4323
Ultrafast dynamic contrast-enhanced MRI of the breast: Correlations with prognostic factors of breast cancer.Ken Yamaguchi1, Takahiko Nakazono1, Ryoko Egashira1, and Hiroyuki Irie1
1Department of radiology, Saga university, Saga City, Japan
Synopsis
- The purpose of our study is to determine the correlation between the parameters obtained from ultrafast dynamic contrast-enhanced (ultrafast DCE) MRI and prognostic factors of breast cancer.
- Fifty five breast cancers were included in this study. Ultrafast DCE sequence was performed using higher than usual parallel imaging factor and obtained with 8.3 second temporal resolution. Kinetic parameters obtained from ultrafast DCE were compared with prognostic factors.
- Mean maximum slope of invasive cancer (10.2) was significantly higher than that of DCIS (8.2).
- Ultrafast DCE MRI is useful for differentiating DCIS and invasive breast cancer.
Introduction
Recently, ultrafast dynamic contrast-enhanced (ultrafast DCE) MRI has been developed because of its very high temporal resolution1-4. According to recent several studies, its diagnostic performance for breast cancer is equal to superior compared to conventional breast MRI1-4. However no study has established the relationship between ultrafast DCE findings and prognostic factor of breast cancer. The purpose of our study is to determine the correlation between the parameters obtained from ultrafast DCE and prognostic factors of breast cancer.Materials and Methods
This retrospective study was approved by institutional review board. From May 2016 to April 2017, 87 patients with 95 surgically proved breast lesions were performed breast MRI including ultrafast DCE sequence. Of these, benign cases, cases performed neoadjuvant chemotherapy before surgery, cases without complete pathological data and cases with technical error were excluded. Thus, 52 patients (median age; 59) with 55 breast cancers (median size; 19mm) were included in this study. All examinations were performed using a 3T MR system (Magnetom Prisma, Siemens Healthcare, Erlamgen, Germany) with a dedicated 18 channel breast coil. Ultrafast DCE sequence was performed using higher than usual parallel imaging (GRAPPA) factor and its spatial resolution was 0.9x0.9x2.5mm. Its sequence was just started with contrast enhancement material injection and obtained 12 phases with 8.3 second temporal resolution. Enhancement ratio at each time point, area under the curve (AUC) of the kinetic curve at each time point and maximum slope based on the steepest part of the kinetic curve were obtained from dedicated workstation (PM view, JMAC systems) and compared with prognostic factors, including invasive component status (ductal carcinoma in situ [DCIS] or invasive cancer), hormone receptor (estrogen receptor [ER] and progesterone receptor [PgR]) status, human epidermal growth factor receptor 2 (HER2) status, proliferative marker (ki 67) status, nuclear grade, intrinsic subtype, and lymph node status. T-test, one way ANOVA test and Pearson’s correlation test were used for statistical analysis. P-value < 0.05 was considered significant.Results
Mean maximum slope of invasive cancer (10.2) was significantly higher than that of DCIS (8.2) (Figure1-3). Mean enhancement ratio at first phase of HER2 negative cancer (81.1%) tended to be higher than that of HER2 positive cancer (54.2%) but there was not significant correlation (P=0.07). Other prognostic factors were not significant correlated with kinetic parameters of ultrafast DCE MRI.Conclusion
Ultrafast DCE MRI is useful for not only differentiating benign and malignant breast lesion but also differentiating DCIS and invasive breast cancer.Acknowledgements
No acknowledgement found.References
1: Mann RM, et al. Invest Radiol. 2014 Sep;49(9):579-85.
2: Abe H, et al. AJR Am J Roentgenol. 2016 Nov;207(5):1159-1166.
3: Mus RD, et al. Eur J Radiol. 2017 Apr;89:90-96.
4: Onishi N, et al. J Magn Reson Imaging. 2017 May 28.
