4423
Development of a small-car mountable MRI system for human extremities using a 0.2 T permanent magnet1Institute of Applied Physics, University of Tsukuba, Tsukuba, Japan, 2Institute of Clinical Medicine, Department of Diagnostic and Interventional Radiology, University of Tsukuba, Tsukuba, Japan
Synopsis
We developed a new, compact portable MRI system for imaging extremities using a 0.2 T permanent magnet. The system was sufficiently small in size and mountable on a small, standard-sized vehicle. The use of the open-geometry magnet enabled the easy patient positioning within the limited space in the vehicle. We showed that our portable MRI provides clinically relevant images. The portable system might be deployable during sport events or in resource-poor environments access to MRI systems, and allow mass screening, early diagnosis, and case finding.
INTRODUCTION
Conventional MRI scanners are massive and confined within a hospital. In contrast, portable MRI scanners can provide new opportunities for mobile operation in many environments including disease screening and primary care suite. Here we develop a new, compact portable MRI system for imaging small joints of the extremities using a 0.2 T, 200 kg permanent magnet. The whole system including the magnet, gradient coils, RF probes, and MRI consoles (80 kg in weight) are installed in a standard-sized vehicle. The use of the open-geometry magnet enables the easy patient positioning within the limited space in the vehicle. We show that our portable MRI provides clinically relevant images. The portable system might be deployable during sport events or in resource-poor environments access to MRI systems, and allow mass screening, early diagnosis [1], and case finding.METHOD
We used a 0.2 T permanent magnet (NEOMAX Engineering, Japan; 200 kg; 16 cm gap; 44 cm x 50 cm x 36 cm; 10 ppm over 10 cm diameter of spherical volume (DSV)), a home-built solenoid RF coil, and home-built gradient coils designed with the singular value decomposition method [2] (homogeneity = 90 % over 10cm DSV; gradient efficiency = 1.74 (x), 1.64 (y), 2.97 (z) mT/m/A). The imaging volume was 10 cm DSV. The magnet was portable using a hand lift. A portable MRI console consisted of a digital transceiver (DTRX6, MRTechnology, Japan), a gradient driver (20 V, 10 A, DST Inc., Japan), and a transmitter (150 W, DST Inc., Japan), which were installed in a 19-inch rack (56 cm x 77 cm x 60 cm, 80 kg). The weight of the system was under maximum authorized payload and all the devices were mountable on the vehicle (Mercedes Benz, GH-639811; 191 cm (width) x 193 cm (height) x 476 cm (length); 110 cm (interior width) x 130 cm (interior height) x 240 cm (interior length)) (Fig. 1).
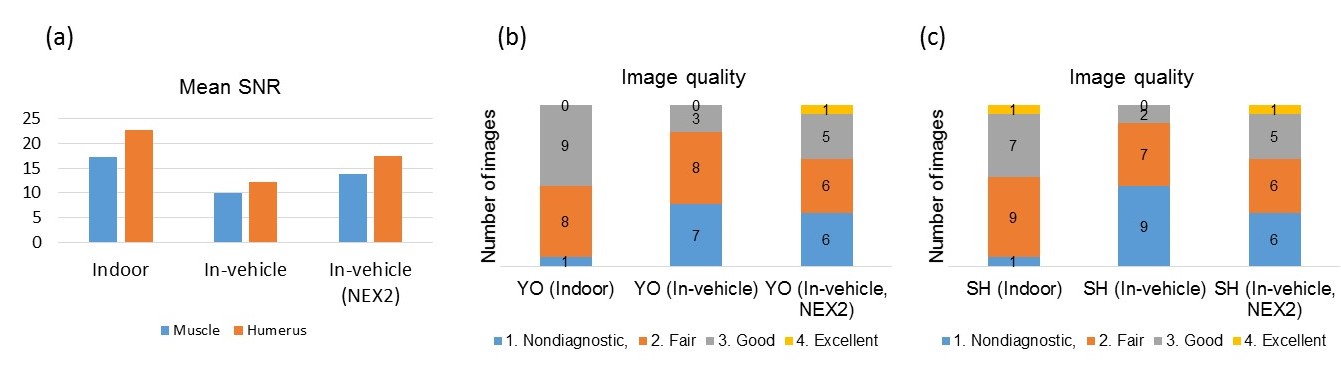
Coronal images of the normal human elbows (nine subjects, 22-44 years) were acquired in an indoor laboratory room and in the vehicle. A gradient echo (TR = 500 ms, TE = 16 ms, FA = 75, slice thickness = 3 mm, matrix size = 256 x 192, FOV = 180 x 180 mm2, measurement time = 1 min 36 sec (NEX = 1)) was used. The image quality was graded by two radiologists (YO and SH) on a 4-point scale: 1 = nondiagnostic, 2 = fair, 3 = good, and 4 = excellent. Rater YO and SH have 18 and 12 years of experience in musculoskeletal radiology, respectively.
