4489
MultiVane Diffusion-Weighted Imaging for Multiparametric Prostate Magnetic Resonance Imaging in Men with Hip Implants: A Preliminary Report1Radiology, UT Southwestern Medical Center, Dallas, TX, United States, 2Philips Healthcare, Gainesville, FL, United States, 3Radiology, Advanced Imaging Research Center, UT Southwestern Medical Center, Dallas, TX, United States, 4Radiology, Advanced Imaging Research Center, Urology, UT Southwestern Medical Center, Dallas, TX, United States
Synopsis
Diffusion-weighted echo-planar-imaging (DW-EPI) is the cornerstone of multiparametric MRI in evaluation of prostate cancer in the peripheral zone and can help in the detection of transitional zone tumors. However, DW-EPI suffers from significant image distortion and signal loss in men with hip arthroplasty, a population at risk for development of prostate cancer. We have implemented a DWI sequence with turbo spin-echo readout, MultiVane k-space trajectory, and short-tau inversion recovery fat-suppression that provides images without appreciable distortion and promising preliminary results in evaluation of prostate cancer in men with hip implants.
Introduction
Metal-associated artifacts significantly affect the quality of diffusion-weighted echo-planar imaging (DW-EPI), the cornerstone of multiparametric MRI (mpMRI) for evaluation of prostate cancer in the peripheral zone, where 70-80% of prostate cancers arise [1-7]. These artifacts are often severe enough to render the DW-EPI images non-diagnostic. Considering the demographical overlap of men with hip replacement and those with prostate cancer [8-10], there is a critical need for a robust DWI sequence to image this population. In this work, we explored turbo spin echo (TSE) based DWI sequences to minimize metal artifacts in men with hip implants.Methods
Phantom Studies
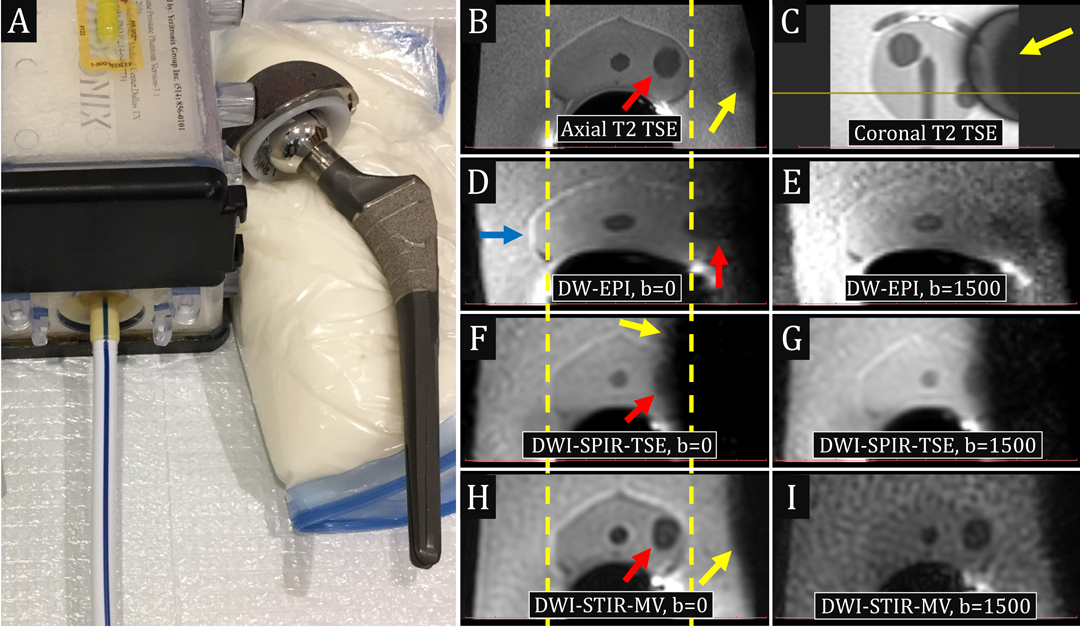
Experiments were performed on a 3T scanner (Ingenia; Philips Healthcare, Best, The Netherlands) with a 16-channel anterior torso coil, 12-channel posterior coil embedded in the table, and an endorectal coil (Medrad, Warrendale, PA). A Titanium-alloy hip implant (Zimmer-Biomet, Warsaw, IN) was placed adjacent to a prostate phantom (version 3.1, Yezitronix Group Inc., Quebec, Canada), simulating the artifact caused by the hip implant in vivo. TSE-based DWI sequences were tested and optimized with both Cartesian and MultiVane (MV) k-space trajectories, using spectral presaturation inversion recovery (SPIR) and non-selective short-tau inversion recovery (STIR), respectively, for fat-suppression. Axial and coronal T2-weighted TSE and axial single-shot DW-EPI images were obtained per standard clinical protocol for comparison.
