elastography and model diffusion-weighted imaging of Autoimmune Pancreatitis: A Preliminary Study1Shengjing Hospital of China Medical University, ShenYang, China, 2Philips Healthcare China, Beijing, China
Synopsis
Autoimmune pancreatitis (AIP) is a benign process characterized by lymphoplasmacytic infiltration and massive fibrosis.
Introduction
AIP is a type of rare pancreatic disease AIP patients often present with painless jaundice and focal enlargement of the pancreas, mimicking a real pancreatic cancer (PC). As AIP responds dramatically to steroid therapy, the preoperative diagnosis of AIP is of the utmost importance in order to obviate the need for surgical resection.1 Novel magnetic resonance imaging techniques, such as MR elastography (MRE) and intravoxel incoherent motion model diffusion-weighted imaging (IVIM-DWI) with multiple b-values, have shown potentials on detecting fibrosis, inflammation and molecular diffusion of water in both PC and AIP.2 We hypothesize that MRE and IVIM-DWI might aid the establishment of AIP diagnosis. Hence, this study was to clarify the clinical utility of both MRE and IVIM-DWI for differentiating AIP from PC and healthy pancreas.Method and materials
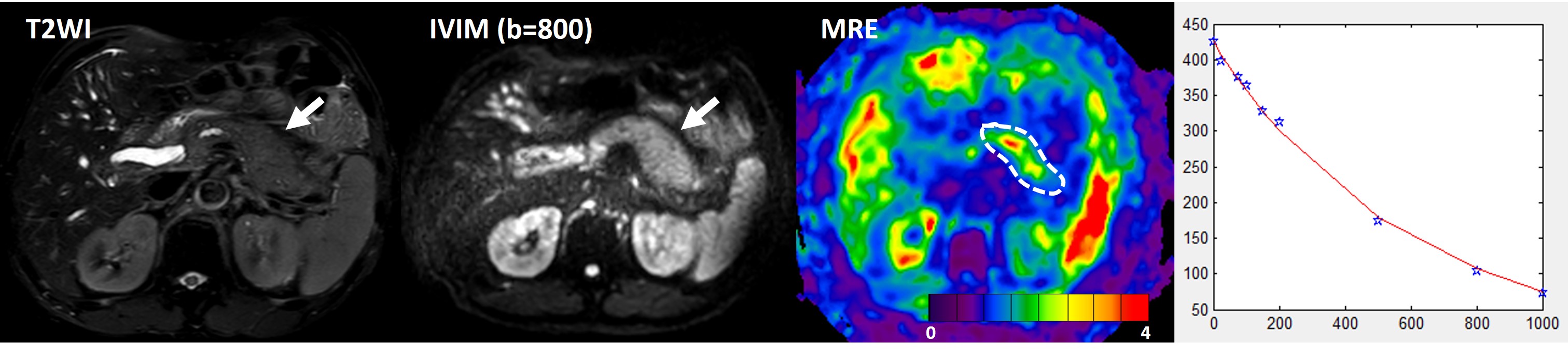
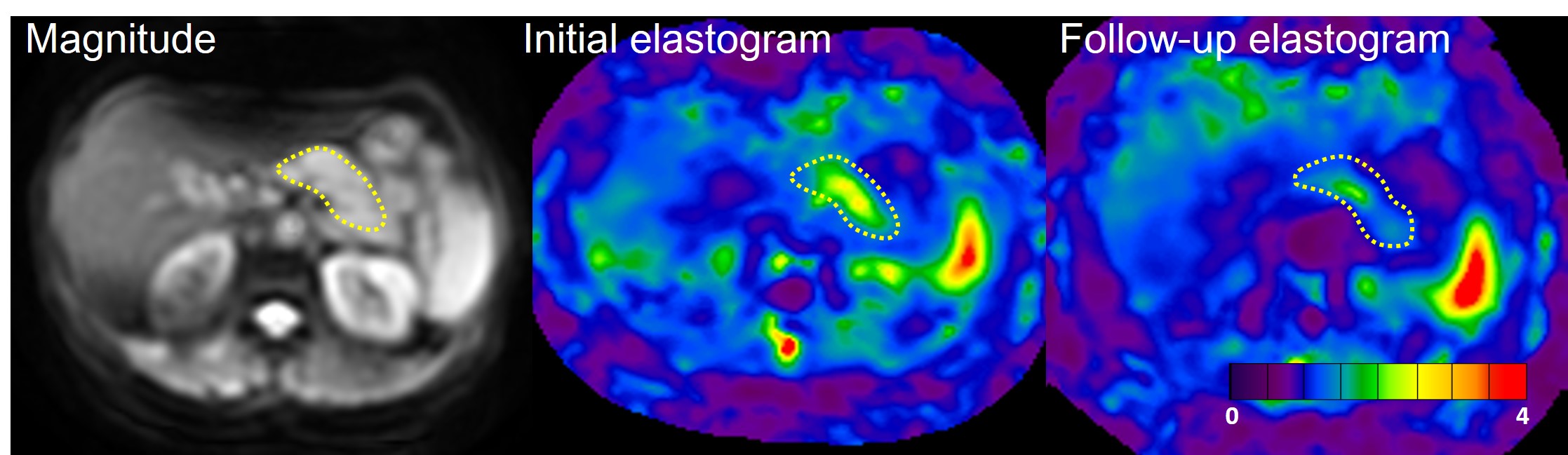
Fourteen AIP patients, 14 PC patients and 10 healthy volunteers were retrospectively collected, with examination of both MRE and IVIM-DWI. All AIP patients underwent MRE before steroid therapy and 7 of 14 underwent MRE both before and after therapy.. Both pancreatic stiffness values and IVIM-drived parameters including D (true diffusion coefficient), f (perfusion fraction), D* (pseudo diffusion coefficient) were calculated in all subjects. Receiver operating characteristic (ROC) analysis was performed for differentiating AIP from healthy pancreas and from PC. The patients first performed clinical MR sequences with IVIM-DWI on a 3.0T Philips scanner (Philips