4623
Robustness of diffusion-prepared 3D TSE for isotropic-resolution large-FOV coronal DWI of neurogenic tumors in cervical and pelvic regions1Diagnostic and Interventional Radiology, Technical University of Munich, Munich, Germany, 2Philips Healthcare, Hamburg, Germany, 3Philips MR Clinical Science, Best, Netherlands, 4Orthopaedic Surgery, Technical University of Munich, Munich, Germany
Synopsis
DWI of musculoskeletal tumors has been proposed as a non-invasive tool of potential valuable diagnostic utility. Large-FOV isotropic-resolution DWI can provide improved visualization of MSK tumors but deems particularly challenging for conventionally used DW-EPI in terms of geometric distortions and chemical-shift artifacts. 3D DW-TSE techniques can alleviate these challenges and have been shown to be useful in DWI of different body regions. The present work examines the robustness to distortions and artifacts of 3D DW-TSE in isotropic-resolution large-FOV coronal DWI of neurogenic tumors in two anatomical regions where DW-EPI is highly prone to distortion artifacts.
Purpose
Diffusion-weighted imaging (DWI) has been proposed as a potentially useful imaging technique for non-invasively assessing the cellularity of musculoskeletal tumors [1,2]. There are reports of its use in the evaluation of musculoskeletal tumors for the characterization of soft tissue masses as benign or malignant [3] or for characterizing changes after tumor resection in the resected area for evaluation of the possibility of a recurrent tumor [4]. Moreover, DWI has previously shown low diffusivity values indicating malignancy in peripheral nerve tumors [5]. The application of DWI in musculoskeletal sites has been primarily based on single-shot EPI, acquired on axial planes and with anisotropic voxel sizes. Performing single-shot DW-EPI in large FOVs (acquired on sagittal and coronal planes) and increasing its spatial resolution is challenging due to the associated large geometric distortions and severe fat-induced chemical shift artifacts. DW-TSE can alleviate the above challenges, but it has been previously combined only with 2D imaging for musculoskeletal lesion DWI [6]. 3D DW-TSE techniques have been recently emerging in DWI of different body regions [7,8]. Body regions where considerable B0 inhomogeneity is present and where coronal imaging is required, such as the cervical and pelvic regions, deem especially challenging in isotropic-resolution DWI using EPI-based techniques and are therefore of particular interest in TSE-based DWI. The purpose of the present work is to examine the robustness in terms of geometric distortions and artifacts of 3D DW-TSE for isotropic-resolution large-FOV coronal DWI of neurogenic tumors in cervical and pelvic regions.Methods
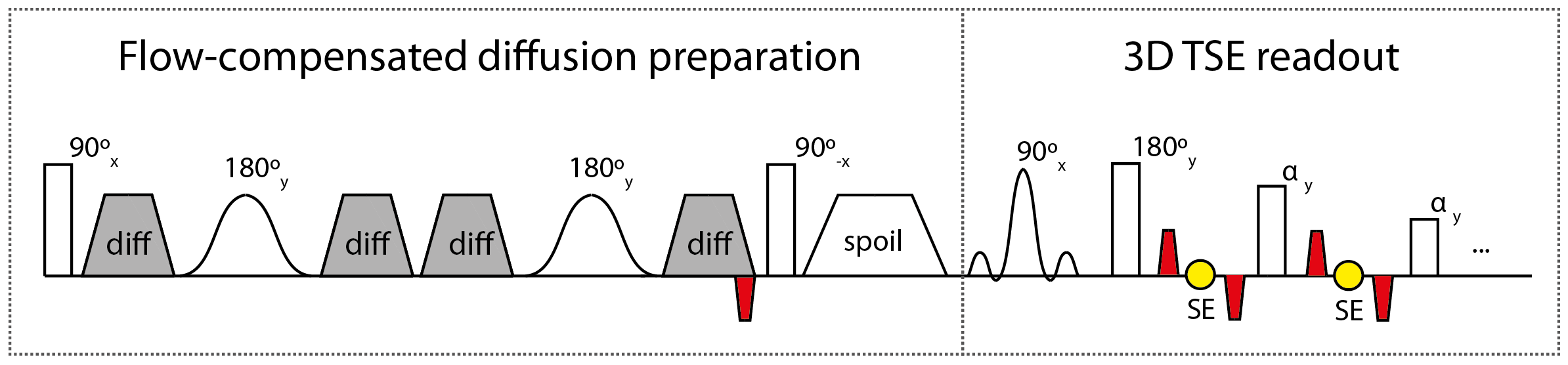
Pulse sequence: A sequence was developed (Figure 1) combining a flow-compensated diffusion preparation with a 3D TSE readout in which dephasing and rephasing gradients were added during the diffusion preparation and in the TSE readout to reduce sensitivity to phase errors [9,10,11].