Patient Studies
TSE-based DWI sequences (both Cartesian and MV) were added to the standard clinical protocol (performed on a 3T scanner with similar configurations as above) in 5 men with clinical suspicion of prostate cancer and prior hip arthroplasty and non-diagnostic standard DW-EPI images. Limited TSE acquisitions were also performed in 8 patients without prosthesis to compare image quality/distortion and tumor visualization to that of the standard DW-EPI acquisitions. Under Institutional Review Board approval MRIs in these patients were retrospectively reviewed.
Results
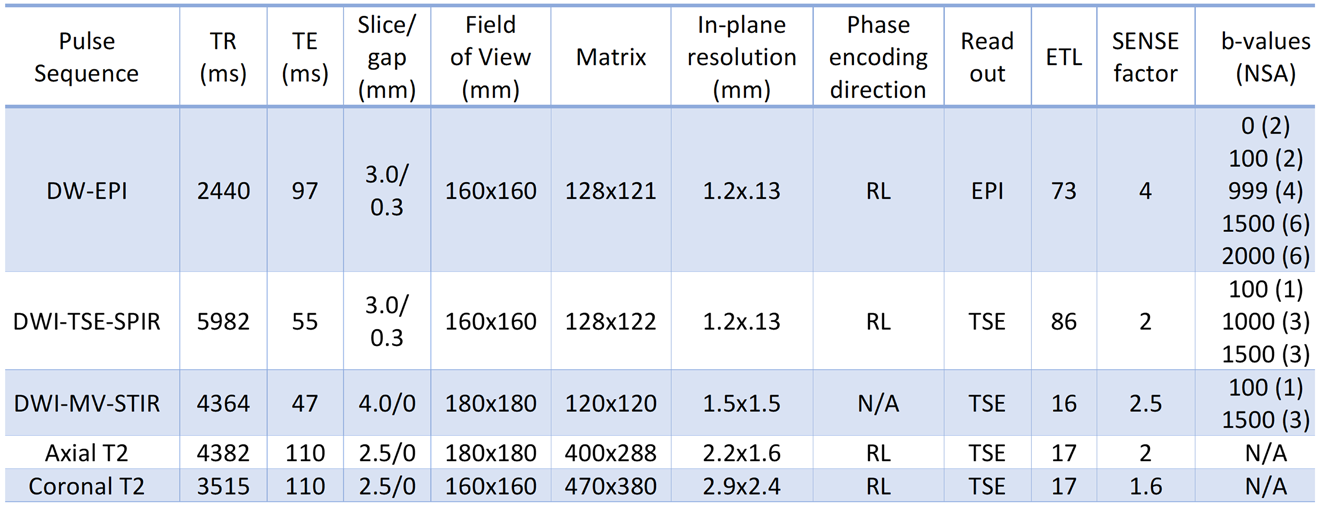
Table 1 summarizes the optimized imaging parameters. Figure 1 illustrates significant image distortion and signal loss in the clinical DW-EPI acquisition (Figure 1, D & E). While a single-shot DWI-TSE with Cartesian k-space trajectory eliminated image distortion, it suffered severe signal loss in proximity to the metal (Figure 1, F & G), due to increased B0-inhomogeneity and use of frequency-selective SPIR fat-suppression. A DWI-TSE with MultiVane k-space trajectory and non-selective STIR fat-suppression (DWI-STIR-MV) revealed the entire gland without appreciable image distortion (Figure 1, H & I).
