4360
Multi- and Sigle Parametric Approaches using Chemical Exchange Saturation Transfer (CEST) Imaging, Diffusion-Weighted Imaging and FDG-PET/CT for Pulmonary Nodule Diagnosis1Division of Functional and Diagnostic Imaging Research, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 2Advanced Biomedical Imaging Research Center, Kobe University Graduate School of Medicine, Kobe, Japan, 3Toshiba Medical Systems Corporation, Otawara, Japan, 4Radiology, UC, San Diego, La Jolla, CA, United States, 5Division of Radiology, Department of Radiology, Kobe University Graduate School of Medicine, Kobe, Japan, 6Center for Radiology and Radiation Oncology, Kobe University Hospital, Kobe, Japan
Synopsis
No major reports have been reported the capability for differentiating malignant and benign pulmonary lesions among multi- and single parametric approaches by CEST imaging, DWI and PET/CT. We hypothesized that multi parametric approach by all three techniques had better potential for diagnosis of pulmonary nodule than single parametric approach, when applied with CEST imaging, DWI and FDG-PET/CT. The purpose of this study was to directly and prospectively compare the capability for differentiating of malignant from benign pulmonary nodules between multi- and single-parametric approaches by CEST, DWI, and FDG-PET/CT.
Introduction
Differentiation of malignant from benign nodules is essential for radiological examination in routine clinical practice. Currently, CT and MR imaging including diffusion-weighted imaging (DWI) as well as dynamic contrast-enhanced MR imaging have been applied for morphological evaluation, although FDG-PET and PET/CT are applicable molecular imaging technique in various clinical and academic interest. As compared with FDG-PET or PET/CT, chemical exchange saturation transfer (CEST) imaging has been suggested as the new technique for MR-based molecular imaging, and reported as having the potential for diagnosis of thoracic lesions as well as pulmonary nodules (1, 2). However, no major reports have been reported the capability for differentiating malignant and benign pulmonary lesions among multi- and single parametric approaches by CEST imaging, DWI and PET/CT. We hypothesized that multi parametric approach by all three techniques had better potential for diagnosis of pulmonary nodule than single parametric approach, when applied CEST imaging, DWI and FDG-PET/CT. The purpose of this study was to directly and prospectively compare the capability for differentiating of malignant from benign pulmonary nodules between multi- and single-parametric approaches by CEST, DWI, and FDG-PET/CT.Materials and Methods
Fifty-six consecutive patients (34 men, 22 women; mean age 71 years) with 65 pulmonary nodules prospectively underwent CEST imaging and DWI using a fast advanced spin-echo (FASE) sequence at 3T MR system (Vantage Titan 3T, Toshiba Medical Systems Corporation, Otawara, Tochigi, Japan), FDG-PET/CT, pathological examinations from specimens obtained by transbronchial or CT-guided biopsies or surgical resection, and/or follow-up examinations. According to pathological examination results, all lesions were divided to malignant (n=44) and benign (n=21) groups. To obtain CEST data in each subject, respiratory-synchronized FASE imaging was conducted following a series of magnetization transfer (MT) pulses. Then, magnetization transfer ratio asymmetry (MTRasym) was calculated from z-spectra in each pixel, and MTRasym map was computationally generated. To obtain radiological indexes on CEST imaging, DWI and PET/CT, ROIs were placed over each lesion, and determined MTRasym, apparent diffusion coefficient (ADC) and maximum standard uptake value (SUVmax). Multivariate logistic regression analysis was performed to investigate the discriminating factors of malignant lesions from benign lesions. ROC analysis was performed to compare diagnostic performance among all methods. Finally, sensitivity, specificity and accuracy were compared among all methods by McNemar’s test. A p value less than 0.05 was considered as significant in this study.Results
Representative cases are shown in Figures 1 and 2. There were significant differences of all indexes between malignant (MTRasym: 0.8±3.0%, ADC: 933.9±178.7×10-6mm2/s, SUVmax: 3.7±1.4) and benign (MTRasym: -3.7±4.4%, ADC: 1227.2±127.7×10-6mm2/s, SUVmax: 2.4±0.4) groups (p<0.05). Multivariate regression analysis identified MTRasym (Odds ratio [OR]: 0.62), ADC (OR: 1.01) and SUVmax (OR: 0.15) as a significant differentiator of malignancy. Results of ROC analysis were shown in Figure 3. ROC analysis showed area under the curve (Az) of multiparametric method using all indexes (Az=0.96) was significantly larger than that of SUVmax (Az=0.84, p<0.05). Results of comparison of diagnostic performance among all methods are shown in Figure 4. Sensitivity (SE) and accuracy (AC) of multiparametric method (SE: 90.9 [40/44] %, AC: 89.2 [58/65] %) and MTRasym (SE: 86.4 [38/44] %, AC: 86.2 [56/65] %) were significantly higher than those of SUVmax (SE: 70.5 [31/44] %, p<0.05; AC: 76.9 [50/65] %, p<0.05).Conclusion
Multiparametric approach by CEST imaging, DWI and PET/CT has a potential to improve diagnosis performance of PET/CT alone for diagnosis of pulmonary nodules.Acknowledgements
This work was supported by Toshiba Medical Systems Corporation.References
- Ohno Y, Yui M, Koyama H, et al. Radiology. 2016; 279: 578-589.
