4350
Robust Retrospective Respiratory Gating for Detection of Small Pulmonary Nodules with UTE MRI1Center for Magnetic Resonance Research, Department of Radiology, University of Minnesota, Minneapolis, MN, United States, 2Division of Pulmonary, Allergy, Critical Care and Sleep, Department of Medicine, University of Minnesota, Minneapolis, MN, United States, 3Department of Radiology, University of Minnesota, Minneapolis, MN, United States, 4Division of Hematology, Oncology and Transplantation, Department of Medicine, University of Minnesota, Minneapolis, MN, United States
Synopsis
Retrospective respiratory gating using a 3D time series lung image reconstructed with sub-second temporal resolution is introduced to achieve accurate small pulmonary nodule detection with ultrashort echo time (UTE) MRI. Changes of the diaphragmatic level during free breathing were tracked using the 3D time series lung image. With the extracted respiratory motion, the data in exhalation were reconstructed to a high resolution image. The feasibility and robustness of the proposed retrospective gating method were tested by surveilling incident lung nodules in two UTE MRI examinations: a baseline scan and a follow-up scan in 10 weeks.
Purpose
Incidentally detected lung nodules are common in clinical CT such as neck CT, cardiac CT and chest CT1. Although the majority of the nodules are benign, they need to be surveilled with CT in a regular basis to confirm their stability, which results in an increased exposure to ionizing radiation. Ultrashort echo time (UTE) MRI is a promising technique for pulmonary imaging due to its extremely high sensitivity to fast-decaying signals and the inherent tolerance to motion