4565
Rapid single slice multidimensional fetal flow imaging with MRI1Medical Biophysics, University of Toronto, Toronto, ON, Canada, 2Translational Medicine, Hospital for Sick Children, Toronto, ON, Canada, 3Biomedical Engineering, Ryerson University, Toronto, ON, Canada, 4The Keenan Research Centre for Biomedical Science, St. Michael’s Hospital, Toronto, ON, Canada, 5Division of Cardiology, Hospital for Sick Children, Toronto, ON, Canada, 6Paediatrics, University of Toronto, Toronto, ON, Canada
Synopsis
In this study, we demonstrate multidimensional fetal blood flow quantification, using a novel radial phase contrast sampling strategy combined with compressed sensing reconstruction. This acquisition and analysis pipeline provides high temporal resolution real-time reconstructions that enable image-based gating for subsequent CINE reconstruction. Experimental validation of gating and flow quantitation are presented from an adult volunteer. Preliminary results in two human fetuses show the feasibility of this novel strategy for multidimensional fetal flow in imaging in a single slice.
Introduction
Velocity sensitive phase contrast (PC) MR is the gold standard for measuring blood flow in postnatal subjects and, using image-based cardiac gating, has enabled quantification of fetal blood flow in both normal pregnancies and fetal congenital heart disease1. Unfortunately, studies of fetal blood flow have been limited by motion, placing constraints on the achievable spatial resolution, temporal resolution, and number of dimensions of flow sensitivity2. In this work, we demonstrate a novel method for high resolution multidimensional imaging of fetal flow. Recent studies have overcome these limitations for anatomical imaging of the fetal heart by implementing a golden-angle radial acquisition, which enables intermediate real-time (RT) reconstructions for performing motion correction and image-based gating2,3. The motion-corrected and retrospectively gated data are then combined to produce a high-quality CINE reconstruction using compressed sensing (CS) to remove residual artifact4,5.
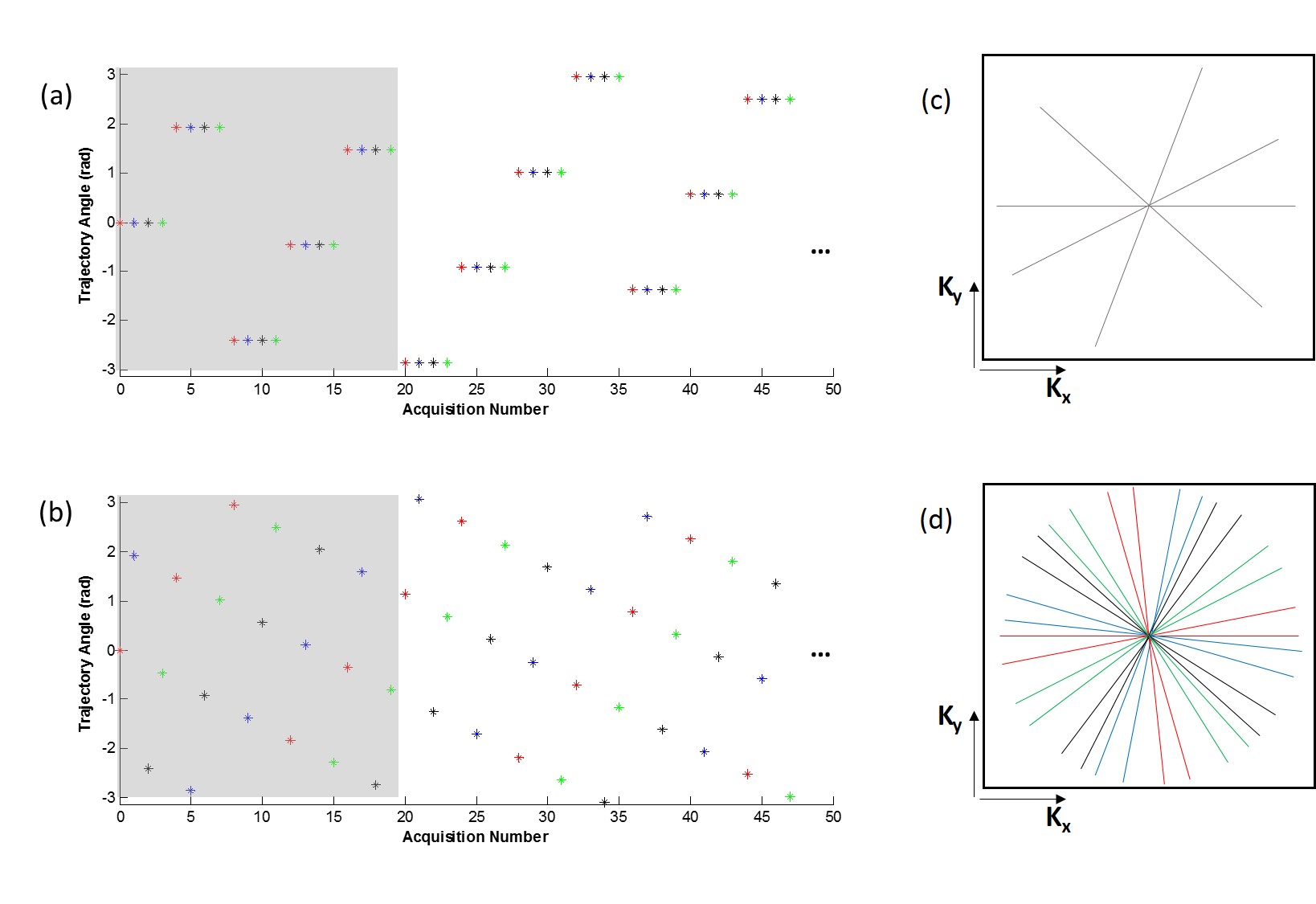