- Ohno Y, Kishida Y, Seki S, et al. J Magn Reson Imaging. 2017 Aug 11. doi: 10.1002/jmri.25832. [Epub ahead of print]
Figures

Figure 1. 62-year-old female with invasive adenocarcinoma (L to R: thin-section CT, DWI, ADC map, MTRasym map fused with T2WI, and SUVmax map fused with CT)
Thin-section CT demonstrates a nodule with bubble like appearance in the right upper lobe. SUVmax of this nodule was 2.6. ADC was 1.05×10-6mm2/s. CEST image shows low MTRasym with the value of 1.25. This case was false-negative on PET/CT, and true-positive on DWI and CEST. When combined both indexes, PET/CT with CEST was also diagnosed as malignant nodule, and determined as true-positive case.

Figure 2. 81-year-old male with invasive aspergilosis (L to R: thin-section CT, DWI, ADC map, MTRasym map fused with T2WI, and SUVmax map fused with CT)
Thin-section CT demonstrates a nodule with cavity in the right lower lobe. SUVmax of this nodule was 3.5. ADC was 1.28×10-6mm2/s. CEST image shows low MTRasym with the value of -1.57. This case was false-positive on PET/CT, and true-negative on DWI and CEST. When combined both indexes, PET/CT with CEST was also diagnosed as malignant nodule, and determined as true-negative case.
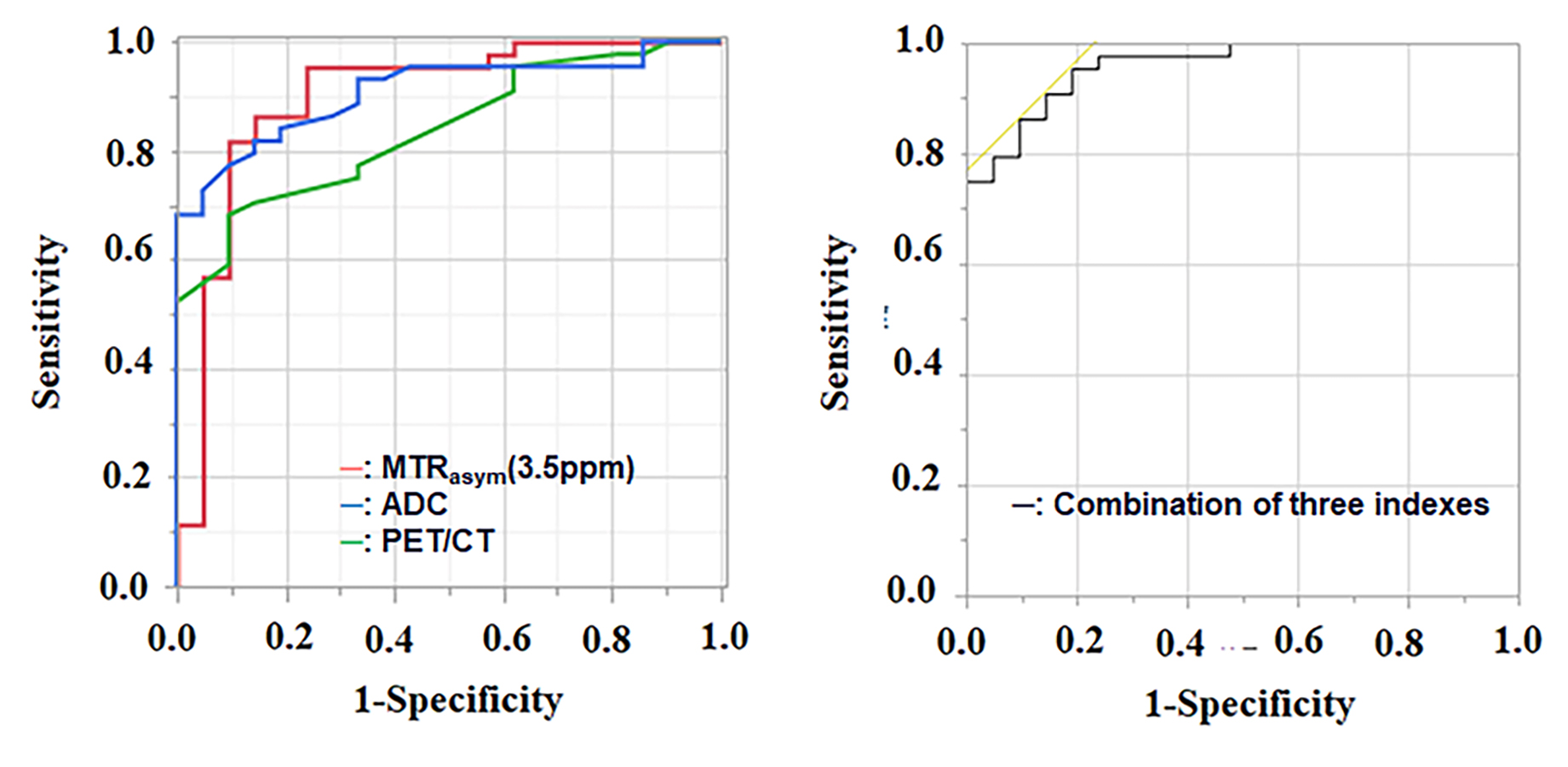
Figure 3. Results of ROC analysis on multi- and single-parametric approaches by MTRasym at 3.5ppm, ADC and SUVmax for distinguishing malignant and benign groups (L to R: Results with single parametric approaches to result with multi parametric approach)
Area under the curve (Az) of combined method (Az=0.96) was significantly higher than that of SUVmax (Az=0.84, p<0.05), although MTRasym (Az=0.90) and ADC (Az=0.91) had no significant difference with combined method.
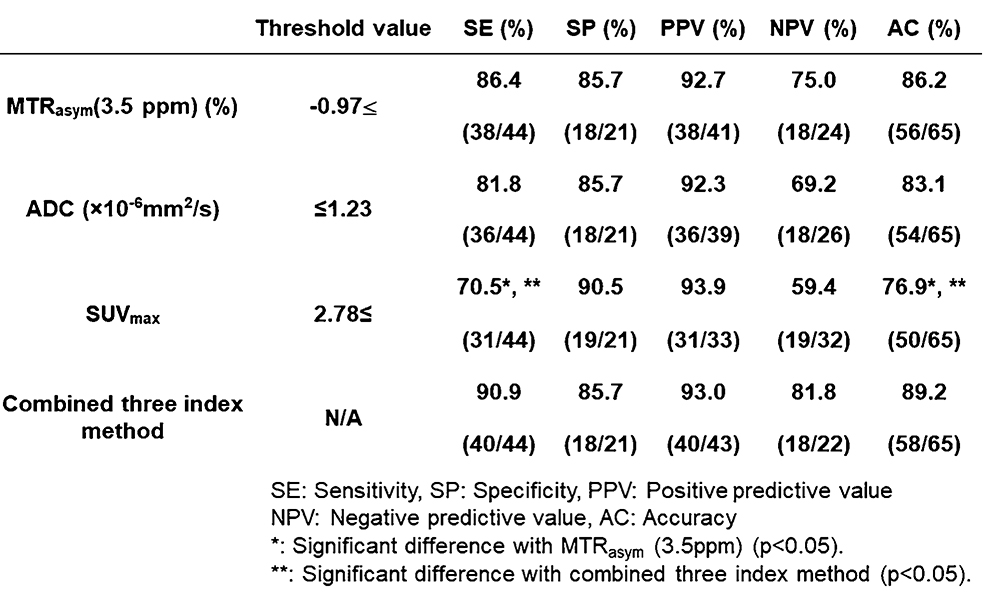
Figure 4. Comparison of diagnostic performance among MTRasym at 3.5ppm, ADC, SUVmax and multiparametric approach for distinguishing malignant and benign groups.
Sensitivity (SE) and accuracy (AC) of multiparametric method and MTRasym were significantly higher than those of SUVmax (p<0.05).