4446
Diffusional Kurtosis Imaging for Differentiation of Additional Suspicious Lesions on Preoperative Breast MRI of Patients with Known Breast Cancer1Radiology, Yonsei University College of Medicine, Seoul, Republic of Korea, 2Center for Advanced Imaging Innovation and Research (CAI2R), New York University School of Medicine, New York, NY, United States
Synopsis
We investigated the potential of diffusional kurtosis imaging (DKI) and conventional diffusion weighted imaging (DWI) for differentiation of additional suspicious lesions on preoperative breast MRI patients with known breast cancer. This study included 53 pathologically confirmed lesions larger than 10mm in 45 women with known breast cancer. DKI and DWI parameters were compared between lesions. Multiple DKI parameters showed a significant difference between benign vs. invasive breast lesions and a few differed between DCIS vs. invasive breast lesions, with high specificity. However, DKI and DWI could not distinguish DCIS from benign lesions and may have lower potential in this subgroup
Introduction
Diffusion weighted imaging (DWI) has been proposed to improve the specificity of breast MRI.1 Although the conventional DWI model assumes a Gaussian diffusion of water protons, water diffusion in complex biological tissues shows a non-Gaussian phenomena, likely associated with tissue microstructure.2-3 Diffusional kurtosis imaging (DKI) is a non-Gaussian diffusion weighted model and includes calculation of diffusivity (D, diffusion coefficient with correction of non-Gaussian bias) and kurtosis (K, deviation of tissue diffusion from a Gaussian pattern).4 Several recent studies reported that DKI improved characterization of breast lesions.3-4. In clinical practice, patients often undergo breast MRI for evaluation of known breast cancer and would benefit from accurate assessment of any additional suspicious lesions seen on breast MRI. Hence, the purpose of this study was to investigate the potential of DKI and DWI for evaluation of additional suspicious lesions on preoperative breast MRI patients with known breast cancer.Methods
Fifty-three pathologically confirmed additional suspicious breast lesions larger than 10 mm in 45 women with newly diagnosed breast cancer were included. Patients were scanned with a 3T MRI scanner (Ingenia, Philips Medical Systems). Diffusion MRI study was performed before dynamic contrast enhanced MRI, using a spin-echo single-shot EPI pulse sequence with parallel imaging, SPAIR fat suppression, slice thickness=3mm, voxel size= 1.5x1.5x3.0 mm3, TR/TE= 14275/121 ms/ms, and b-values of 0, 50, 600, 1000, and 3000 sec/mm2. For a conventional DWI measure, apparent diffusion coefficient (ADC) was estimated from with b=50, 600, and 1000 sec/mm2. For DKI, D and K were calculated from b values between 50 and 3000, using an in-house software. Data were analyzed in consensus by two radiologists and a region of interest (ROI) was manually drawn on a representative slice of DWI images, with reference to contrast-enhanced T1-weighted images. Histogram analysis was applied to D, K, and ADC and the histogram measures included in this study were mean, standard deviation (SD), minimum, maximum, 10th, 25th, 50th, 75th, 90th percentiles and kurtosis, skewness and entropy. We compared the histogram measures of D, K and ADC between benign vs. malignant lesions, and also performed multigroup comparisons between benign vs. ductal carcinoma in situ (DCIS) vs. invasive breast lesions with the Bonferroni correction. For the parameters that showed a significant difference, we performed a receiver operating characteristic (ROC) curve analysis. Correlation between the mean values of D and K was analyzed by Spearman coefficient (rs) according to lesion type.Results
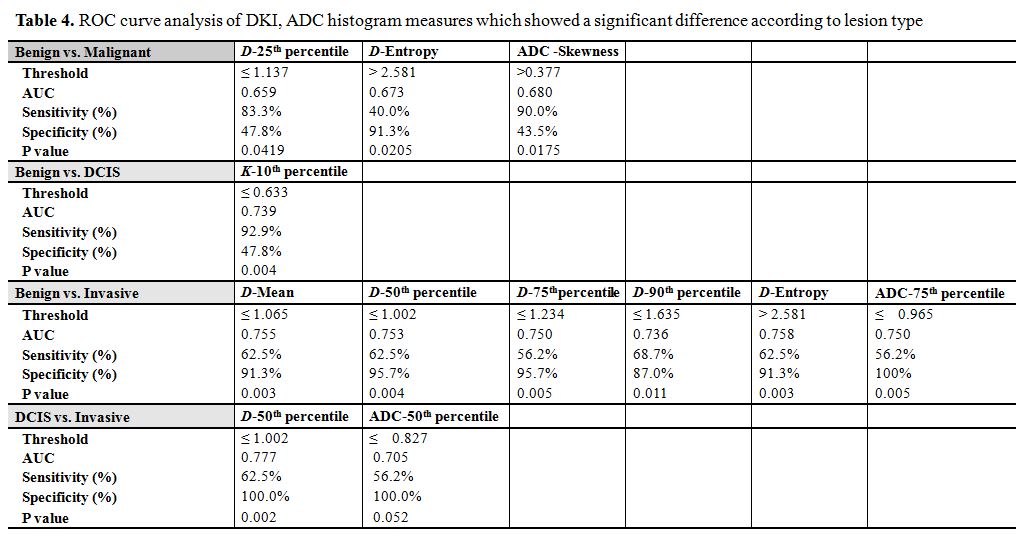
The median size of the included lesions on MRI was 12 mm (range, 11−99 mm). Twenty-three (43.4%) lesions were benign and 30 (46.6%) were malignant (n=14 for DCIS and 16 for invasive carcinoma). For the comparison between benign and malignant lesions, D differed significantly in terms of the 25th percentile (benign vs. malignant: 1.07 vs. 0.94, P=.048) and entropy (1.37 vs. 1.75, P=.032). None of the histogram measures of K showed a significant difference. The skewness of ADC showed a significant difference (-0.13 vs. 0.21, P=.026).
