4668
Functional Connectivity changes during Real-time fMRI based Neuro-rehabilitation of post-stroke Aphasic Patients.Sujesh Sreedharan1, Arun K. M.1, Sylaja P. N.2, Ranaganatha Sitaram3, and Kesavadas C.1
1Imaging Sciences and Interventional Radiology, SCTIMST, Trivandrum, India, 2Neurology, SCTIMST, Trivandrum, India, 3Department of Psychiatry and Division of Neuroscience, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
Recovery from stroke to lead an improved life is one of the most sought after rehabilitation programs around the globe. Various factors are involved in the process of restoration of an impaired function. The study examined the functional network disruption due to stroke and the network changes happening during the real-time fMRI based neurofeedback training for aphasic stroke survivors to retrain the language areas. The results show that though the contralateral hemisphere for test group has strong connections when compared with controls, and with training the ipsilateral connections are strengthened and are recovering through alternate connections.
Introduction
Rehabilitation in stroke helps survivors relearn skills that are lost when part of the brain is damaged1,2. A carefully directed, well-focused, repetitively practiced rehabilitation regime is highly desired for the compensation or recovery from the deficits3. A real-time fMRI (rt-fMRI) based neuro-feedback training was performed to modulate neural activity of language areas in post-stroke aphasic patients. The effect of this intervention is studied using the functional connectivity (FC) changes in the network of language areas and the associated structures. The objective was to study: (i) the effect of stroke on FC in a limited area of the brain including language areas, (ii) the alteration of brain networks during up-regulation activity during training, and (iii) the brain networks strengthened due to the training and associated language recovery.Methods
Twelve subjects were recruited for the study. The subject group included four experimental and four control patients, all with Broca’s aphasia and four healthy volunteers. The study was designed as sessions having alternating baseline and up-regulation epochs. The first session is a pre-test session which also includes a naming task after each baseline and up-regulation epoch. The next four sessions are neuro-feedback training sessions which do not have any testing task. The last session is a post-test session which is a repetition of the pre-test. For controls the experiment is conducted having only the pre-training and post-training sessions and skipping the four training sessions. The regions of- interest (ROIs) chosen for the study included the Broca’s and Wernicke’s areas and its right homologues, and eleven other ROIs surrounding the Broca’s and Wernicke’s areas (restricted to each patient’s active region during an SPM T-statistic map of p <0.01).The connectivity analysis was performed on data preprocessed using SPM8 toolbox. The preprocessing involved realignment, coregistration of anatomical scan, normalization and smoothing. This data was then analyzed using the CONN toolbox4. The measure used for functional connectivity is the bivariate correlation between ROIs. The connectivity matrix obtained for the healthy group is then analyzed for modularity and subsequently grouped into the six modules in the left hemisphere as shown in Figure 1. These modules are restricted to the left hemisphere (LH) and six other analogous modules are generated for the right hemisphere (RH) as well using the AAL markers. Table 1 describes the areas covered in each module. Twelve modules so generated are analyzed for functional connectivity changes. The inter-modular connections are found by summing the connectivity from each ROI of one module to that of the other module. The modular connectivity is then plotted for various conditions using BrainNet viewer.Results and Discussion
The study evaluated inter subject group and inter condition comparisons in the functional connectivity changes among the modules defined above. Inter modular connections for the test group is compared with the control groups as well as healthy volunteers to understand the changes in network organization. Healthy volunteers at rest when compared to test patients have shown a stronger inter-hemispheric connection between CO modules and between FL and TL modules in the LH. They are indicative of weakened connections due to aphasic stroke for the test group. In healthy group the FL and TL module connections are observed to strengthen most due to neurofeedback training over the sessions (Figure 2). In the test patient group the intra-hemispheric connections involving FL, SP, CO and TL modules are getting strengthened over the training sessions. Connections to right hemispheric SP and CO modules are also seen. TL module is not directly connected to FL module in the LH, and only indirectly through CO and SP modules as opposed to direct connection in case of healthy volunteers. The effect of training in test patients was further studied by comparing the final sessions of the study with control group. The connections in RH are seen to strengthen most in addition to the LH connections involving FP, FL, TL and SP modules (Figure 3a & 3c).Conclusion
The results of the study explored the effect of stroke on FC in the language areas. The test patients when compared to normal have disrupted connections between the temporal and frontal language modules. The resting and language active connections are stronger on the contralateral hemisphere when compared to controls. Up regulation through neuro-feedback has been shown to increase the strength of left hemispheric connections which were disrupted due to stroke, through alternate pathwaysAcknowledgements
No acknowledgement found.References
- Smith, L. N. et al. Rehabilitation of patients with stroke: summary of SIGN guidance. BMJ 340, c2845 (2010).
