4321
Repeatability of Diffusion-Weighted Imaging Model Parameters within a Benign Breast Cancer Cohort Influences Optimal Model Choice1Department of Circulation and Medical Imaging, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 2Clinic of Radiology and Nuclear Medicine, St. Olavs University Hospital, Trondheim, Norway, 3Department of Physics, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 4Department of Cancer Research and Molecular Medicine, Norwegian University of Science and Technology - NTNU, Trondheim, Norway, 5Department of Surgery, St. Olavs University Hospital, Trondheim, Norway
Synopsis
Diffusion-weighted MR imaging (DWI) is an essential tool in oncology. Diffusion models beyond monoexponential fitting attempt to capture non-Gaussian decay using additional data acquisition. Model repeatability and suitability is critical, but often neglected. We report findings from fitting multiple diffusion models in a benign breast cancer repeatability cohort, and show no clear dominance of diffusion models across voxels, patients, or scans. Repeatability of ADC, IVIM, and stretched exponential parameters are reported, and highlight the complexity of making inferences from DWI parameters.The potential of DWI in oncology is tempered by a need for critical appraisal of the model and parameter applicability.
Introduction
Diffusion-weighted imaging (DWI) for oncology is a powerful tool, giving volumetric, non-invasive, microstructure-sensitive information on disease extent and character using only endogenous contrast. Tissue diffusion models beyond simple monoexponential fitting (for apparent diffusion coefficient, ADC) attempt to capture non-Gaussian diffusion behaviour, requiring specific acquisition strategies of multiple b-values and/or directions; repeatability and suitability of these models is critical for robust DWI biomarkers, however, and