Conventional PCMR requires repeating each radial spoke for each flow encode as demonstrated by Fig. 1a. This results in lower temporal resolution of the RT reconstructions relative to anatomical imaging, effectively reducing the accuracy of image-based gating strategies. In this work, we propose an alternate strategy that increments both the golden-angle radial trajectory and the velocity encoding direction, synchronously (Fig. 1b), thereby preserving the temporal resolution of RT reconstructions. We combine this sampling strategy with translational motion correction, image-based gating (metric optimized gating, MOG)2, and CS to reconstruct high-quality flow images from accelerated acquisitions. Experimental validation of this strategy is performed in an adult volunteer. Using this pipeline, we present the first multidimensional PCMR velocity maps of the human fetal heart.
Methods
Validation of the proposed acquisition and reconstruction strategy was performed in a healthy adult volunteer using a 1.5T MRI system (AvantoFIT, Siemens). Relevant PCMR parameters were: total spokes 4000 (across all flow encodes), field-of-view 340x340mm2, resolution 1.3x1.3x5mm3, TR 7ms, scan time 29s, VENC 150cm/s. Imaging was performed at the bifurcation of the pulmonary artery, and repeated 4 times to test repeatability. Scans were performed without cardiac gating, although the pulse gating signal was logged for subsequent comparison to MOG. MOG was performed on velocity-sensitive RT reconstructions from a window of 16 spokes per frame with 50% view sharing (effective temporal resolution: 40ms)2,6. For computational efficiency, CS of the real-time reconstructions was performed using iterative thresholding with only temporal total variation sparsity. Final CS CINE reconstructions of the retrospectively gated data were performed with a conjugate gradient algorithm and spatial total variation, complex difference and temporal Fourier sparsities. Quantitative evaluation of the proposed sampling and reconstruction scheme compared cardiac gating timing and flow parameters obtained using MOG versus those obtained using pulse gating.
Feasibility of the proposed methods in the fetal population was assessed in two healthy pregnancies (32 weeks gestation) imaged using a 3T MRI system (PrismaFIT, Siemens). The imaging parameters were: free breathing, total number of spokes 4800 (across all flow encodes), field-of-view 256x256mm2, resolution 1x1x4mm3, TR 6ms, scan time 28s, VENC 80cm/s. Acquisitions were motion compensated and then gated with MOG. Final CINE reconstructions were performed as in the adult.
Results
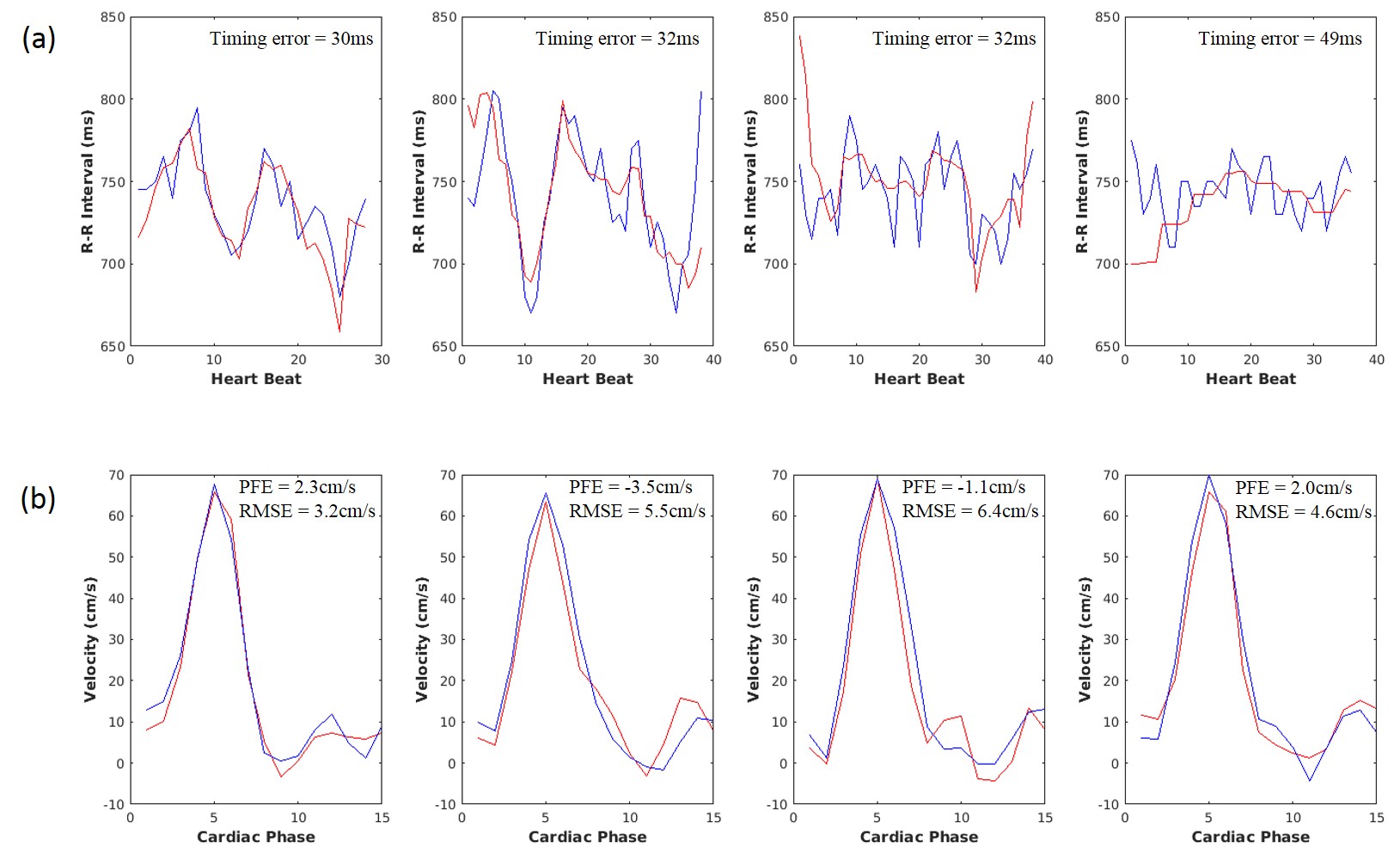