- Carey, L. M. Stroke Rehabilitation: Insights from Neuroscience and Imaging. (OUP USA, 2012).
- Woldag, H. & Hummelsheim, H. Evidence-based physiotherapeutic concepts for improving arm and hand function in stroke patients: a review. J. Neurol. 249, 518–528 (2002).
- Whitfield-Gabrieli, S. & Nieto-Castanon, A. Conn: A Functional Connectivity Toolbox for Correlated and Anticorrelated Brain Networks. Brain Connect. 2, 125–141 (2012).
Figures
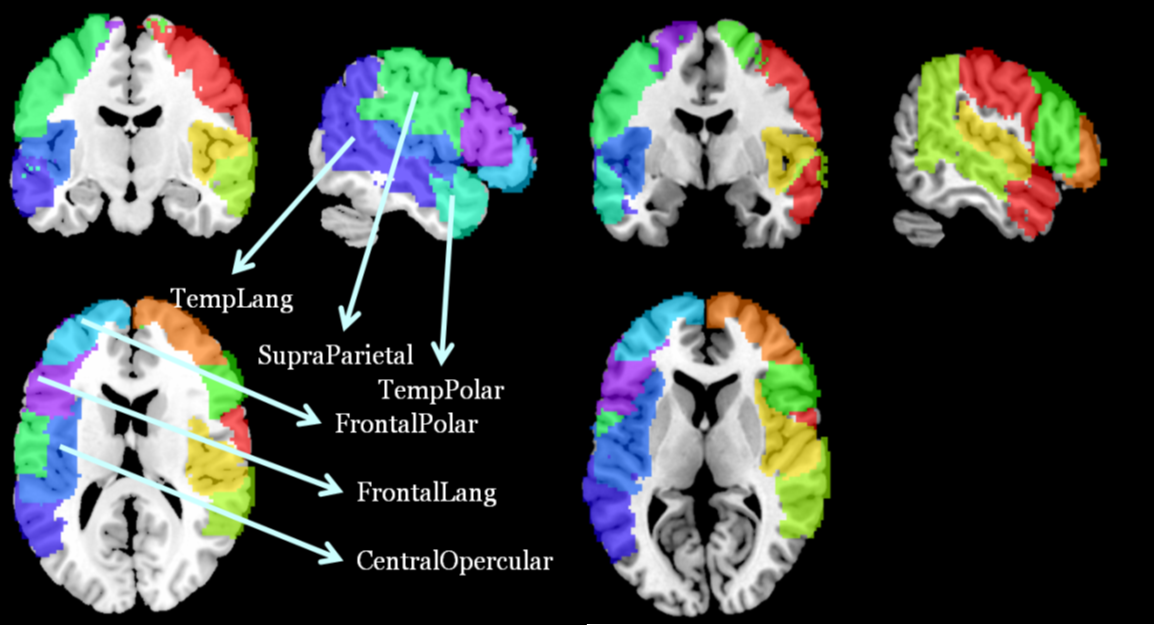
FIgure 1: Modular Sub networks for language areas
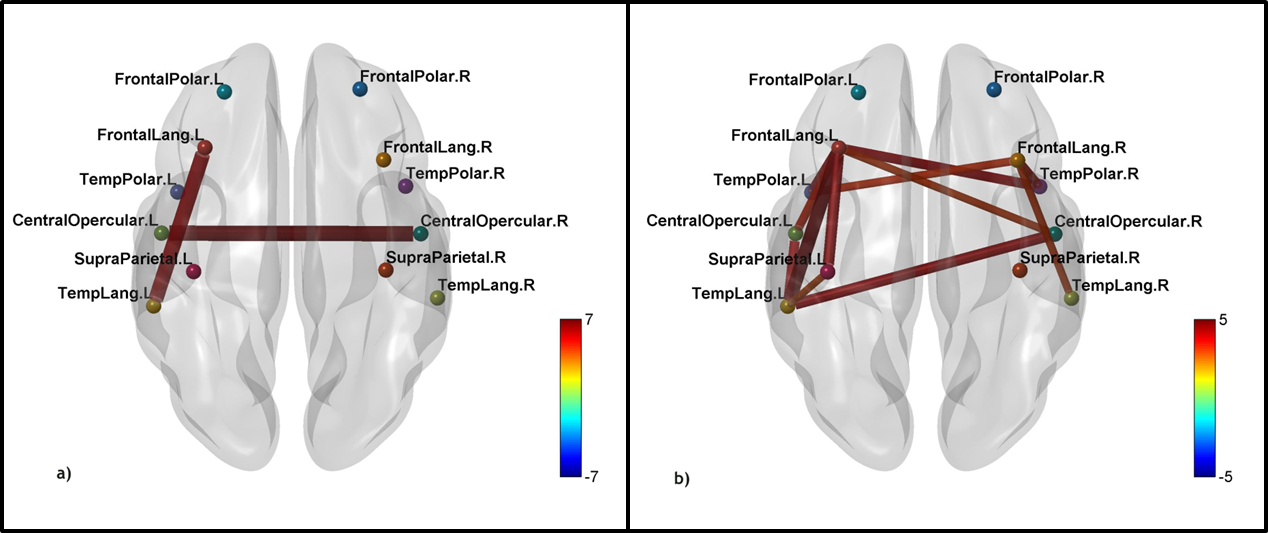
Figure 2: Connectivity changes in healthy volunteers. a)
Strongest connections at rest when compared to test patients. b) Improved
connections in healthy volunteers during neuro-feedback training. Only above 50
% of strongest connections are shown.
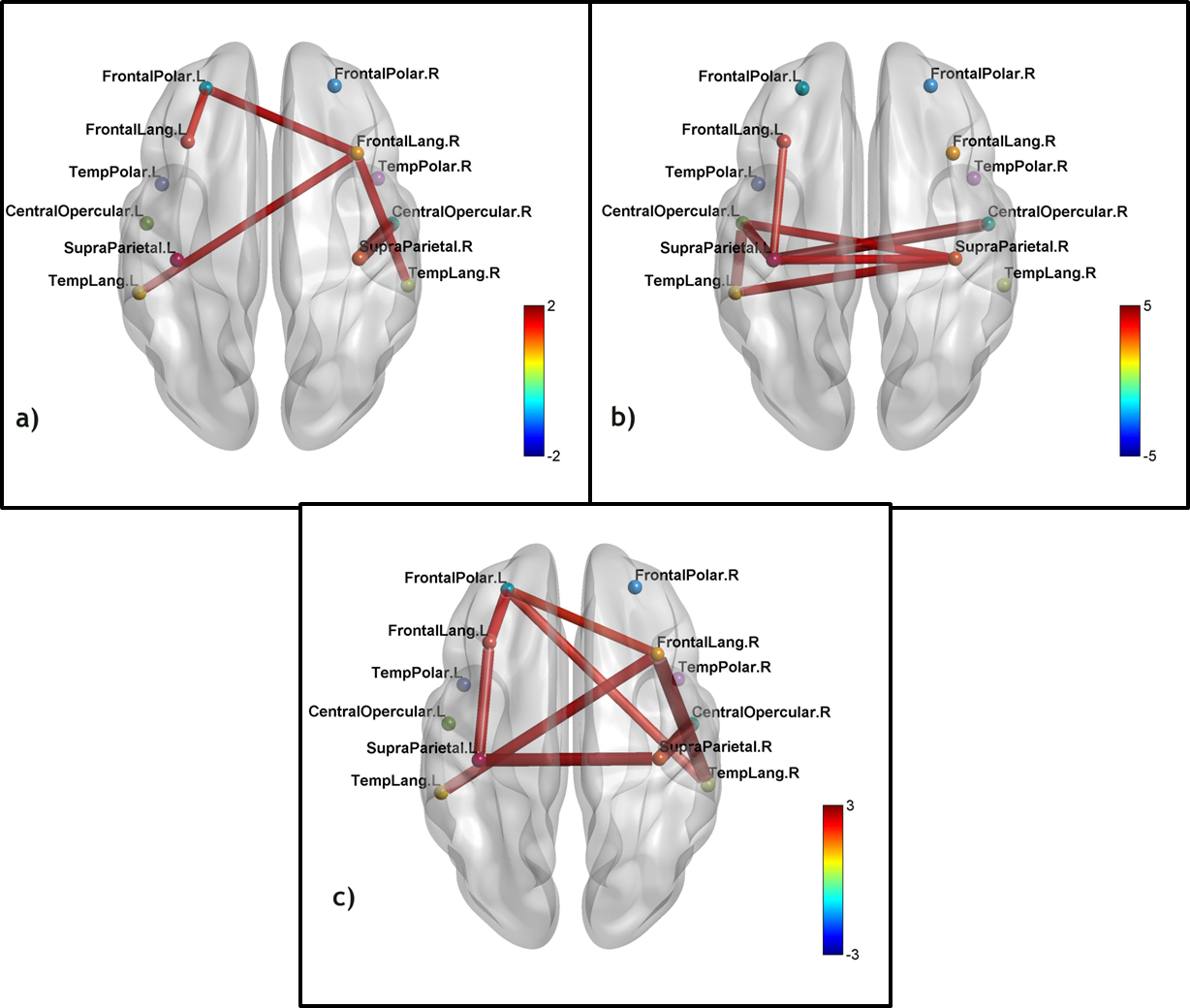
Figure 3: a) Strongest connections for test patients when