artifacts. Reliable lung nodule surveillance with UTE MRI can eliminate the radiation risk associated with repeated follow-up CT imaging. However, since motion during UTE acquisition results in image blurring, adequate respiratory motion management is essential to detect small pulmonary nodules (e.g. 3-5 mm in diameter). In this study, we introduce a retrospective respiratory gating method for small lung nodule detection that uses a 3D time series lung image to accurately track diaphragmatic motion during the MRI scan.Methods
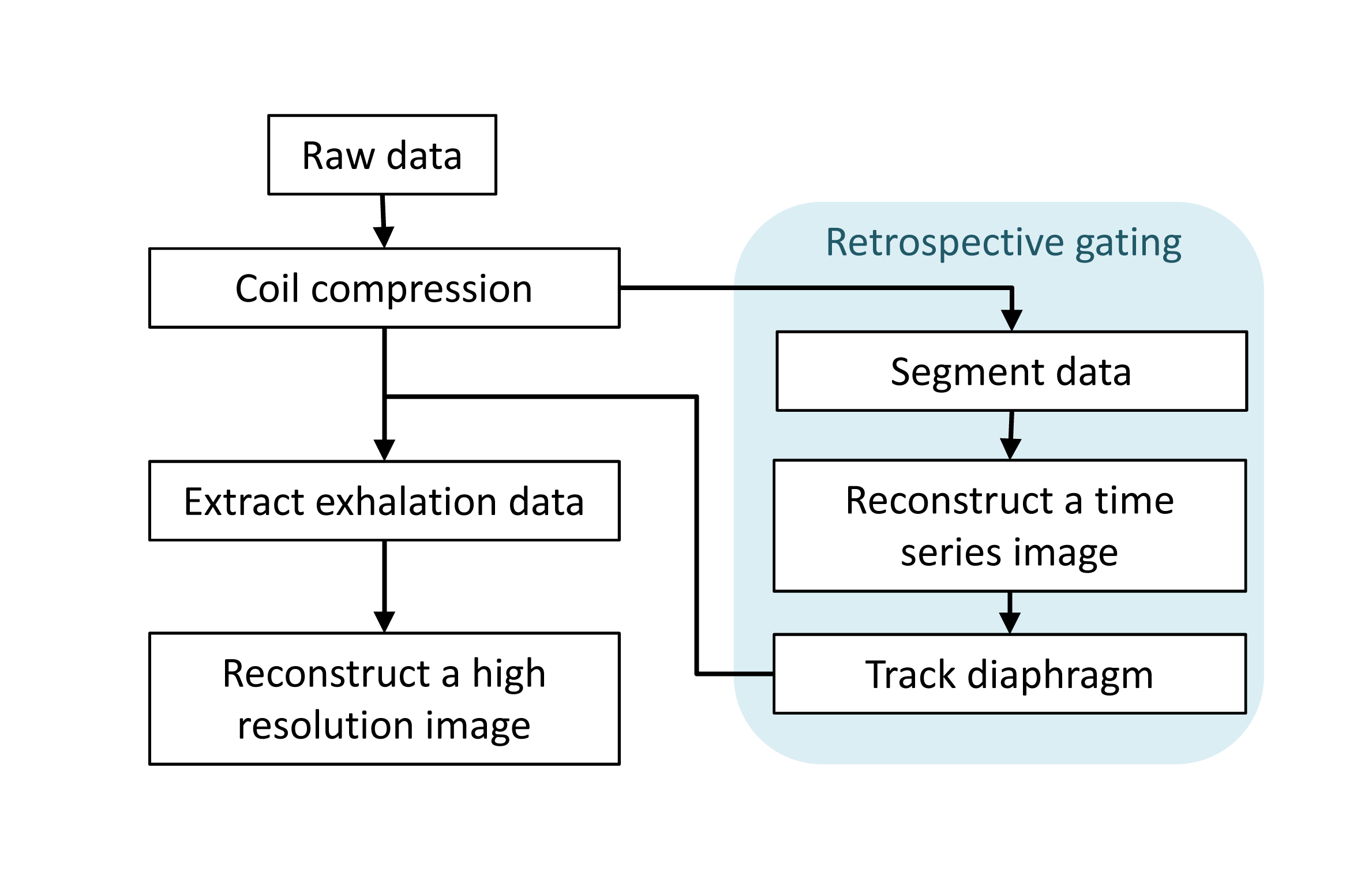
MR imaging in this study was performed with a 3T Siemens Prisma scanner. Lung imaging data were acquired on healthy volunteers (N=4) under an IRB approved protocol. In UTE data acquisition, 3D radial k-space data were acquired following slab selective excitation with a minimum phase Shinner-Le Roux pulse2, which provided TE=110 μs. UTE sequence parameters were as follows: TR=2.5 ms, flip angle=5°, fat saturation inserted every 128 TRs, number of radial views=111,616 and scan time=5 min. A 3D spherical k-space was sparsely sampled every 256 views (0.68 sec). During the MRI scan, subjects breathed freely. Image reconstruction was performed following the image reconstruction pipeline (Fig.1). The acquired data were compressed by coil compression3 and then sent to the retrospective respiratory gating pipeline. The data were segmented to 436 temporal frames (256 views each) to extract respiratory motion. The segmented data were reconstructed to a 3D time series lung image, I, by iteratively minimizing the following equation: $$$I=\arg\min_{x}\left\{\frac{1}{2}\cdot\mid s-Ex\mid_2^2+\lambda_sTV_s(x)+\lambda_tTV_t(x)\right\}$$$, where