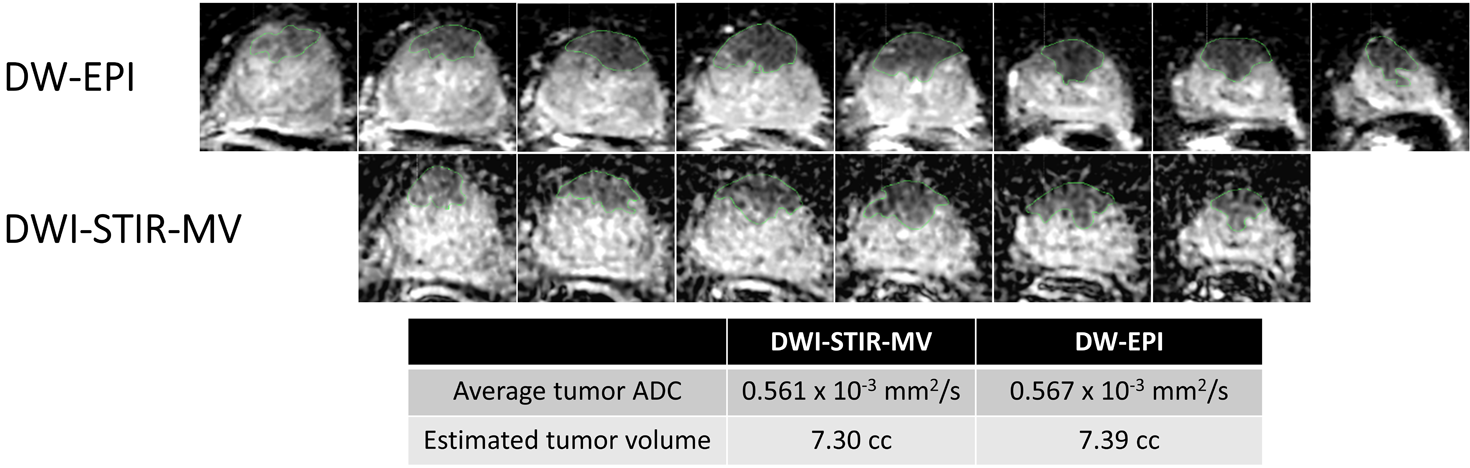
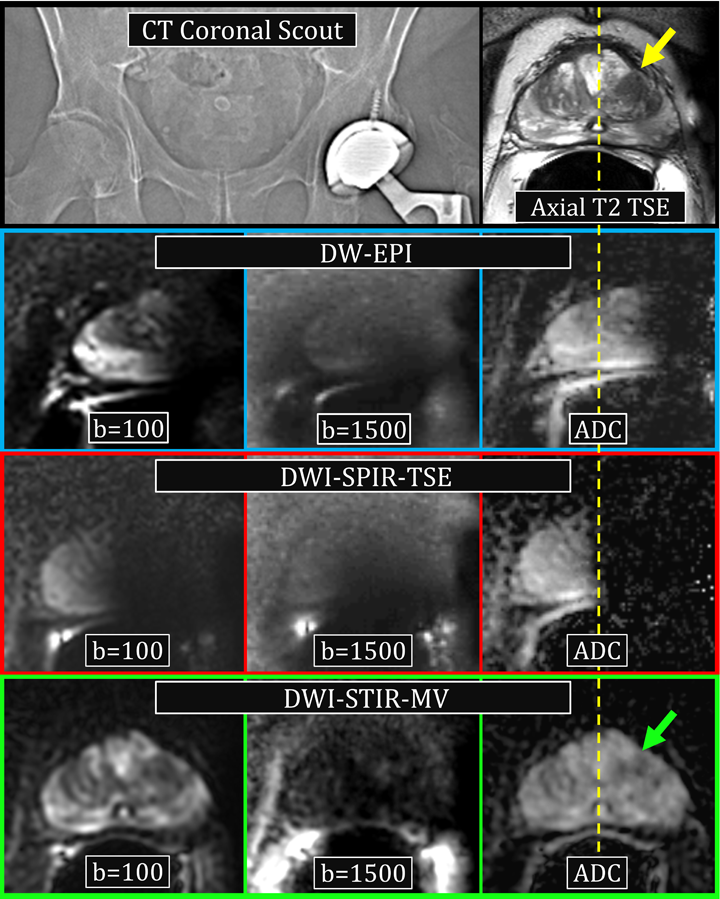
In patients without hip implants, DW-EPI demonstrates favorable image quality and higher SNR compared to DWI-STIR-MV (Figure 2), with good agreement in estimated tumor volume and average apparent diffusion coefficient (ADC) between the two techniques. However, DW-EPI suffered significant image distortion and signal loss in a subject with a hip implant (Figure 3). The DWI-STIR-MV sequence revealed the prostate without appreciable image distortion; a focus suspicious for cancer in this patient was only visible on the T2-weighted and DWI-STIR-MV images. Targeted MR/transrectal ultrasound fusion biopsy confirmed Gleason 4+4 adenocarcinoma.
