4608
High Acceleration Three Dimensional T1-weighted Dual Echo Dixon Imaging using Compressed Sensing-SENSE: Comparison of Image Quality and Solid Lesion Detectability with the Standard T1-Weighted Sequence1Seoul National University Hostpital, Seoul, Republic of Korea, 2Seoul National University Hospital, Seoul, Republic of Korea, 3Hallym University Sacred Heart Hospital, Gyeonggi-do, Republic of Korea, 4Chung-Ang University Hospital, Seoul, Republic of Korea, 5National Cancer Center, Gyeonggi-do, Republic of Korea, 6Philips Healthcare Korea, Seoul, Republic of Korea, 7Philips Research Hamburg, Hamburg, Germany
Synopsis
A total of 163 consecutive patients underwent gadoxetic acid-enhanced liver MRI at 3T with two HBP protocols using the standard mDIxon-3D-GRE technique with sensitivity-encoding method (SENSE; acceleration factor (AF): 2.8, standard mDixon-GRE) and a high acceleration mDIxon-3D GRE technique using the combined compressed sensing (CS)-SENSE technique (CS-SENSE mDixon-GRE). The consensus reading revealed no significant difference in overall image quality. CS-SENSE mDixon-GRE showed higher image noise, but less motion artifact and overall artifact levels. In terms of lesion detection, reader-averaged JAFROC figures-of-merit showed non-inferior performance of CS-SENSE mDixon-GRE over standard mDixon-GRE was confirmed (JAFROC figure-of-merits difference: 0.064 [-0.012, 0.081])
INTRODUCTION
Various research efforts had been directed toward finding ways to reduce the acquisition time of MR, including partial k-space sampling,1 parallel imaging (PI) such as sensitivity encoding (SENSE),2,3 and compressed sensing (CS).4-6 CS is a relatively new concept in MRI acquisition derived from a mathematical idea in approximation theory and information theory7-9. It focuses on the sparsity of images in a certain domain and attempts to avoid under-sampling artifacts using incoherent sampling with nonlinear reconstruction.7,9,10 CS-MR imaging offers a synergistic enhancement to PI with a built-in noise reduction, and combining the CS and PI techniques has been shown to provide better-reconstructed images than PI and partial-Fourier techniques, enabling highly accelerated imaging.5,11-13 Therefore, the purpose of this study is to determine if the CS-SENSE mDixon-3D GRE technique can offer adequate image quality and detectability of solid focal liver lesions (FLLs) in the hepatobiliary phase (HBP) of gadoxetic acid-enhanced liver MR imaging compared with the standard mDixon 3D-GRE technique.METHODS
After a preliminary study conducted with 54 consecutive patients using four HBP protocols, using standard or increased acceleration factor (AF), we applied two HBP protocols in the main study. A total of 163 consecutive patients underwent gadoxetic acid-enhanced liver MRI at 3T with HBP imaging obtained twice sequentially using the standard mDIxon-3D-GRE technique with SENSE and a high acceleration mDIxon-3D GRE technique using the combined CS-SENSE technique (CS-SENSE mDixon-GRE). Standard mDixon-3D GRE T1W imaging was obtaining using the dS-SENSE technique with an AF of 2.8 (2 in the phase-encoding direction and 1.4 in the slice encoding direction) and CS-mDixon 3D GRE T1W imaging was obtained using a total AF of 4.5 (2 in the phase-encoding direction, 1.4 in the slice encoding direction, and 1.6 extrareduction factor accomplished with the integrated CS-SENSE algorithm). Two abdominal radiologists assessed the two MR imaging data sets for image quality in consensus in a five-point-scale. Three other abdominal radiologists independently assessed the diagnostic performance of each data set in detecting solid FLLs in 117 patients with 193 solid nodules, and compared them using jackknife alternative free-response receiver operating characteristics (JAFROC).RESULTS
The consensus reading revealed no significant difference in overall image quality (p=0.663). Among all 163 patients, 4.3% (7/163) was scored as unread or poor in overall image quality for both the standard and CS-SENSE mDixon-GRE techniques. CS-SENSE mDixon-GRE showed higher image noise (standard mDixon GRE vs. CS-SENSE mDixon-GRE; 3.01±0.50 vs. 2.53±0.65, p<0.0001) and aliasing artifact (2.75±0.44 vs. 2.42±0.52, p<0.0001) but less motion artifact (3.69±0.75 vs. 3.85±0.66, p=0.005) and overall artifact levels (3.74±0.62 vs. 3.65±0.70, p=0.045) than did standard mDixon-GRE. In terms of lesion detection, reader-averaged figures of merit estimated with JAFROC was 0.918 for standard mDixon GRE and 0.953 for CS-SENSE mDixon-GRE (p=0.142) and the non-inferiority of CS-SENSE mDixon-GRE over standard mDixon-GRE was confirmed when the lower limit for the 95% CI for the difference was set as -0.1 (difference: 0.064 [-0.012, 0.081]).14,15DISCUSSION
