4345
Clinical Feasible Breath-Hold Lung Imaging Using Zero Echo Time MRI1GE Healthcare, Taipei, Taiwan, 2Department of Radiology, Wang Fang Hospital, Taipei Medical University, Taipei, Taiwan, 3Department of Radiology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
Synopsis
A high resolution, rapid scanning in one breath-hold and three-dimensional zero-echo time protocol for lung imaging was established in this study. It successfully captured rapid-decaying lung signal and eliminated the motion artifact and consequently exhibit high quality of pulmonary anatomy, including the tortuous vessels architecture and bronchial wall in exceptional clarity and detail. Additionally, it provides the volume estimation of pulmonary tissue and shows somewhat comparable with the calculation result from computed tomography.
Purpose:
Computed Tomography (CT) is the imaging method of choice for assessing pulmonary tissue in clinical practice. In contrast, magnetic resonance imaging (MRI) of lung is extremely challenging because of several shortcomings, including low signal to noise ratio due to low proton density and short signal life times (T2* ~ 0.5 -3 ms) in lung tissue, artifacts relate to the prominent susceptibility difference between air and soft tissue, and respiratory motion artifacts1,2. A novel MRI technique named zero-echo time (ZTE) has been recent developed2. It utilizes hard pulse excitation followed by immediately three-dimensional (3D) radial sampling to achieve nominal TE of zero and consequently could provide efficient sampling short T2* signals in lung tissue. The aim of this study is to establish a clinical feasible lung imaging protocol which can capture rapid decay lung signal with minimal artifact in evaluating pulmonary tissue using ZTE MRI.Methods:
All MRI acquisitions were performed on a 3T clinical scanner (Discovery MR750w, GE Healthcare, Milwaukee, USA) using a large-size 16-channel flexible array coil as the signal detection covering chest region and whole body coil for radio-frequency excitation. ZTE data were acquired using a non-selective hard pulse excitation followed by 3D center-out radial sampling. The scanning parameters were as follows: TR=283 ms, flip angle=1 degree, receiver bandwidth= 62.5 kHz, field-of-view= 26 cm:, isotropic resolution= 2 mm (interpolated to 0.51 × 0.51 × 1 mm), scan time= 27 s. Three-dimensional view of lung imaging was generated on an Advantage Windows workstation using an advanced visualization platform (READY View (ver.4.7), GE Healthcare). Lung regions were automatically segmented using auto thresholding method (ImageJ, NIH, Maryland, USA). The calculation of pulmonary volume was conducted with homemade program (MATLAB 2003).Results:
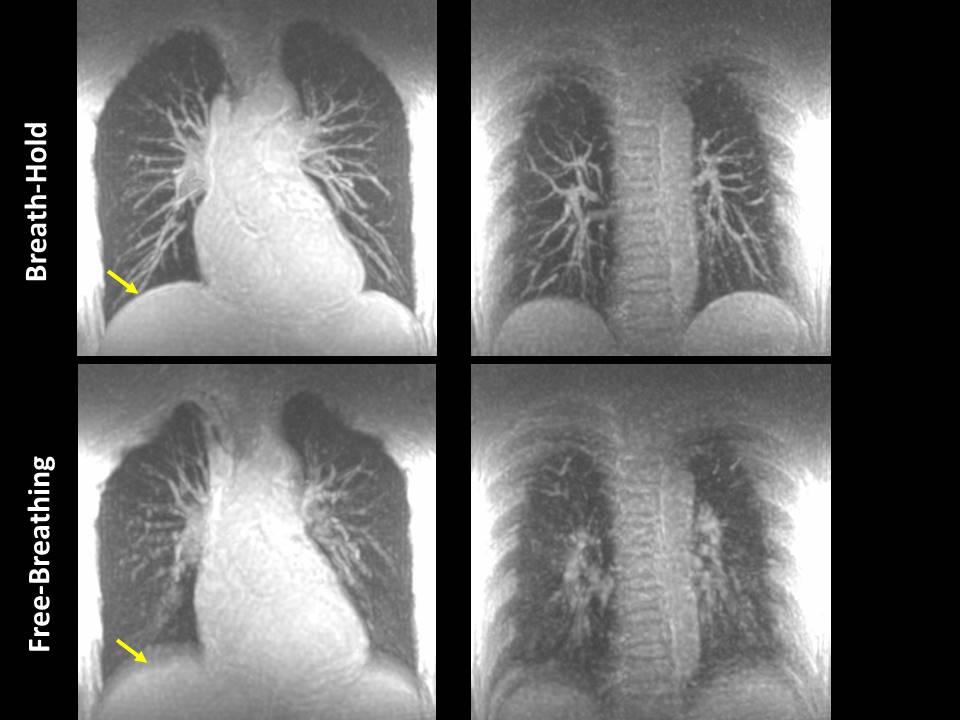
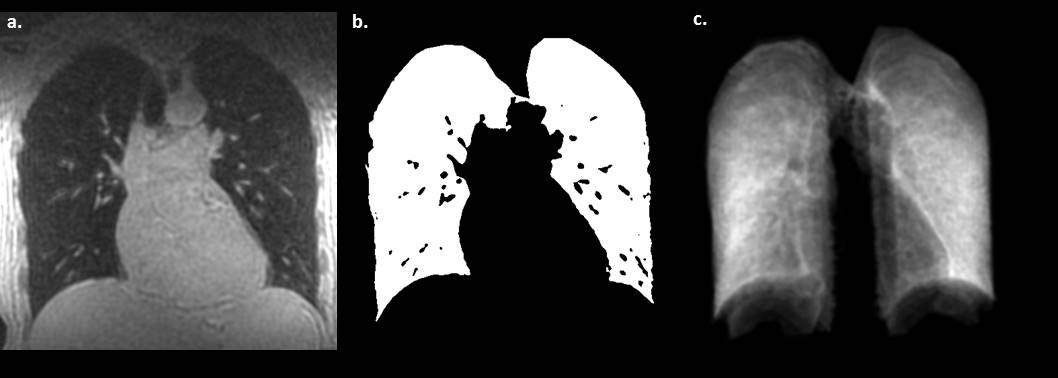
Lung ZTE MRI of a representative volunteer obtained with free-breathing (FB) and breath-hold (BH) at same acquisition time was shown in Fig. 1. Compared to FB lung ZTE, BH lung imaging showed high-quality of pulmonary anatomy, including the tortuous vessels architecture and bronchial wall in exceptional clarity and detail. In addition, the respiratory motion was successfully eliminated in BH lung ZTE, as demonstrated by sharp lung structures and evident diaphragm edge (yellow arrow indicated). In the raw data of ZTE, with proper setting of intensity threshold, pulmonary tissue can be easily identified due to the great contrast between lung and other tissues (Fig.2). After segmentation, the volume of lung region was calculated and was 3057.2 cm3 (left lung: 1450.6 cm3 and right lung=1606.6 cm3). This value is similar with the data obtained by CT3 (Haas M et al., figure 1).Discussion and Conclusion:
In this study, high resolution, rapid scanning in one breath-hold and 3D ZTE protocol was established. We herein reported, for the first time, better-than-expected results in depicting details of whole lung anatomy, with minimal artifacts. It also allows whole lung volume estimation, in combination with automatic lung segmentation and its volume determination is comparable with the result obtained by CT data3. This clinical feasible ZTE MRI setting provides alternative radiation-free diagnostic option that is especially relevant to young and pregnant patients, as well as selective subjects who need to undergo repeated examinations for evaluation of the course of lung disease and monitoring of the therapeutic response.Acknowledgements
No acknowledgement found.References
1. Kurihara, Y et al., “MRI of Pulmonary Nodules,” AJR, 202:W210-216, 2014.
2. Gibiino, F, et al., “Free-breathing, zero-TE MR ling imaging,” Magn Reson Matter Phy, 28:207–215, 2015.
3. Haas, M, et al., “Automated Lung Volumetry from Routine Thoracic CT Scans,” Acad Radiol, 21:633-638, 2014.
Figures