Ingenia, Philips Healthcare, the Netherlands) and then MRE on a 3.0T GE scanner (GE Healthcare, Signa EXCITE HD). IVIM-DWI was obtained using a single-shot echo-planar imaging (SE-EPI) sequence with nine b-values (0, 25, 75, 100, 150, 200, 500, 800, 1000 mm2/s). MRE images were acquired by another SE-EPI sequence with 32 slices at 40Hz. The other imaging parameters for MRE were as follows: TR/TE: 1375/38.8ms; field of view: 350-420 mm; matrix size: 96 × 96; slice thickness: 3.5 mm; phase offsets: 3.Results
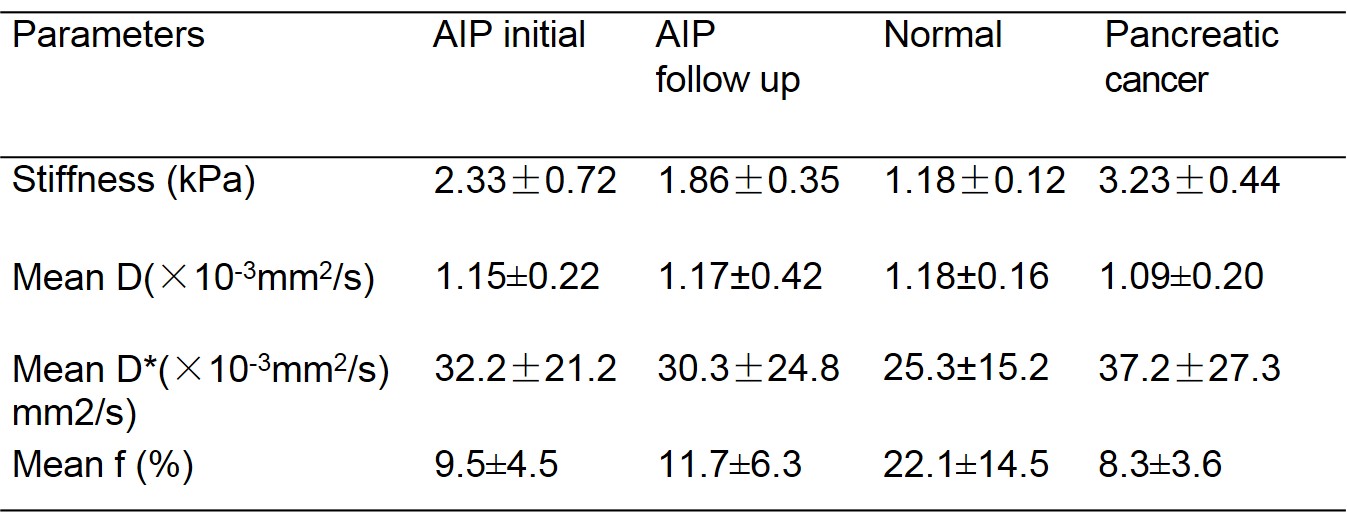
Both AIP and PC were detected as high-stiffness areas. The high-stiffness areas were diffuse (n = 5), solitary (n= 6), and multiple (n = 3) in AIP cases, and solitary in 13 PC cases except for 1 diffuse case (P < 0.001). A nodular or irregular shape (n = 9) was significantly more frequent in PC, and a longitudinal shape (n = 7) was more frequently found in AIP (P = 0.005). f was the only value where we found significant differences by IVIM, with significantly lower value in AIP than that of healthy pancreas (9.5±4.5 % vs. 22.1±14.5 %, P<0.001). The f, D and D* between PC patients and AIP did not reach statistical significance (all P>0.05). The normal stiffness in pancreas was 1.18±0.12kPa, significantly lower than the stiffness of AIP (2.33±0.72kPa) and PC (3.23±0.44kPa). ROC analysis showed that the AUC of stiffness and f-value for differentiation of PC from initial AIP was 0.85 and 0.72 (P<0.05), for differentiation of PC from AIP after therapy were 0.92 and 0.79 (P<0.001), and for initial AIP from healthy pancreas were 0.99 vs 0.91 (P=0.02), respectively.Discussion
A major clinical challenge in the management of AIP is the initial establishment of the correct diagnosis. Both stiffness and perfusion fraction showed differences in AIP and healthy pancreas, and the stiffness was the only parameter for significant difference between PC and initial AIP. In AIP, the acinar cell