Figures
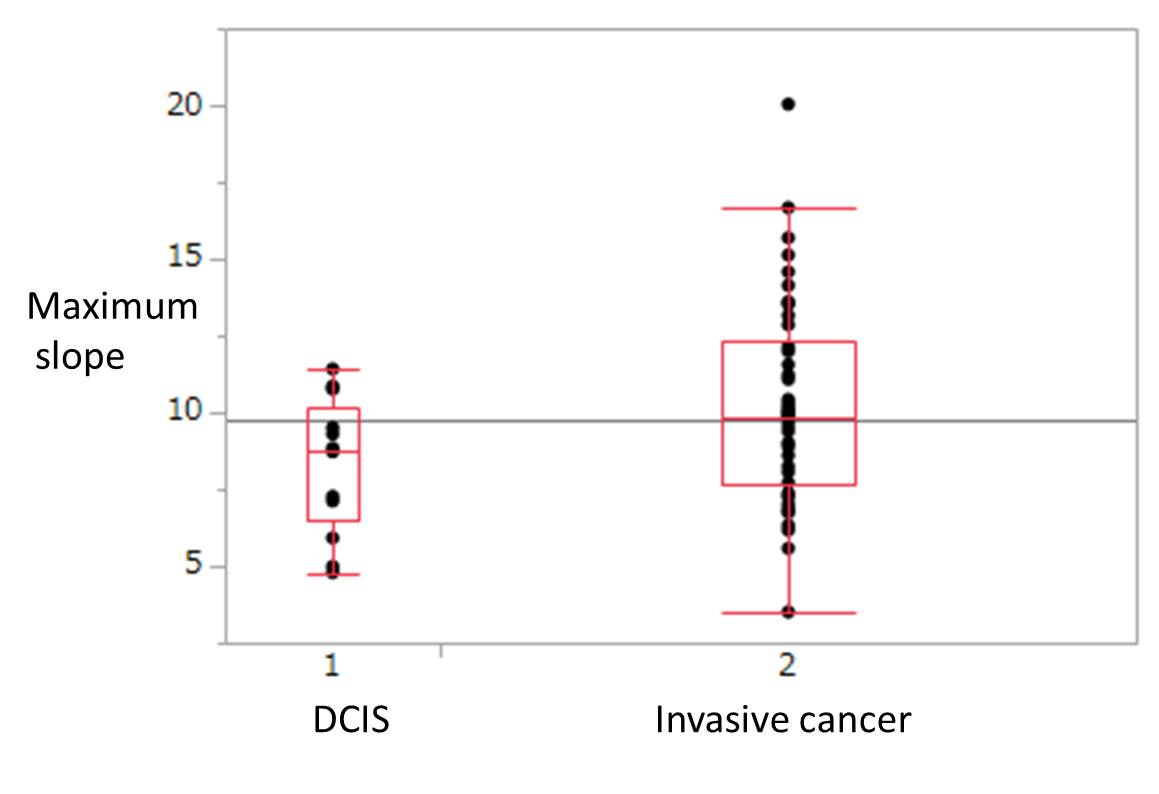
Mean
maximum slope of invasive cancer (10.2) was significantly higher than that of DCIS
(8.2).
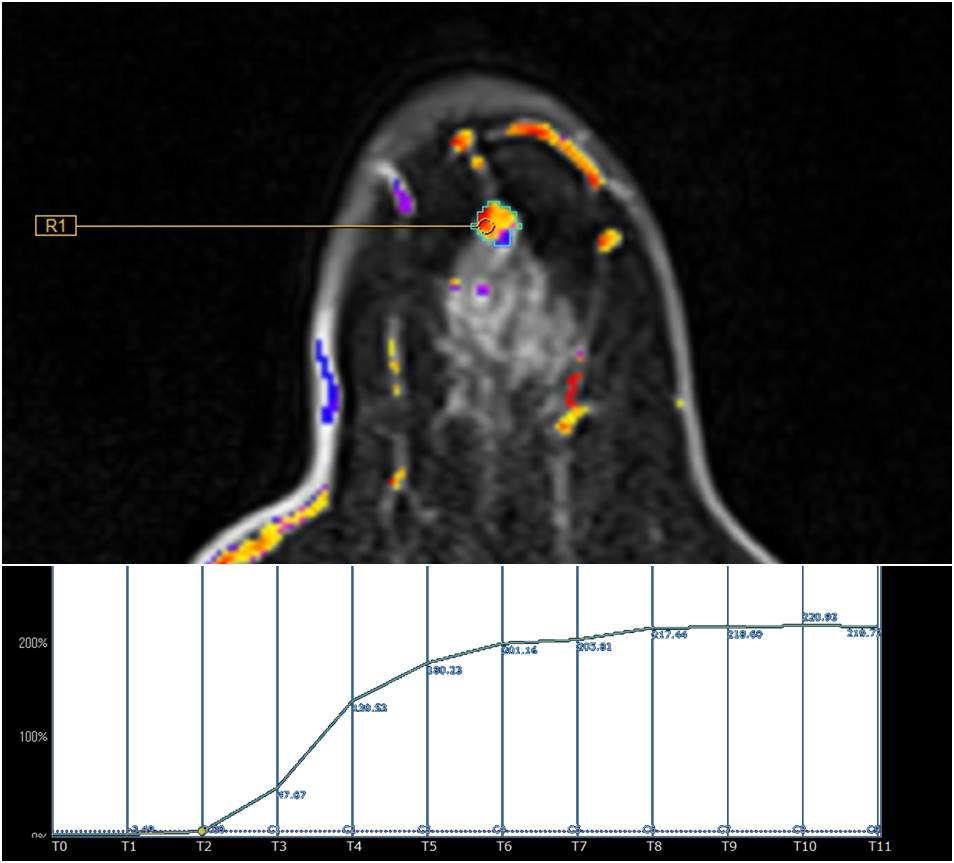
A 69-year-old woman with ductal carcinoma in situ (DCIS). Figure shows time intensity curve of ultrafast DCE and its maximum slope was 8.72.