The time resolution we applied on CS-mDixon-GRE sequence was 1.6 times faster than our standard mDixon-GRE sequence, and 2~2.4 times faster than usual breath-holding time up to 18~22 seconds in literature. Our study results showing the non-inferiority of the CS-SENSE mDixon-GRE sequence over standard mDixon-GRE sequence for detection of solid FLLs may have clinical value in increasing the tolerance or compliance of patients for liver MR imaging which currently require multiple relatively long breath-holding sessions of up to 18~22 seconds. The results of sparse reconstruction including that for CS techniques depends highly on the choice of the regularization parameters, the sampling pattern of MR data, and the degree of undersampling.16 An excessively high regularization parameter value can lead to the excessive removal of low-value coefficients in the sparse domain, resulting in image blurring or loss of small image features, while an excessively low value can lead to incomplete removal of incoherent artifacts.4 In our study, we used a total AF of 4.5 for CS-SENSE mDixon-GRE images which is a relatively high acceleration of acquisition speed. In addition, we also used irregular sampling pattern (pseudorandom), which resulted in higher central sampling and lower peripheral data sampling. Furthermore, regularization corresponding to a denoising level of 20% was selected to improve denoising without significant loss in detail. We intentionally kept AF along Ky or Kz direction from SENSE not to exceed 2 to avoid large noise amplification for our standard mDixon-GRE sequence.CONCLUSION
The CS-SENSE mDixon-GRE sequence provided comparable overall image quality and non-inferior solid FFL detectability compared to the standard mDixon-GRE sequence, with reduced acquisition time.Acknowledgements
No acknowledgement found.References
1. McGibney G, Smith MR, Nichols ST, Crawley A. QUANTITATIVE-EVALUATION OF SEVERAL PARTIAL FOURIER RECONSTRUCTION ALGORITHMS USED IN MRI. Magnetic Resonance in Medicine. 1993;30(1):51-59.
2. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: Sensitivity encoding for fast MRI. Magnetic Resonance in Medicine. 1999;42(5):952-962.
3. Griswold MA, Jakob PM, Heidemann RM, et al. Generalized Autocalibrating Partially Parallel Acquisitions (GRAPPA). Magnetic Resonance in Medicine. 2002;47(6):1202-1210.
4. Feng L, Benkert T, Block KT, Sodickson DK, Otazo R, Chandarana H. Compressed sensing for body MRI. Journal of magnetic resonance imaging : JMRI. 2016.
5. Liang D, Liu B, Wang J, Ying L. Accelerating SENSE using compressed sensing. Magnetic Resonance in Medicine. 2009;62(6):1574-1584.
6. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic Resonance in Medicine. 2007;58(6):1182-1195.
7. Candès EJ, Romberg J, Tao T. Robust uncertainty principles: Exact signal reconstruction from highly incomplete frequency information. IEEE Transactions on information theory. 2006;52(2):489-509.
8. Donoho DL. Compressed sensing. IEEE Transactions on information theory. 2006;52(4):1289-1306.
9. Lustig M, Donoho DL, Santos JM, Pauly JM. Compressed sensing MRI. IEEE signal processing magazine. 2008;25(2):72-82.
10. Chandarana H, Feng L, Block TK, et al. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Investigative radiology. 2013;48(1).
11. Jaspan ON, Fleysher R, Lipton ML. Compressed sensing MRI: a review of the clinical literature. British Journal of Radiology. 2015;88(1056).
12. Liu F, Duan Y, Peterson BS, Kangarlu A. Compressed sensing MRI combined with SENSE in partial k-space. Phys Med Biol. 2012;57(21):N391-403.
13. Runge VM. Current Technological Advances in Magnetic Resonance With Critical Impact for Clinical Diagnosis and Therapy. Investigative Radiology. 2013;48(12):869-877.
14. Fletcher JG, Yu L, Li Z, et al. Observer performance in the detection and classification of malignant hepatic nodules and masses with CT image-space denoising and iterative reconstruction. Radiology. 2015;276(2):465-478.