A CINE reconstruction of adult data obtained using the proposed pipeline is shown in Fig. 2. Qualitatively, pulsatile flow is well visualized along each flow dimension. These qualitative observations are consistent with the quantitative analysis in Fig. 3, which shows that the R-R intervals detected by MOG agreed well with pulse gating, having a mean timing error of 35ms (Fig. 3a). The MOG and pulse gated flows had an RMSE of 5.1cm/s across all four acquisitions, and differed in peak flow by ‑0.1±2.7cm/s (Fig. 3b).
Reconstructed fetal flow CINEs in four-chamber and three-vessel views are presented in Fig. 4, showing the complex hemodynamics within the fetal heart. Figure 5 further illustrates this using velocity vectors of the in-plane flow only, depicting blood passage through the heart with in-plane speeds reaching 80cm/s during peak filling and contraction.
Discussions
The proposed sampling strategy incremented both the radial trajectory and the velocity encoding direction, synchronously. This allowed RT reconstructions at high temporal resolution, which was required for image-based gating. To achieve similar RT imaging quality with conventional PCMR sampling leads to unacceptable temporal resolution for fetal applications. This proposed approach may also be useful for multidimensional flow studies in uncooperative subjects, such as neonates or the elderly.Conclusions
We have proposed and demonstrated a novel sampling and reconstruction pipeline targeting fetal blood flow applications. This pipeline was validated in an adult study, and its feasibility tested in two fetuses resulting in the first multidimensional velocity maps of the fetal heart obtained using MRI.Acknowledgements
No acknowledgement found.References
1. Seed M, van Amerom J, Yoo S, et al. Feasibility of quantification of the distribution of blood flow in the normal human fetal circulation using CMR: a cross-sectional study. JCMR. 2012; 14:79.
2. Roy C, Seed M, Macgowan C. Accelerated MRI of the fetal heart using compressed sensing and metric optimised gating. MRM. 2017; 77(6):2125-2135.
3. Chaptinel J, Mivelaz Y, Yerly J et al. A golden-angle acquisition coupled with k-t sparse SENSE reconstruction for fetal self retro-gated CINE cardiac MRI: an in vivo feasibility study. In: Proc 24th Annual Meeting ISMRM, Singapore;2016.
4. Lustig M, Donoho D, Pauly JM. Sparse MRI: The application of compressed sensing for rapid MR imaging. MRM. 2007; 58(6):1182-95.
5. Otazo R, Candès E, Sodickson D. Low-rank plus sparse matrix decomposition for accelerated dynamic MRI with separation of background and dynamic components. MRM. 2015; 73(3):1125-1136.
6. Jansz M, van Amerom J, Wong D et al. Metric optimized gating for fetal cardiac MRI. MRM. 2012; 64(5):1304-14.
Figures