4294
RF Shimming and Improved SAR Safety for 16-Channel Transmit/Receive RF Coil Arrays for Cardiac MRI at 7T1Chair of Cellular and Molecular Imaging, Comprehensive Heart Failure Center (CHFC), University Hospital, Wuerzburg, Germany, 2Rapid Biomedical GmbH, Rimpar, Germany
Synopsis
In this work, comprehensive high resolution EM-simulations were performed for three different 16-element transmit/receive (Tx/Rx) planar RF coil arrays loaded with the anatomical Duke human model to examine their performance in cardiac magnetic resonance imaging (cMRI) at 7T. An optimization routine has been developed in MATLAB to optimize the phases for B1+ field homogeneity with minimal local SAR values within the Duke human biological model. Before B1-shimming, all arrays demonstrated approximately the same B1+ field distributions with a pronounced higher field values near to the coil surface. With phase increments of 45° phase shift between each of the 8-element pairs, the arrays generate pronounced local SAR hot spots with maximum values of 10.3, 10.1, and 9.4 W/kg for design 1, 2 and 3, respectively. In accordance with IEC regulations, the calculated 10 g averaged SAR values were found to be within the limits and the relative hot spots were found to be below 11 W/kg. RF shimming improves the B1+ field homogeneity by 24%, 49% and 40% in the central sagittal slice for design 1, 2 and 3, respectively.
Introduction
Magnetic Resonance
Imaging (MRI) at Ultra-high Field (UHF) has been become a popular modality in specific
anatomical regions like the brain or joints to improve the signal-to-noise
ratio (SNR). Cardiac MRI (cMRI) at UHF is
still in its infancies, only relatively little technological methodology exits
in this area. At 7T, the wavelength within the object to be imaged such as the human head is
becoming smaller than the object’s dimensions which results in B1+-field inhomogeneity. Different designs of
multi-channel transmit/receive (Tx/Rx) coil arrays have been developed for cMRI
at 7T [1-5]. Optimization of the B1+-field inhomogeneity was considered a challenge
until novel transmit RF coils for cMRI were developed and new ideas of
controlling the deficiency of global amplitude and phase of the coil channels were
investigated. In addition, B0
and B1-field homogeneity
are prominently distressed when the heart is aimed to be as a region of interest.
The purpose of this study was to design, simulate, and build three different
16-element Tx/Rx coil arrays for cMRI at 7T, and to establish a workflow
for SAR and homogeneity assessment.Materials and Methods