is often not examined1. In this study, we report the findings from fitting multiple diffusion models to a multiple b-value DWI protocol in a benign breast cancer repeatability cohort, and highlight the complexity of making inferences from derived DWI parameters.Methods
This prospective study was approved by the regional committee for medical and health research ethics. Informed, consented patients with confirmed benign breast lesions were recruited between Sep 2016 and Oct 2017. Alongside standard anatomical and contrast-enhanced imaging (DCE), clinical MRI examination included a multiple b-value DWI protocol, repeated in an additional scan approximately 1 week later. DWI acquisition parameters included: unilateral sagittal orientation, SE-EPI (bipolar encoding), TR/TE: 11600/86ms, FOV: 180x180mm, matrix: 90x90, slice thickness: 2.5mm, slices: 60, iPAT: GRAPPA 2, b-values: 0, 10, 20, 30, 40, 50, 70, 90, 120, 150, 200, 400, 700 s.mm-2, with additional phase-reversed b=0 scan for distortion correction2. Total DWI scan time: 9 minutes.Analysis
Diffusion images were corrected for distortion using the method described by Teruel et al2; volumes of interest (VOIs) were drawn for all slices of the benign tumour in each scan (on diffusion images, using DCE and T2 as reference). Multiple DWI models, including monoexponential (giving apparent diffusion coefficient ADC), biexponential IVIM (giving volume fraction f of two diffusion coefficients D and D*), and stretched exponential (giving stretching exponent α and distributed diffusion coefficient DDC), were fitted voxel-wise using all b-values, and for mean VOI signal, using a Levenberg-Marquardt algorithm with segmented approach providing initial IVIM values3. The optimal model for each fitting was determined by Akaike information criterion (AIC). Repeat-measure coefficients of variation (CoVs) were calculated for all DWI parameters across the VOI histogram.Results