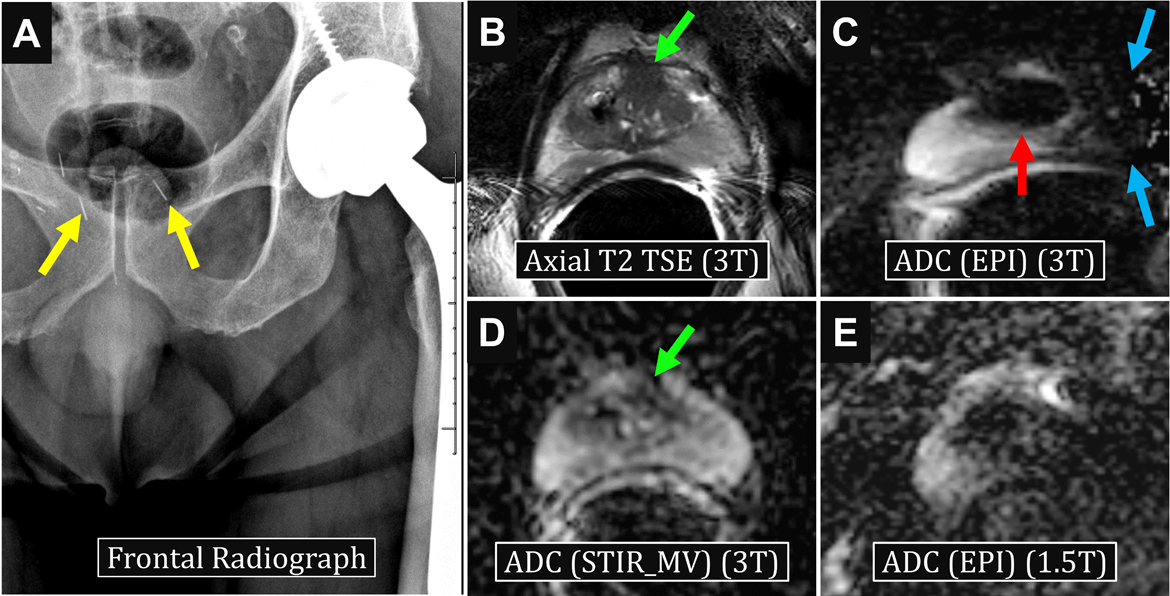
Figure 4 illustrates representative images from prostate MRI in a patient with suspected prostate cancer, prior total left hip arthroplasty, and UroLift® system placement (metal devices implanted within the prostate for treatment of benign prostatic hyperplasia). While the DW-EPI images were non-diagnostic due to artifacts from the hip implant and the prostate device, the DWI-STIR-MV sequence provided diagnostic images, revealing a focus suspicious for cancer. Of note, same-day images from the same patient at 1.5T did not result in improved image quality (Figure 4E).