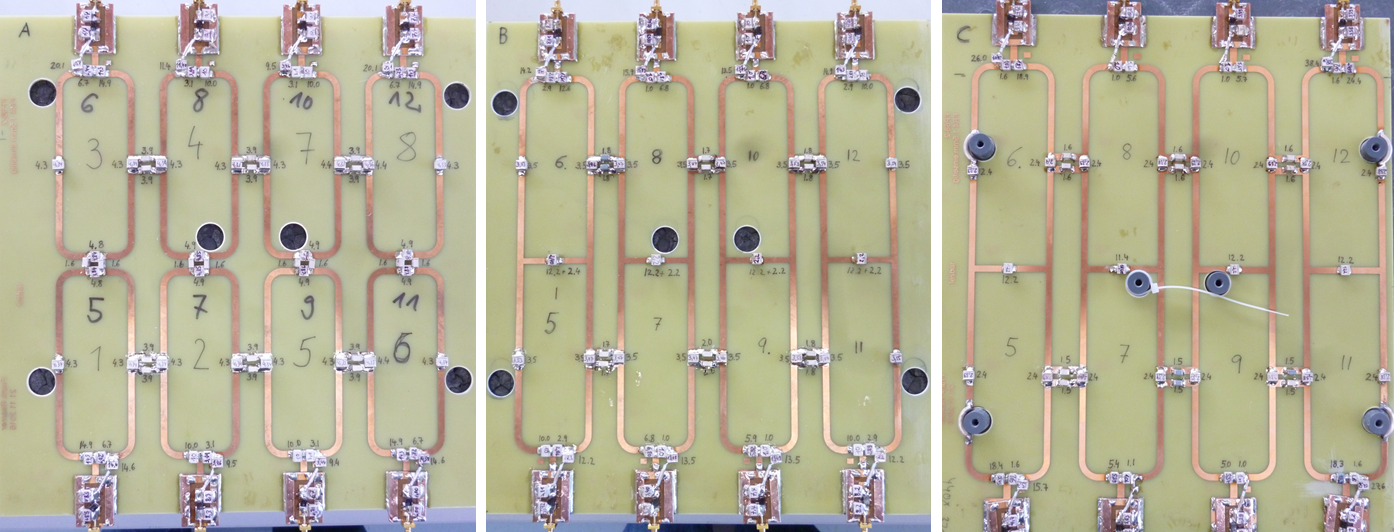
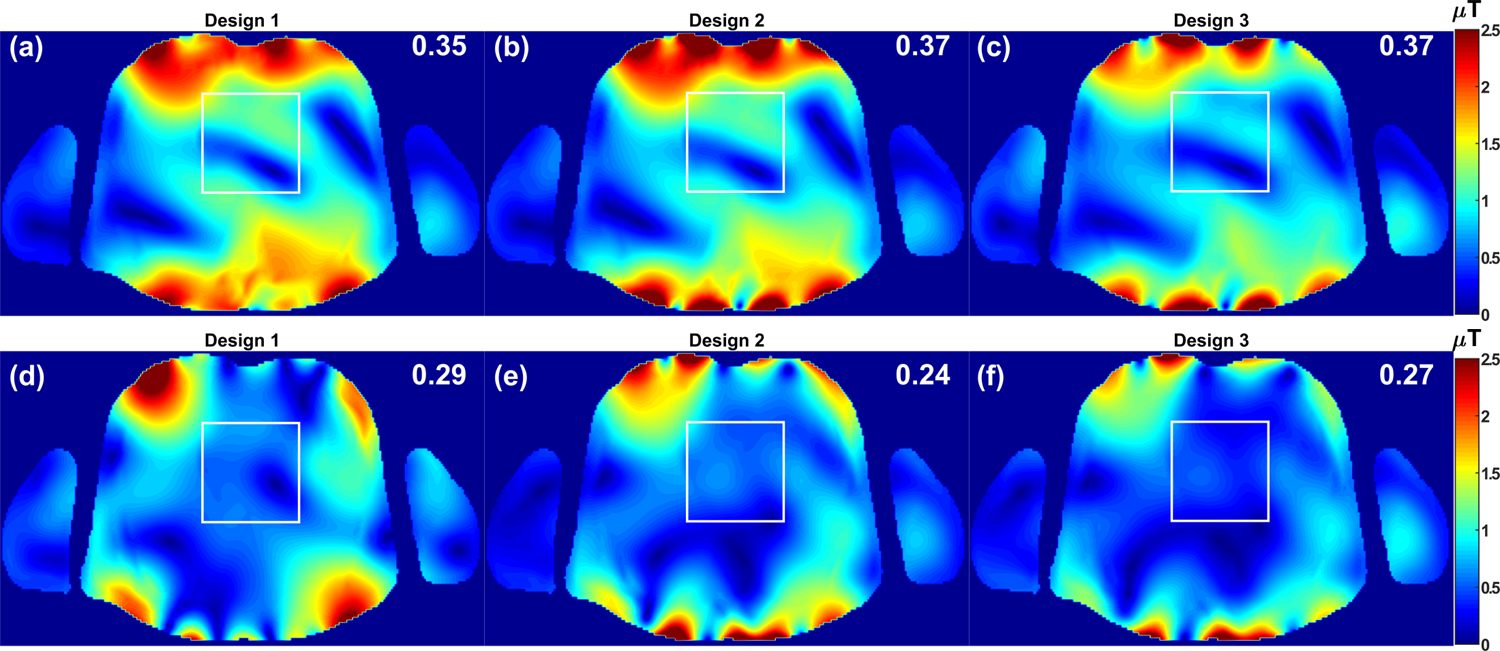
Three different 16-element coil arrays were designed, simulated and built for cMRI at 7T. Each array consists of 8-elements for anterior and 8-elements for posterior sections. Both top and bottom arrays were built using 4×2 rectangular elements. The sizes of the loops are 3.9×10.6, 3.9×11.1, and 4.5×12.7cm2 for design 1, 2 and 3, respectively. For design1, the decoupling of the adjacent coil elements were accomplished using gaps and capacitive decoupling. The adjacent coil elements were separated with vertical and horizontal gaps of 5.5 and 15mm, respectively. For design 2 and 3, the decoupling of the adjacent coil elements were accomplished using a common conductor with shared decoupling capacitor and gaps with capacitive decoupling as shown in Fig. 1. The horizontal decoupling gaps are 15.3, 15.3, and 18mm for designs 1, 2 and 3, respectively. All coil arrays were printed on 1.5mm FR4 substrate. The copper conductor has a width of 4mm and thickness of 35μm. For specific absorption rate (SAR) safety and B1+-field optimization, full-wave EM-simulations were performed for the three 16-element coil arrays using CST® Microwave Studio (Computer Simulation Technology AG Darmstadt, Germany) time-domain transient solver. RF circuit co-simulation was employed for perfect matching, tuning, and decoupling at 297.2 MHz [6]. All three arrays were loaded with the anatomical Duke human model from the Virtual FamilyTM (IT’IS Foundation, ETH Zurich) with 2×2×2mm3 resolution which results in 60-million mesh cells. The distance between the coil and the nearest tissue of the Duke model is 15mm. The local averaged 10 g SAR values were evaluated in CST using IEEE/IEC 62704-1 averaging method. All coil arrays were excited with the same stimulated power of 50W. A routine was developed in MATLAB® to homogenize the B1+-field within the heart of a ROI of 10×8×6cm3 for 1Tx mode with fixed phases with step of 22.5°. The reference phases are linearly incremented (LI) by 45° phase shift between each of the 8-element pairs. The optimization target function (Fopt) was designed to provide maximal homogeneity of histogram and flatness of penetration profile of the B1+-field in the heart and defined by Fopt =(1/RSD)*(B1+, mean/(B1+, max-B1+, median)), where RSD is the relative standard deviation which is defined as the ratio of the standard deviation to the mean value of the B1+-field. The RSD and the peak local SAR values before and after optimization are shown at the top of the image for each array.