RESULTS AND DISCUSSION
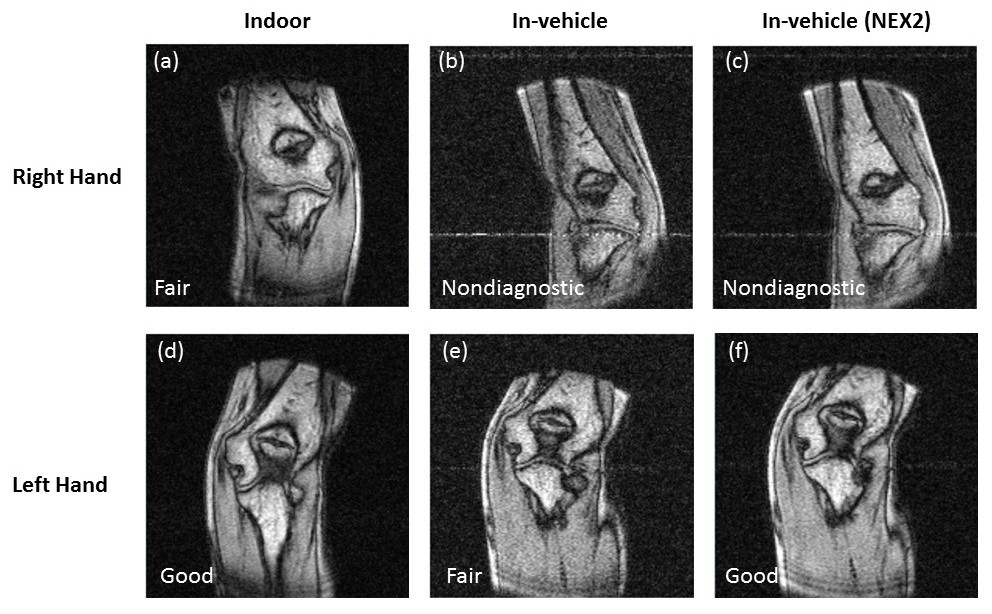
The magnet and the console was quite small and there was a sufficient room in the vehicle for the subject (Fig. 1(b) and (d)), thus providing a comfortable environment for examination. Figures 2 and 3 show examples of MR images. In Fig. 2, anatomical structures, such as medial collateral ligament (MCL), radial, ulna, humerus, and joint spaces were visible in the images acquired in the vehicle, and the image quality scores were better than the fair quality. Figure 3 shows the worst case where the MCL in the right elbow were not clearly visible and the raters assigned the low quality scores. Figure 4 shows the evaluation for the all images. The mean SNR in the vehicle was lower than that in the room, but the difference was not large (Fig. 4(a)). The indoor measurements showed the high quality for most of the cases, demonstrating the high diagnostic performance of this portable system. However, the image quality was degraded in the vehicle environment. This was caused by the incorrect positioning of the subject as shown in Figs. 3(b) and (c), or by the lowering of the SNR due to the increased external noise. The image quality could be improved to the level comparable to the indoor measurements, by the correct positioning using a scout sequence and by the more appropriate grounding and signal averaging to improve the SNR.CONCLUSION
In this study, we developed the portable MRI system for extremities that have the potential for maximizing clinical availability to many environments.Acknowledgements
The authors would like to thank Dr. Haishi for his help to mount the system on his vehicle.References
[1] Y. Okamoto et al., Incidence of elbow injuries in adolescent baseball players: screening by a low field magnetic resonance imaging system specialized for small joints, Jpn J Radiol, 34: 300-6 (2016).
[2] K. Matsuzawa et al., Oval gradient coils for an open magnetic resonance imaging system with a vertical magnetic field, J Magn Reson, 278: 51-59 (2017).
Figures