Discussion
Attempts to move patients with hip prosthesis to a 1.5T scanner after the 3T examinations render non-diagnostic DW-EPI prostate images are generally unsuccessful. Our preliminary results suggest a TSE-based MultiVane DWI sequence with STIR fat-suppression can provide diagnostic-quality images in men with hip implants, without appreciable image distortion and potentially superior gland and tumor visualization compared to DW-EPI. Compared to DW-EPI, the primary limitations of the DWI-STIR-MV sequence are lower SNR and longer acquisition times (approximately 10-13 minutes for 2 b-values, depending on the size of the prostate gland). Although this may seem impractical, it is important to emphasize that in patients with hip prosthesis, this may be the only available diagnostic DWI sequence to diagnose otherwise undetectable cancer. The main limitations of this study are the small number of subjects and its retrospective nature; however, given these encouraging results, we have implemented the DWI-STIR-MV sequence as part of our clinical prostate MRI for men with implants, which will provide more insight into its accuracy for lesion detection.Conclusion
A TSE-based MultiVane DWI sequence with STIR fat-suppression may improve the visualization of prostate cancer in men with metal implants undergoing multiparametric MRI. Further studies are necessary to test its diagnostic accuracy.Acknowledgements
The hip implant used for phantom studies was a sample device lent by Zimmer Biomet.References
1. Hambrock, T., et al., Relationship between apparent diffusion coefficients at 3.0-T MR imaging and Gleason grade in peripheral zone prostate cancer. Radiology, 2011. 259(2): p. 453-61.
2. Vargas, H.A., et al., Diffusion-weighted endorectal MR imaging at 3 T for prostate cancer: tumor detection and assessment of aggressiveness. Radiology, 2011. 259(3): p. 775-84.
3. Turkbey, B., et al., Is apparent diffusion coefficient associated with clinical risk scores for prostate cancers that are visible on 3-T MR images? Radiology, 2011. 258(2): p. 488-95.
4. Bittencourt, L.K., et al., Prostate MRI: diffusion-weighted imaging at 1.5T correlates better with prostatectomy Gleason Grades than TRUS-guided biopsies in peripheral zone tumours. Eur Radiol, 2012. 22(2): p. 468-75.
5. Oto, A., et al., Diffusion-weighted and dynamic contrast-enhanced MRI of prostate cancer: correlation of quantitative MR parameters with Gleason score and tumor angiogenesis. AJR Am J Roentgenol, 2011. 197(6): p. 1382-90.
6. Wu, L.M., et al., The clinical value of diffusion-weighted imaging in combination with T2-weighted imaging in diagnosing prostate carcinoma: a systematic review and meta-analysis. AJR Am J Roentgenol, 2012. 199(1): p. 103-10.
7. Haffner, J., et al., Peripheral zone prostate cancers: location and intraprostatic patterns of spread at histopathology. Prostate, 2009. 69(3): p. 276-82.
8. Maradit Kremers, H., et al., Prevalence of Total Hip and Knee Replacement in the United States. J Bone Joint Surg Am, 2015. 97(17): p. 1386-97.
9. Jemal, A., et al., Cancer statistics, 2010. CA Cancer J Clin, 2010. 60(5): p. 277-300.
10. American Cancer Society. 2017 01/05/2017 08/162017]; Available from: https://www.cancer.org/cancer/prostate-cancer/about/key-statistics.html#references.
Figures