Results and Discussions
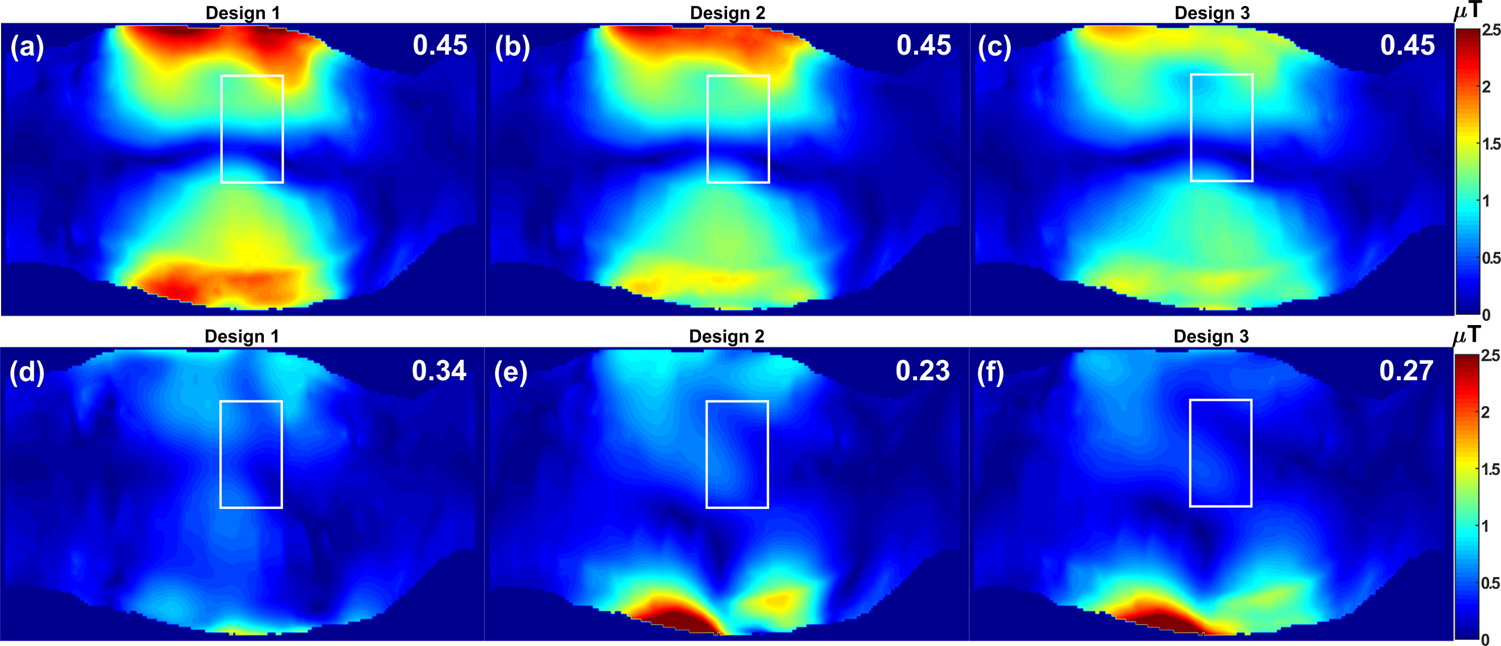
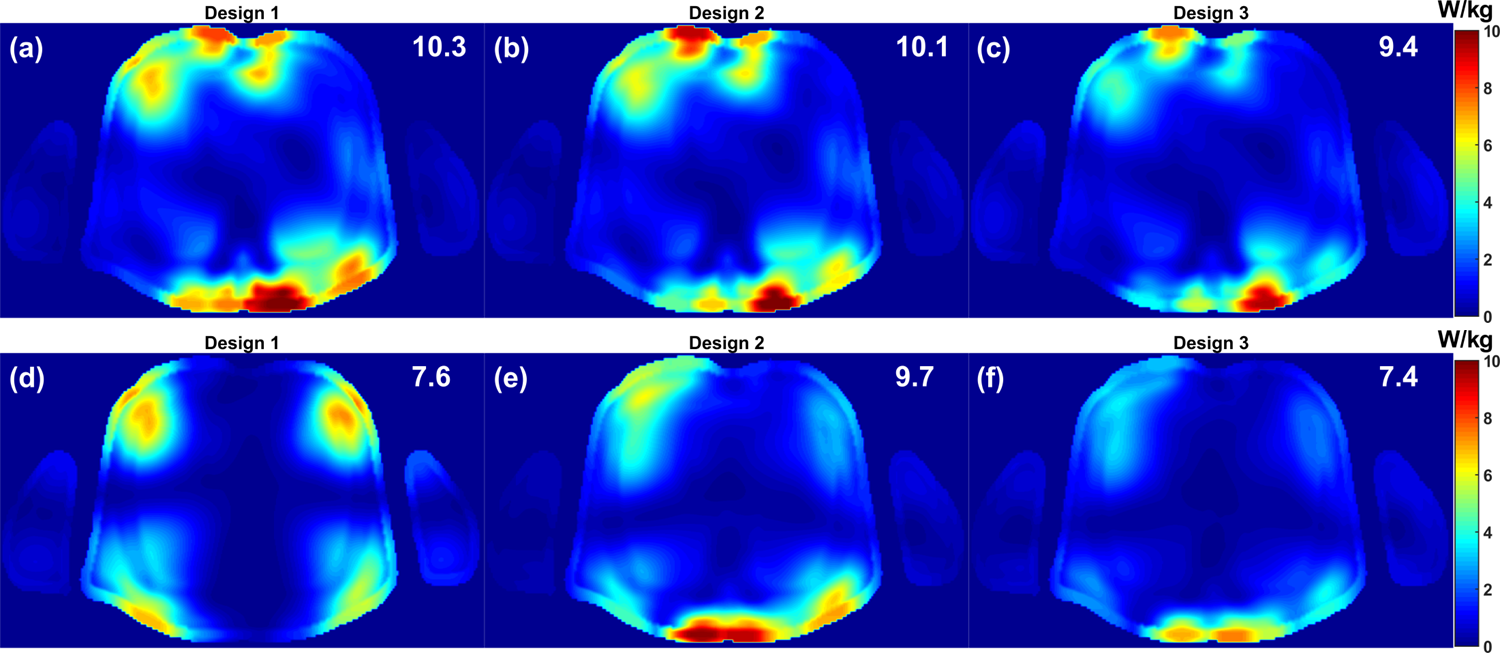
Figs. 2-4 display the simulated distributions of the B1+-field and local SAR in the central axial and sagittal slices within the Duke human model before and after optimization. Prior to B1-shimming, all arrays demonstrated approximately the same B1+-field distributions with higher B1+-field values near to the coil surface. However, design 1 has the best penetration profile within the heart with high transmission efficiency. The LI phase excitations generate pronounced local SAR hot spots with maximum values of 10.3, 10.1, and 9.4 W/kg, respectively. All SAR “hot spots” were found to be below 11 W/kg that corresponds to operation in the first level mode according to the IEC 60601-2-33 standard. For all arrays, the highest peak local SAR is pronounced in the immediate proximity to the conductor plates. RF-shimming improves the B1+-field homogeneity by 17%, 35% and 27% in the central axial slice and by 24%, 49% and 40% in the central sagittal slice for design 1, 2 and 3, respectively. Highly homogeneous B1+-field distributions were obtained with design 2 with a good penetration profile within the heart. After B1-shimming, the peak local SAR values were decreased to 7.6, 9.7, and 7.4 W/kg, respectively.Acknowledgements
Financial support was obtained from the German Ministry of Education and Research (BMBF) under grant# 01E1O1504.References
[1] Snyder et al., MRM 61, 517–524 (2009). [2] Dieringer et al., JMRI 33, 736–741 (2011). [3] Thalhammer et al., JMRI 36, 847–857 (2012). [4] Graessl et al., MRM 72, 276–290 (2014). [5] Gräßl et al., Eu J Radio 82, 752–759 (2013). [6] Kozlov et al., JMR 200, no. 1, 147–152, (2009).Figures