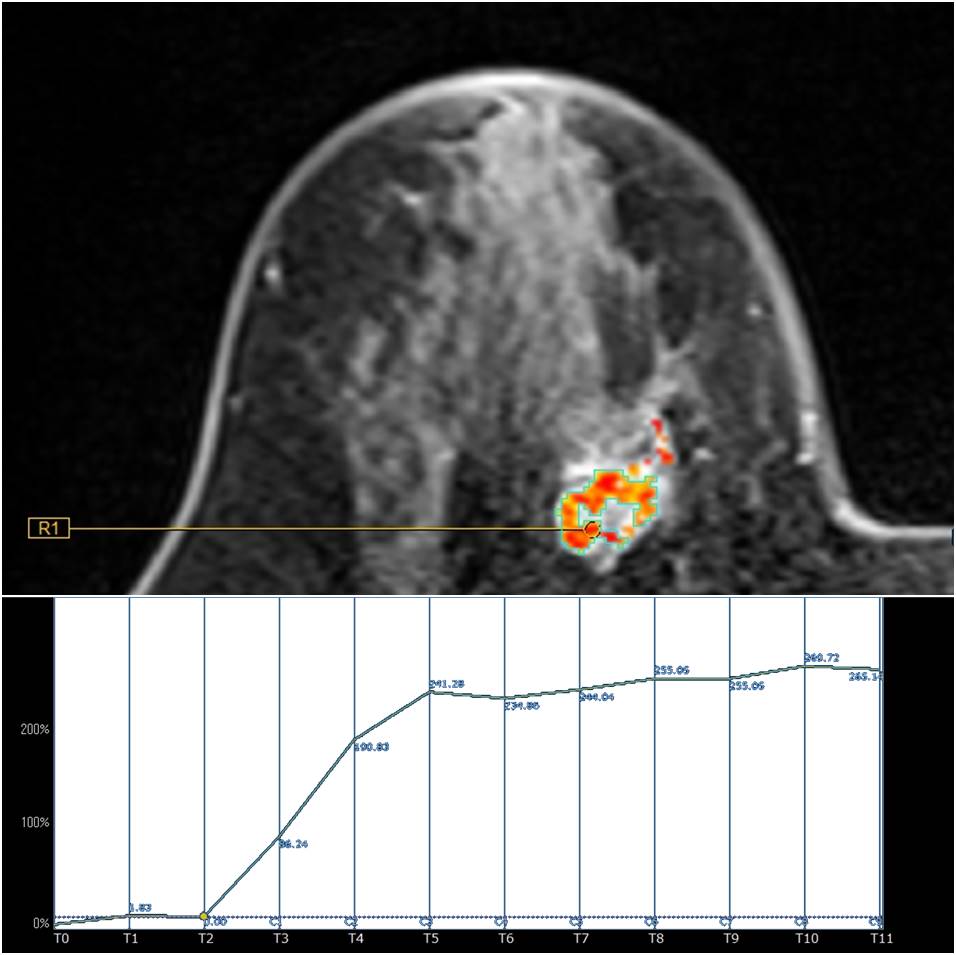
A 61-year-old woman with invasive ductal crcinoma. Figure shows time intensity curve of ultrafast DCE and its maximum slope was 11.23.