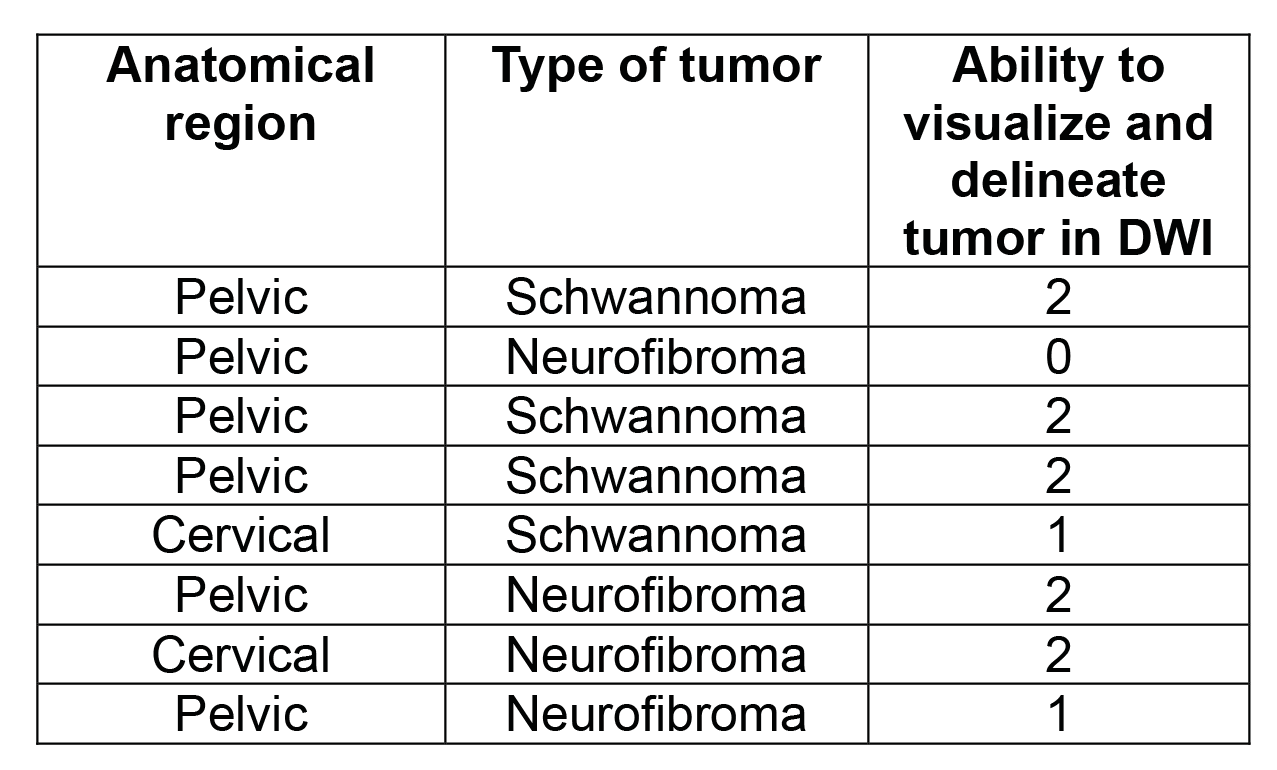
In vivo measurements: 8 subjects (4 males, 4 females, 56 ± 20 years) having either schwannoma or neurofibroma in the cervical or pelvic regions (see summary in Figure 2) were scanned using a 3T Philips system (Philips Ingenia, Best, The Netherlands). Pelvic scans used a 16-channel torso coil in conjunction with the built-in posterior coil and cervical scans used a 20-channel head-neck coil. Isotropic-resolution, large-FOV coronal DWI was performed on all subjects with the developed sequence. Cervical scans used the following sequence parameters: FOV=150×150×60mm3; acquisition voxel=2.4×2.4×2.4mm3; reconstruction voxel=0.78×0.78×1.20mm3; TR/TE=1600/33ms; TSE-factor=42; averages=2; fat suppression with SPAIR; SENSE reduction factor=1.5(RL); b-values=0,400; duration=10m32s. Pelvic scans used