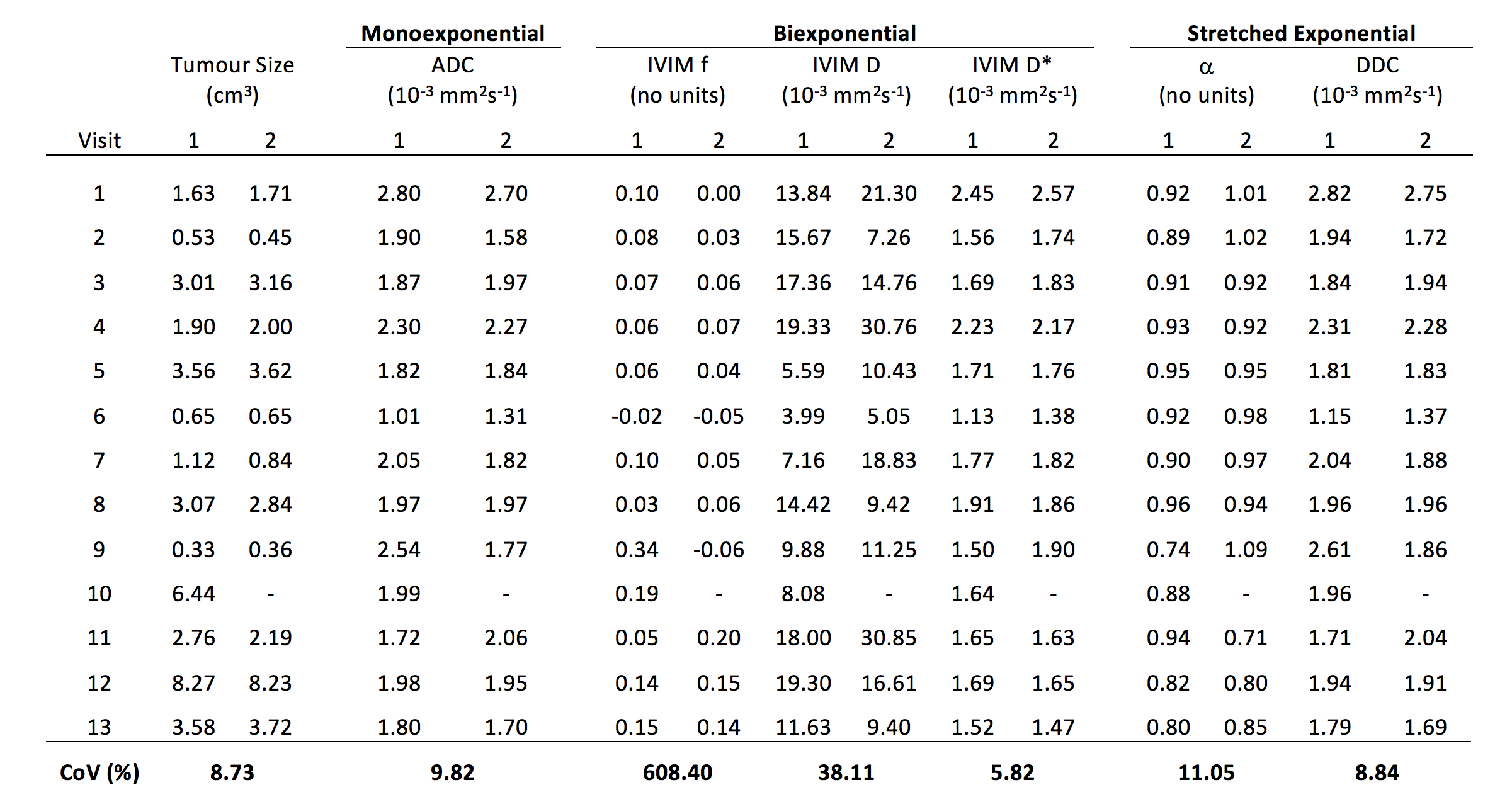
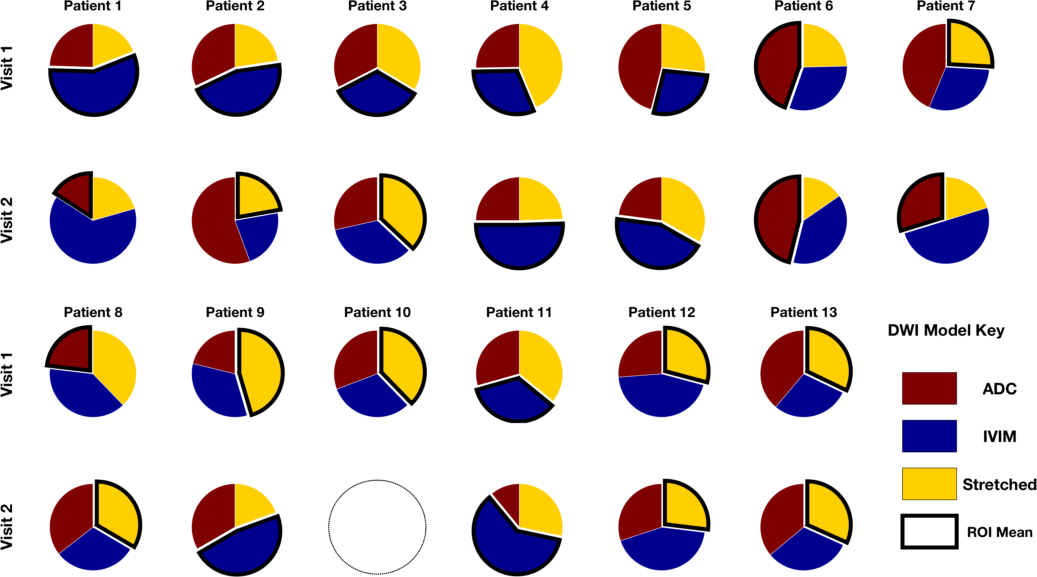
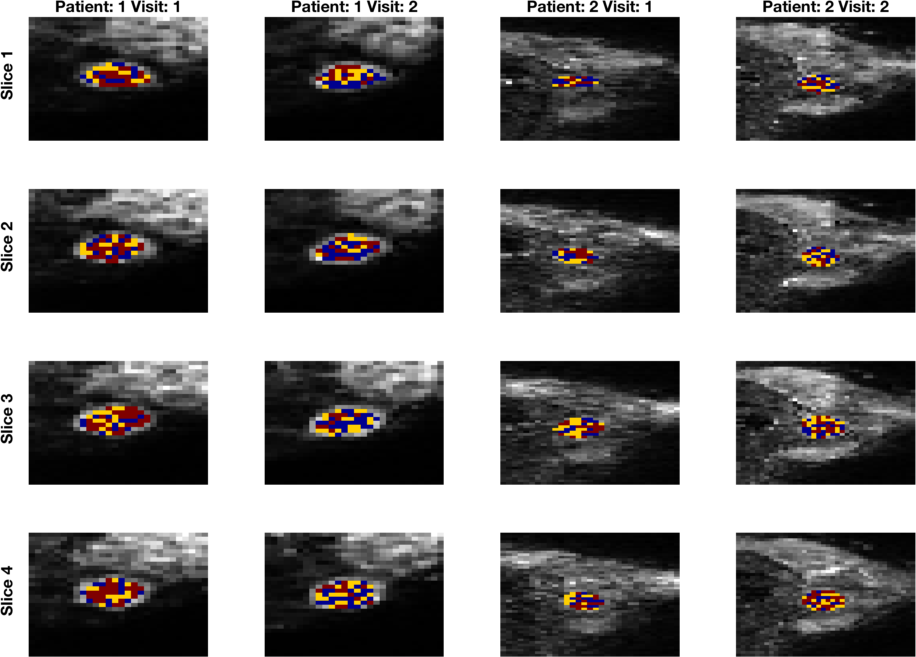
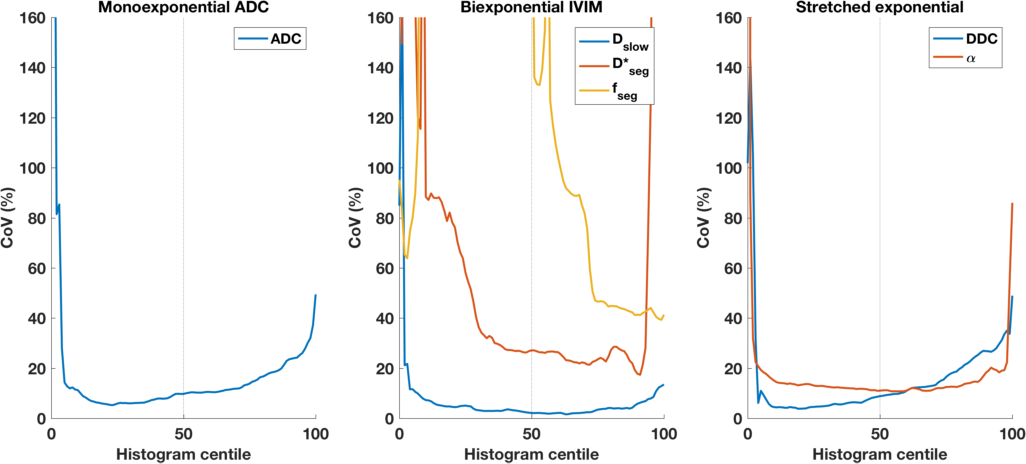
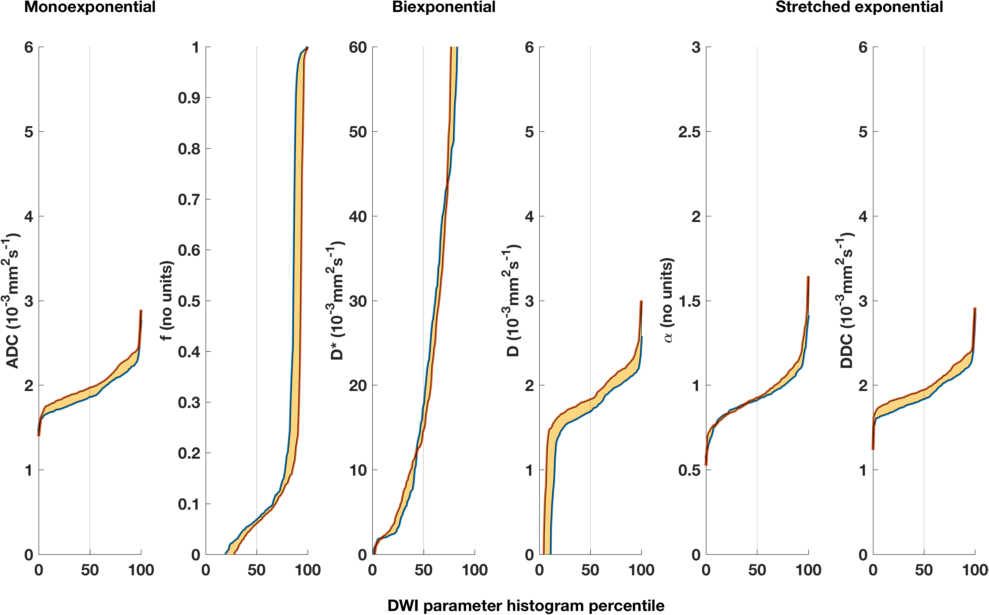
Thirteen patients (median age 24, range 19-50 years) underwent DWI; one patient withdrew following 1 scan, giving 12 repeated datasets. Benign lesions ranged from 0.345 to 8.25cm3, with volume CoV of 8.7%, indicating good VOI repeatability. For full tumour characteristics see Table 1. Figure 1 shows DWI model comparison for all voxels, as well as for mean signal (outlined segment); within each tumour, the diffusion decay curves are not dominated by a single model, and in all patients all models are represented (Figure 2; colours as Figure 1). In all cases, a substantial proportion of voxels are best described by the monoexponential ADC model, with the remainder indicating that while some non-Gaussian diffusion behaviour is observed, the cohort data does not appear to be best described by either IVIM or stretched exponential. Averaging the VOI signal before modelling gives a lower AIC for non-Gaussian models in a majority (80%) of the DWI acquisitions in the study. Interestingly, there was little concordance of dominant model, for either voxel-wise or from VOI-summary DWI fitting, across repeated visits. CoVs for all DWI parameters (median across voxels) are given in Table 1; for diffusivity measures such as ADC, D, and DDC, CoV is low (<10%). For other parameters, CoV is substantially higher (>20%), with the exception of the stretching exponent α, a measure of non-Gaussian character influenced by the entire data range (unlike IVIM f and D*). Figure 3 displays these CoVs for each parameter across each centile, illustrating stability of diffusivity-related parameters (ADC, D, and DDC) as low as 5th histogram percentile, which may indicate regions with highest cellular density. Figure 4 illustrates repeated parameter values from a typical dataset, illustrating non-physiological behaviour of IVIM parameters (negative f values, f ranging up to1, negative D) that indicates that fitting of the IVIM model is neither especially robust, nor necessarily appropriate in this cohort.Discussion
Assumptions for DWI modelling, including model and algorithm choices, are not always valid; the great potential of advanced DWI in oncology is tempered by a need for critical appraisal of the model applicability. These data demonstrates the complexities of interpreting clinical DWI, although this study represents a small cohort of benign breast lesions, which should be borne in mind for ongoing studies that will examine larger cohorts including malign lesions. Repeatability assessments in suitable context are essential in order to fully realise the potential, and understand the shortcomings, of more complex DWI biomarkers in the clinical setting.Acknowledgements
We acknowledge support from the liaison Committee between the Central Norway Regional Health Authority and the Norwegian University of Science and Technology.References
1. Jerome NP, Miyazaki K, Collins DJ, et al. (2017) Repeatability of derived parameters from histograms following non-Gaussian diffusion modelling of diffusion-weighted imaging in a paediatric oncological cohort. Eur Radiol 27:345–353.
2. Teruel, J. R. et al. Inhomogeneous static magnetic field-induced distortion correction applied to diffusion weighted MRI of the breast at 3T. Magn. Reson. Med. 74, 1138–1144 (2015).
3. Vidic, I. et al. Support Vector Machine for Breast Cancer Classification Using Diffusion-Weighted MRI Histogram Features : Preliminary Study. 1–12 (2017). doi:10.1002/jmri.25873
Figures