s is the segmented k-space data, E is the encoding matrix and TVs,t and λs,t are total variation operators and regularization parameters along spatial or time dimension, respectively. Stronger regularization was applied in time dimension. With the reconstructed time series image, breathing motion was extracted by tracking the diaphragm level. Based on the diaphragm motion, the data in exhalation were extracted with an acceptance ratio of 40 % and reconstructed to a high resolution 3D image with a 0.7 mm isotropic nominal resolution. To test the ability of the proposed retrospective respiratory gating to detect small nodules, we performed two UTE MRI examinations for a subject who had small incident solid, non-calcified nodules in the lung: a baseline scan and a follow-up scan in 10 weeks.Results
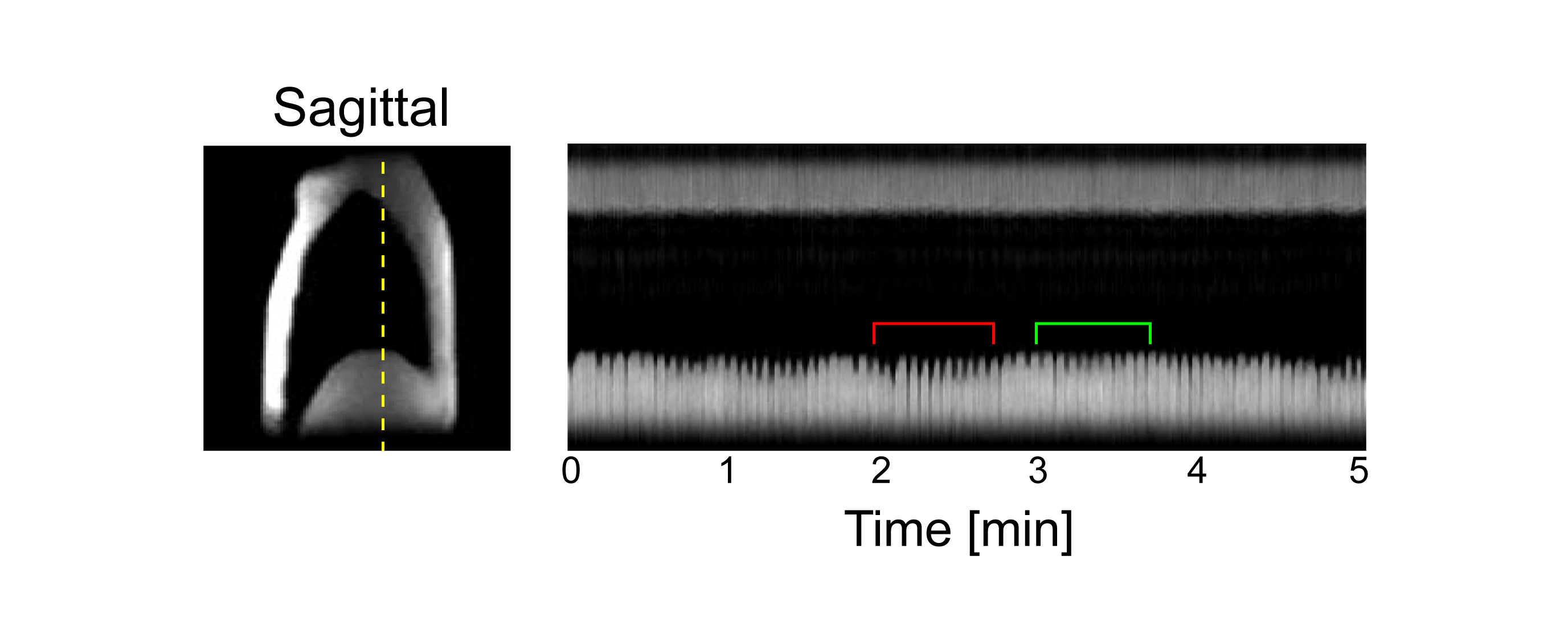
The 3D time series lung image with 0.68 sec temporal resolution nicely captured diaphragmatic motion associated with free breathing (Fig.2); changes of diaphragm level showed fluctuation of breathing depth and rate during the 5 min scan. Breathing motion is relatively stable in exhalation, but the diaphragmatic level was not always consistent with free breathing. A high resolution lung image in exhalation was reconstructed using the diaphragmatic motion extracted from the time series image (Fig.3). The maximum intensity projection image from the image reconstructed with retrospective gating visualized the fine structure of the lung vasculature. Although radial UTE does not show clear motion artifacts without motion management, there was notable image blurring observed in the image without respiratory gating especially around the diaphragm.