15. Lee SJ, Park SH, Kim AY, et al. A prospective comparison of standard-dose CT enterography and 50% reduced-dose CT enterography with and without noise reduction for evaluating Crohn disease. American Journal of Roentgenology. 2011;197(1):50-57.
16. Yang AC, Kretzler M, Sudarski S, Gulani V, Seiberlich N. Sparse Reconstruction Techniques in Magnetic Resonance Imaging: Methods, Applications, and Challenges to Clinical Adoption. Investigative Radiology. 2016;51(6):349-364.
Figures
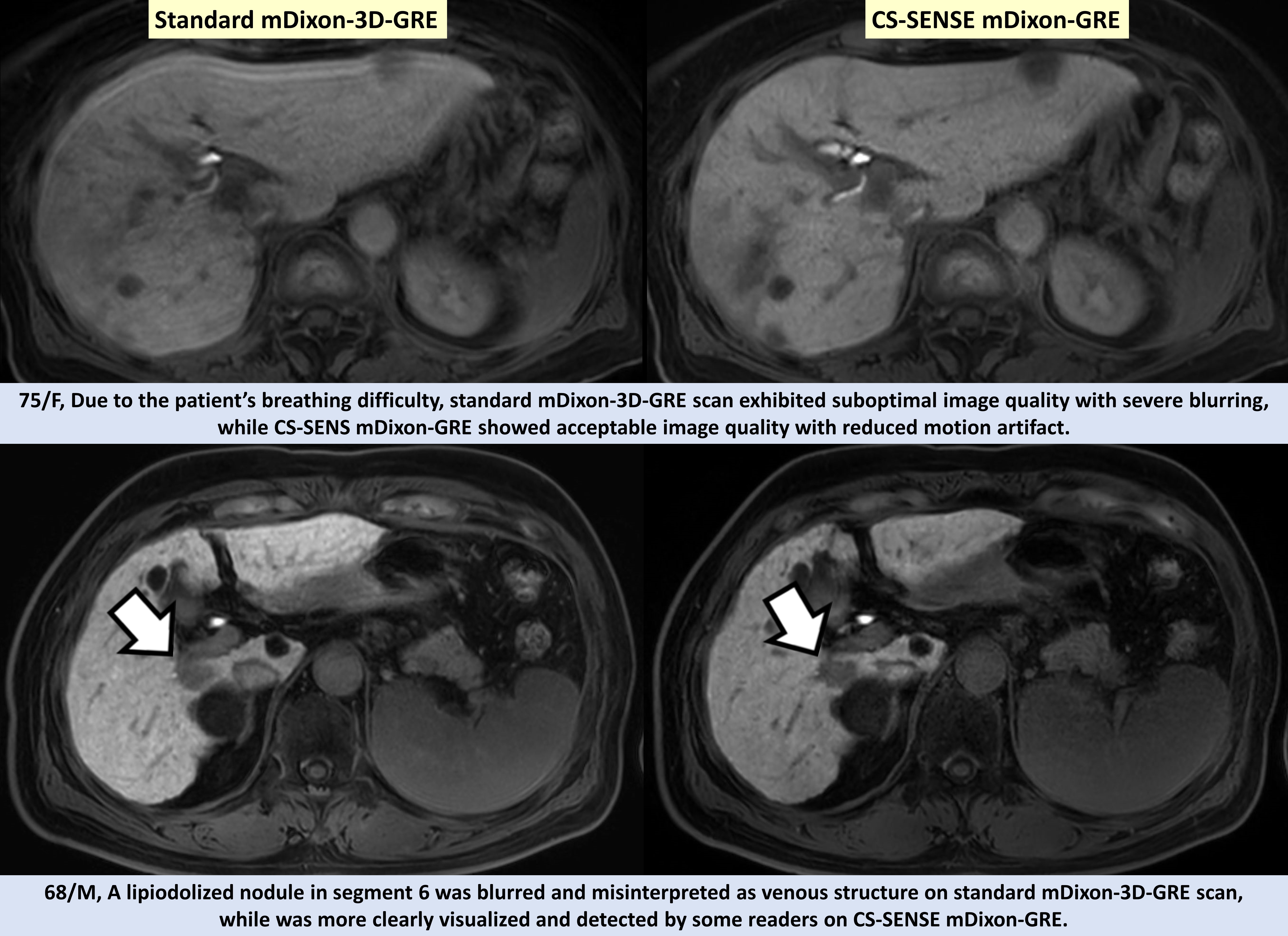
Representative Cases