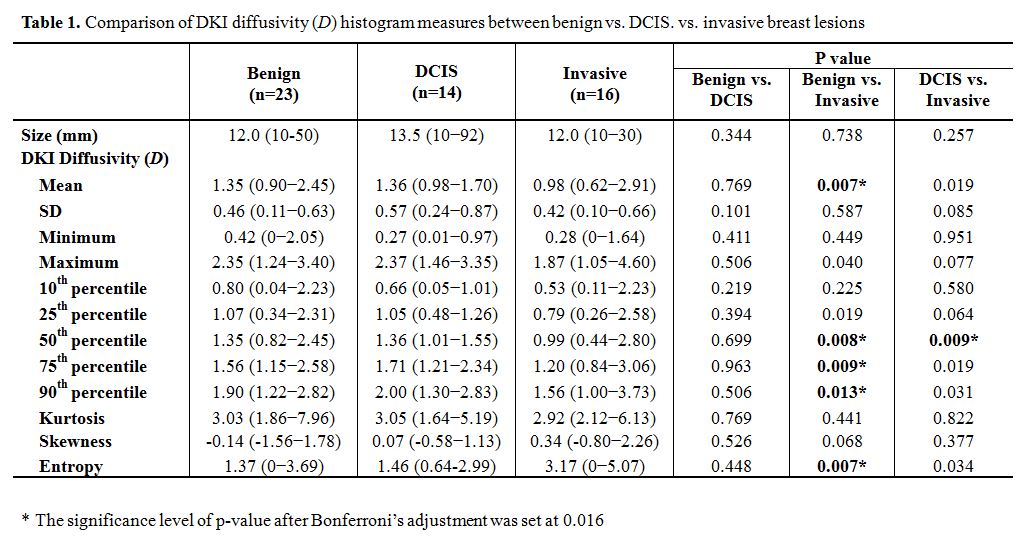
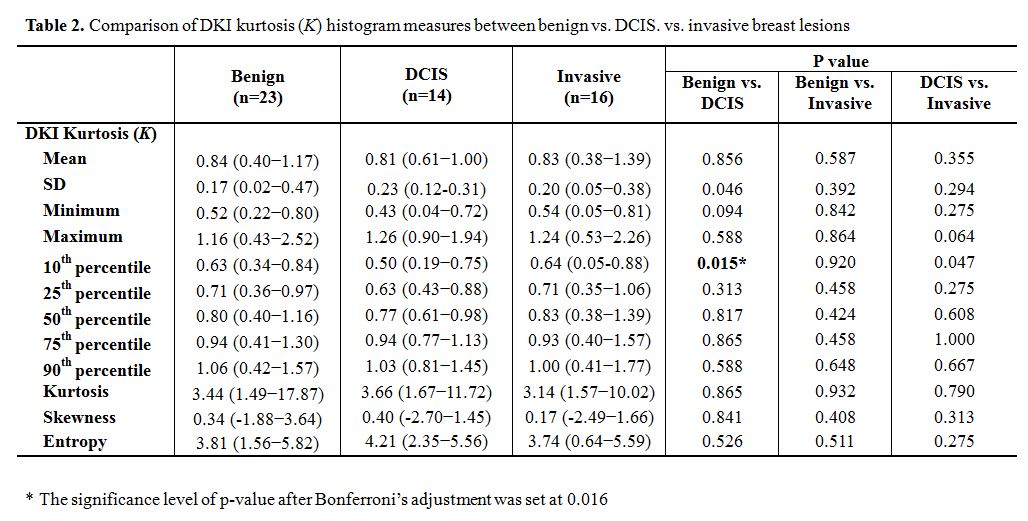
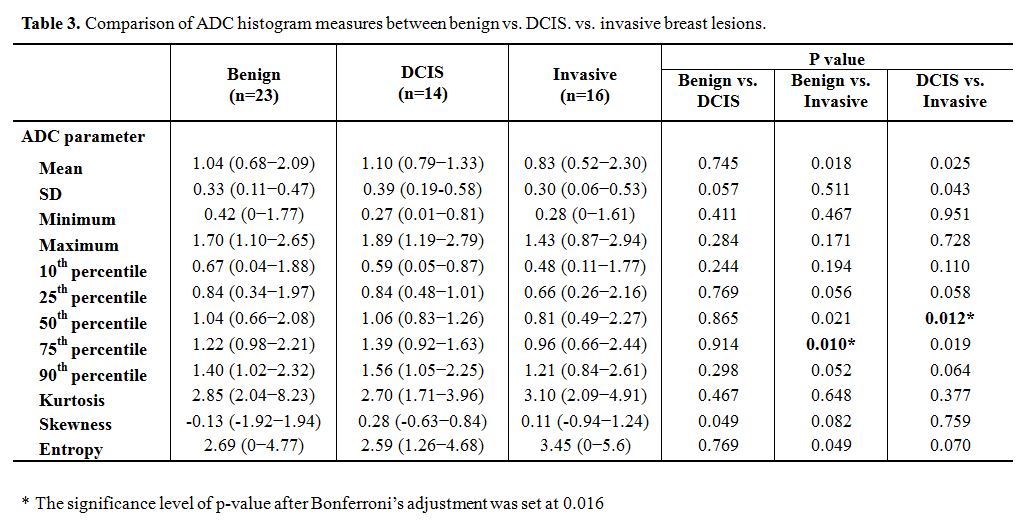
For the multigroup comparison (Table 1), a significant difference between benign vs. invasive breast lesions was found in multiple histogram parameters of D (mean, 50th percentile, 75th percentile, 90th percentile, and entropy). D-50th percentile differed significantly between DCIS and invasive breast lesions. However, D did not show any significant difference between benign and DCIS lesions. K-10th percentile differed between benign vs. DCIS lesions (0.63 vs. 0.50, P =.015) (Table 2). ADC-75th percentile and ADC-50th percentile significantly differed between benign vs. invasive and DCIS vs. invasive, respectively (Table 3). The ROC curve analysis (Table 4) shows high specificity of multiple D parameters and ADC-75th percentile for distinguishing invasive from benign breast lesions, and high specificity of D-50th percentile for distinguishing DCIS vs. invasive breast lesions.
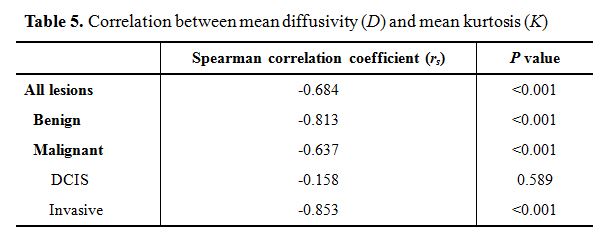
D-mean and K-mean showed strong correlation in all lesions (rs=−0.684), and very strong correlation in benign and invasive breast lesions (rs=−0.813 and rs=−0.853). There was no significant correlation in DCIS (Table 5).
Discussion/Conclusion