parameters: FOV=380×380×100m3; acquisition voxel=2.5×2.5×2.5mm3; reconstruction voxel=0.68×0.68×0.68mm3; TR/TE=1800/34ms; TSE-factor=60; averages=2; fat suppression with SPAIR; SENSE reduction factor=3(RL),1.2(AP); b-values=0,300; duration=15m12s. DWI acquisitions in all anatomies consisted of six diffusion directions to allow the possibility of DTI analysis.
Post-processing: Iso-diffusion-weighted images (iso-DWIs) were created for all subjects. For a single subject, diffusion tensors were computed using linear fitting and mean diffusivity was computed from the derived eigenvalues.
Analysis: One MR researcher with 3.5 years of experience in performing evaluations of MR neurographic studies assessed the ability to visualize and delineate the neurogenic tumors. A three-point scale was used: “0-not visible or poorly visualized/delineated”, “1-moderately visualized/delineated”, “2-well visualized/delineated”.
Results
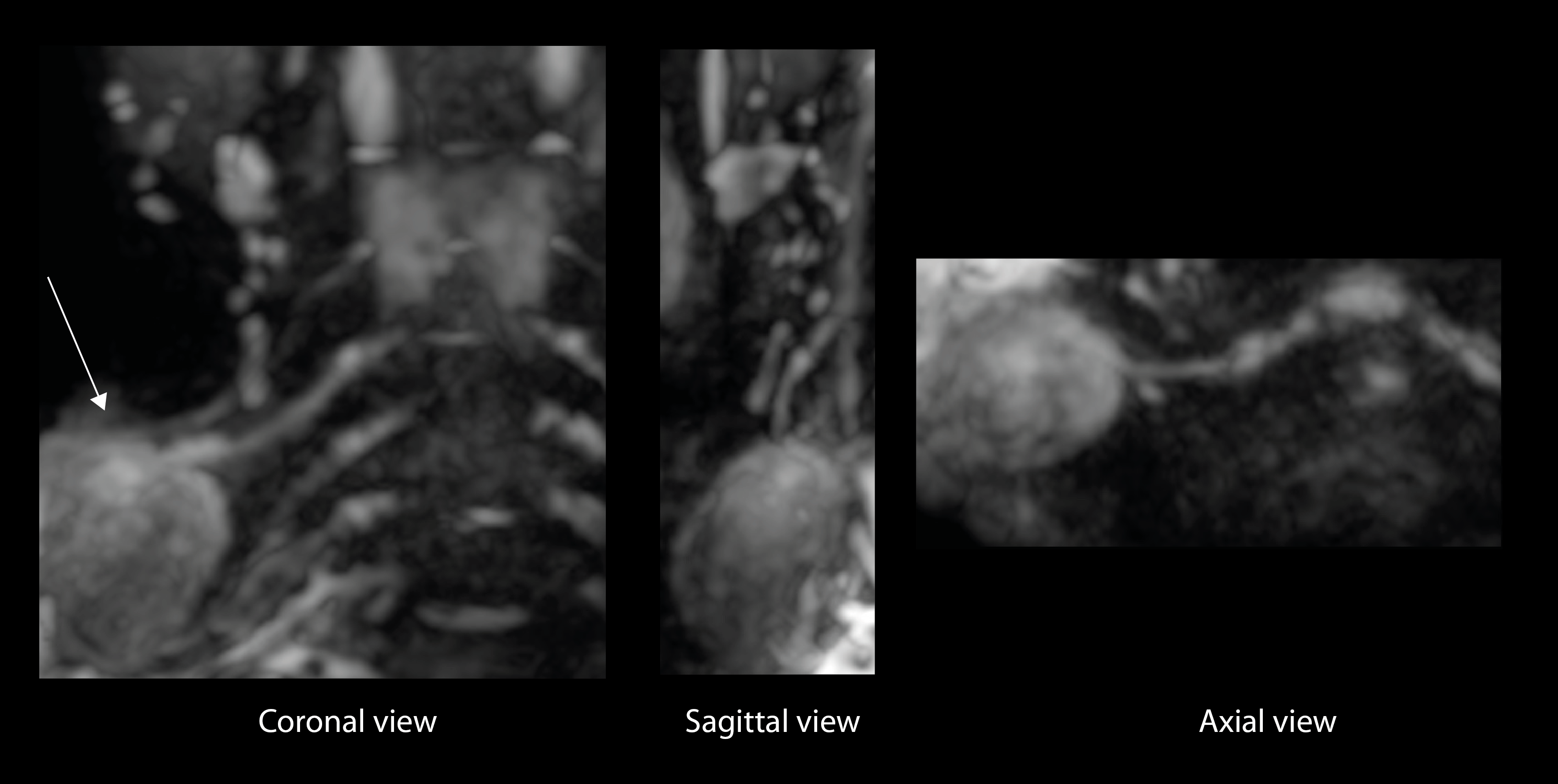
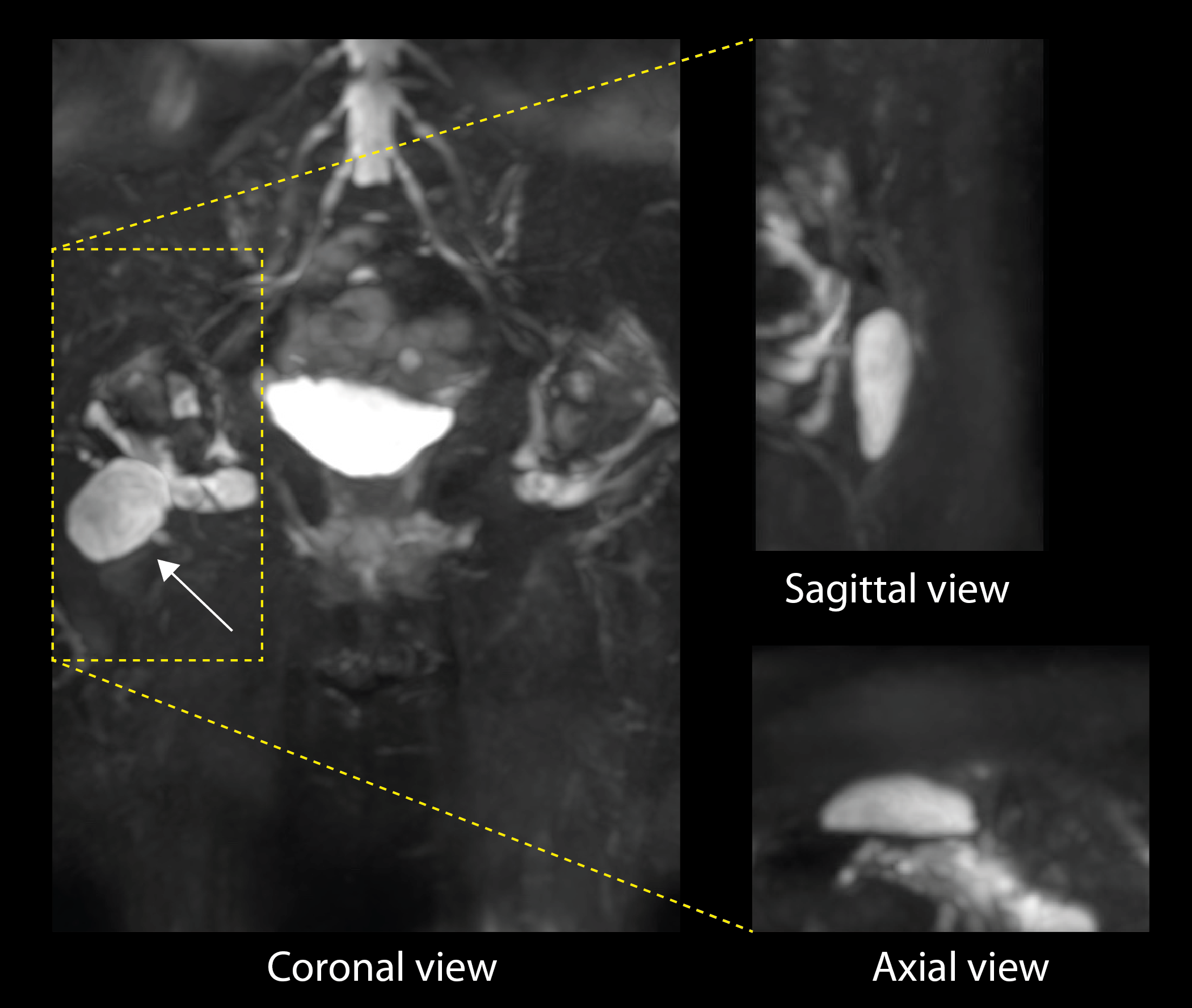
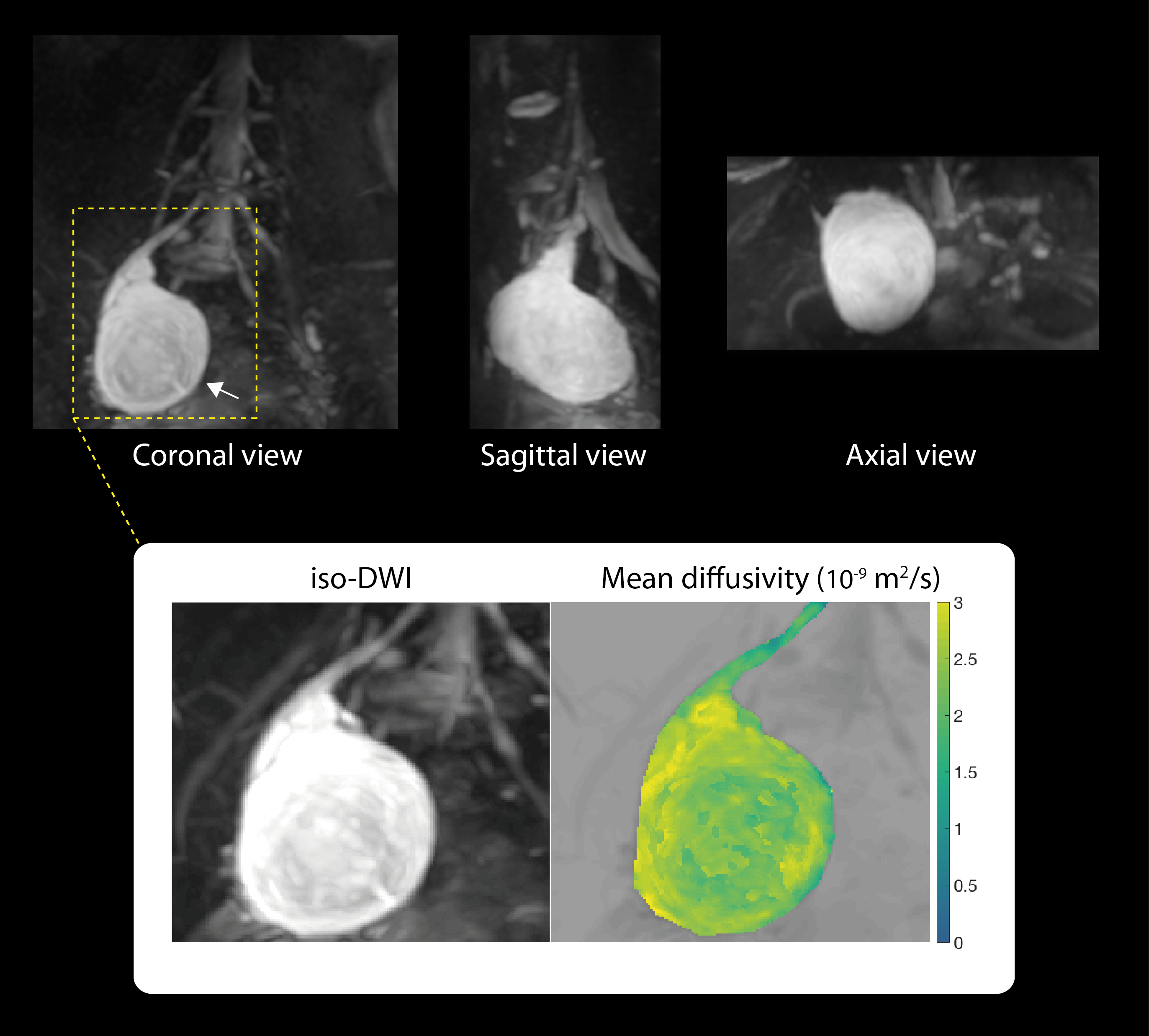
Representative iso-DWIs shown in Figures 3-5 illustrate the image quality achieved with the DW 3D TSE technique in large-FOV coronal isotropic-resolution DWI of schwannomas and neurofibromas in cervical and pelvic regions. The presented images provide distortion- and artifact-free isotropic multi-planar views clearly depicting the neurogenic tumors using diffusion contrast in regions with high geometric complexity and B0 field inhomogeneity. The evaluation of nerve conspicuity and delineation summarized in Figure 2 identified only one case where the neurogenic tumor could only be poorly visualized and two additional cases where