structures are replaced by inflammatory cells and fibrosis, leading to reduced density of capillaries.3 PCs are also hypovascular and desmoplasitc.4 When compared with healthy pancreas, the effects of inflammation, fibrosis and perfusion changes may explain the reduced perfusion fraction f and higher stiffness in both AIP and PC patients. However, f showed little difference in comparing initial AIP and PC, showing similar changes of perfusion in these diseases. The stiffness of PC was significantly higher than that of AIP, this might be explained by different amount and pattern of fibrosis, with more acinar fibrosis in AIP and massive fibrosis in PC.Conclusions
Both MRE and IVIM-DWI are promising imaging methods for distinguishing AIP from healthy pancreas, and MRE is more useful for distinguishing between AIP and PC and for therapy monitoring. Compared with IVIM-DWI, MRE is more convenient, intuitive and accurate.Acknowledgements
We thank Richard Ehman and Kevin Glaser from the Mayo Clinic for providing the MRE system. We also thank Jun Chen from the Mayo Clinic for his assistance with providing the tailored pancreatic MRE driver. This work was supported by a grant from the National Natural Science Foundation of China (No. 81771893, 81771802 and NIH EB1801).References
1. Klauss M, Maier-Hein K, Tjaden C, et al. IVIM DW-MRI of autoimmune pancreatitis: therapy monitoring and differentiation from pancreatic cancer[J]. Eur Radiol, 2016, 26(7): 2099-2106.
2. Kim B, Lee SS, Sung YS, et al. Intravoxel incoherent motion diffusion-weighted imaging of the pancreas: Characterization of benign and malignant pancreatic pathologies[J]. J Magn Reson Imaging, 2017, 45(1): 260-269.
3. Dong Y, D'Onofrio M, Hocke M, et al. Autoimmune pancreatitis: Imaging features[J]. Endosc Ultrasound, 2017.
4. Schober M, Jesenofsky R, Faissner R, et al. Desmoplasia and chemoresistance in pancreatic cancer[J]. Cancers (Basel), 2014, 6(4): 2137-2154.
Figures