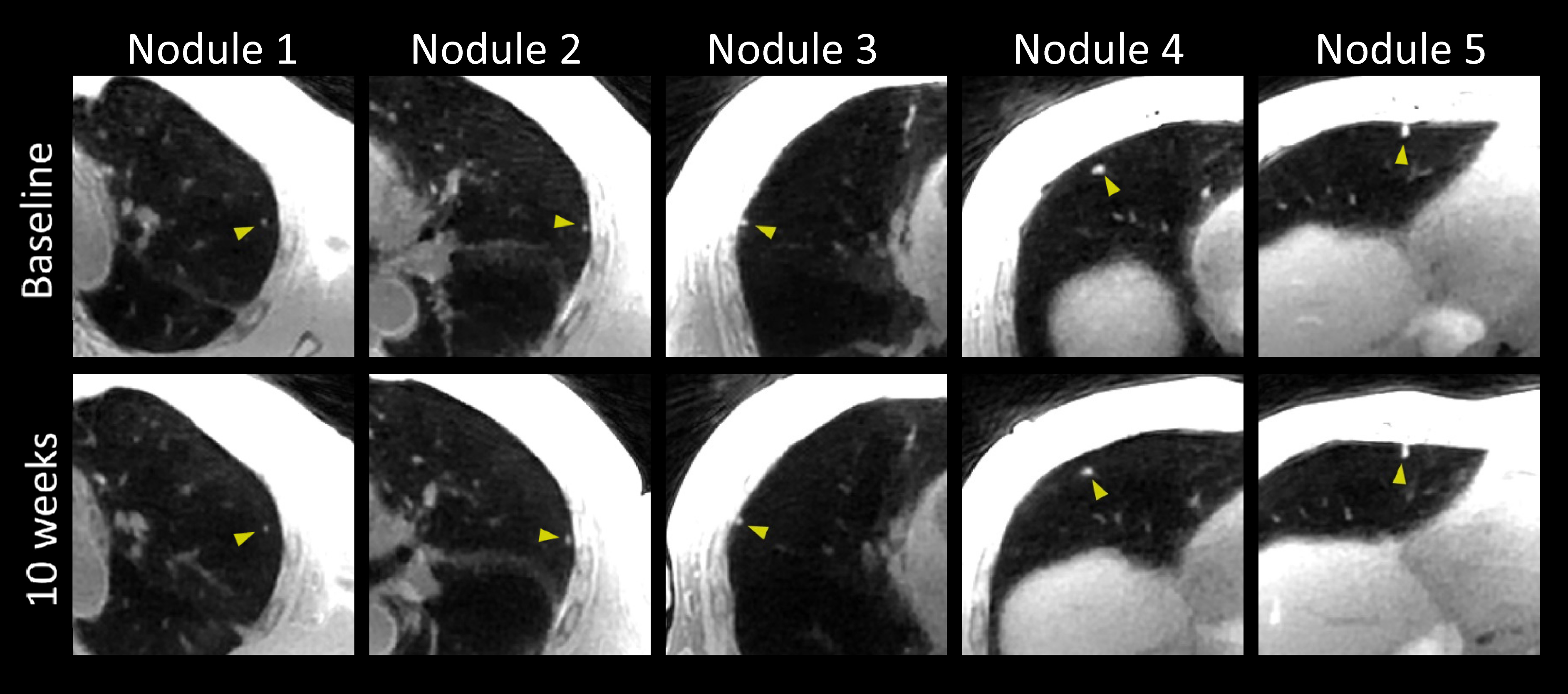
There were five incident nodules in size of 3-7 mm in diameter detected with UTE MRI in the lung of one subject (Fig.4). The five nodules showed stable behavior in the follow-up imaging performed in 10 weeks after the baseline MRI, which indicated the incident nodules are likely to be benign.
Discussion
In this study, we introduced retrospective respiratory gating using a 3D time series image with 0.7 second temporal resolution. Since the normal breathing rate is in a range of 3-6 sec/breath, sampling with an interval of 0.7 second is sufficiently high to capture breathing motion. Tracking of diaphragmatic level enables more precise motion management compared to simple detection of respiratory phase (inhalation or exhalation). Moreover, motion detection with 3D imaging can detect aperiodic contingent motion such as bulk motion of the body, which is useful for correcting or eliminating the deleterious motion effects in image reconstruction.Conclusions
UTE MRI with the proposed retrospective gating may enable accurate detection and surveillance for clinically relevant lung nodules, which could allow more frequent surveillance, for example, for highly suspicious nodules without ionizing radiation.Acknowledgements
This study was supported by NIH grant P41EB015894.References
1. MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology. 2017;284(1):228-43.
2. Pauly J, Le Roux P, Nishimura D, Macovski A. Parameter relations for the Shinnar-Le Roux selective excitation pulse design algorithm [NMR imaging]. IEEE transactions on medical imaging. 1991;10(1):53-65.
3. Buehrer M, Pruessmann KP, Boesiger P, Kozerke S. Array compression for MRI with large coil arrays. Magnetic resonance in medicine. 2007;57(6):1131-9.
Figures