the tumors could only be moderately delineated. The remaining five cases resulted in good visualization and delineation of the neurogenic tumors. Figure 5 also shows a mean diffusivity map of a lumbar plexus schwannoma free of artifacts allowing further assessment of tumor properties.Discussion & Conclusion
A diffusion-prepared 3D TSE sequence that allows isotropic-resolution large-FOV coronal DWI of neurogenic tumors free of distortion artifacts was demonstrated in vivo in the cervical and pelvic regions. Isotropic-resolution iso-DWIs show clear visualization of schwannomas and neurofibromas in coronal, sagittal and axial planes. The presented mean diffusivity map further demonstrates the potential for using the isotropic-resolution diffusion-weighted data acquired with DW 3D TSE for assessing diffusivity within neurogenic tumors in anatomies with complex geometries and where large coronal fields of view are needed. The present work therefore demonstrates the robustness to geometric distortions of the used DW 3D TSE sequence for isotropic-resolution large-FOV coronal DWI of neurogenic tumors in regions where EPI-based techniques are highly prone to distortion artifacts.Acknowledgements
The present work was supported by Philips Healthcare.References
[1] Subhawong, Radiographics 34:1163, 2014
[2] Fayad, Radiology 265:340, 2012
[3] Yakushiji, JMRI 4:895, 2009
[4] Baur, Eur Radiol 11:828, 2001
[5] Chhabra, AJNR 34:802, 2013
[6] Dietrich, Eur Radiol 15:772, 2005
[7] Zhang, NMR Biomed, 2017
[8] Cervantes, Proc. ISMRM 2017, p. 3935
[9] Alsop, Magn Reson Med 38:527, 1997
[10] Sinha, J Magn Reson Imaging 6:657, 1996
[11] Jeong, Magn Reson Med 56:1173, 2006
Figures