compared to control group at rest are shown. b) Connections which got
strengthened during training sessions for the test patients (2nd
half of training greater than 1st half). c) Improved left
hemispheric and right hemispheric connections for test patients after training
when compared to controls. Only 60 % of strongest connections are shown.
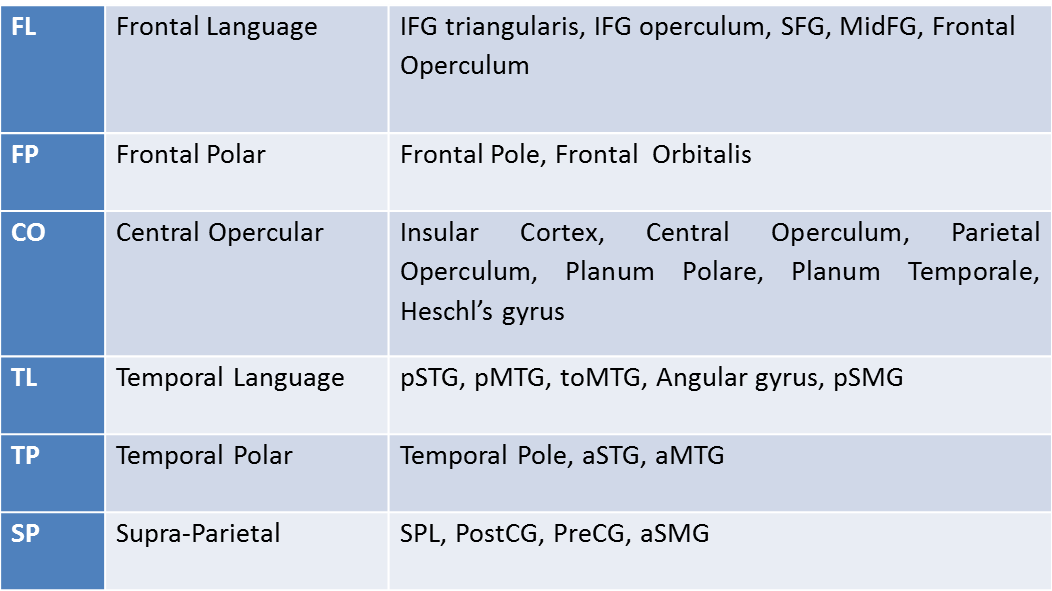
Table 1: Modular Sub networks for Language Areas –
regions forming the modules