The results in this study suggest that DKI may help evaluate additional suspicious lesions detected on breast MRI in patients with known breast cancer. When differentiating benign vs. invasive or DCIS vs. invasive breast cancer, D histogram measures showed high specificity. However, K histogram measures did not differ between benign and malignant breast lesions. This may be partly attributed to the small lesion size compared to prior studies. In addition, mean diffusivity and kurtosis showed no correlation in DCIS lesions. Both ADC and DKI parameters could not differentiate benign vs. DCIS breast lesions, implying that DKI may have lower potential in this subgroup. However, further studies are required.Acknowledgements
No acknowledgement found.References
1. Bogner W, Gruber S, Pinker K, et al. Diffusion-weighted MR for differentiation of breast lesions at 3.0 T: how does selection of diffusion protocols affect diagnosis? Radiology 2009;253:341-351.
2. Wu D, Li G, Zhang J, Chang S, Hu J, Dai Y. Characterization of breast tumors using diffusion kurtosis imaging (DKI). PLoS One 2014;9:e113240.
3. Nogueira L, Brandao S, Matos E, et al. Application of the diffusion kurtosis model for the study of breast lesions. Eur Radiol 2014;24:1197-1203.
4. Sun K, Chen X, Chai W, et al. Breast Cancer: Diffusion Kurtosis MR Imaging-Diagnostic Accuracy and Correlation with Clinical-Pathologic Factors. Radiology 2015;277:46-55.
5. Suo S, Zhang K, Cao M, et al. Characterization of breast masses as benign or malignant at 3.0T MRI with whole-lesion histogram analysis of the apparent diffusion coefficient. J Magn Reson Imaging 2016;43:894-902.
Figures