4227
Fast High-Resolution Endodontic MRI1Division of Radiological Physics, Department of Radiology, University Hospital Basel, Basel, Switzerland, 2Department of Biomedical Engineering, University of Basel, Basel, Switzerland, 3Department of Periodontology, Endodontology, and Cariology, University School of Dental Medicine, University of Basel, Basel, Switzerland, 4Department of Oral Surgery, Oral Radiology and Oral Medicine, University School of Dental Medicine, University of Basel, Basel, Switzerland
Synopsis
The aim of this study was to explore standard MRI hardware and sequences as an alternative radiation-free modality to Cone Beam Computer Tomography for imaging the dental root canals rapidly and with high-resolution for the planning and guidance of the bur to the root canal orifice in combination with an intraoral surface scan.
Introduction / Purpose
Pulp canal calcification (PCC) is a common sequela after dental trauma1 and is often associated with pulp necrosis and apical periodontitis2. In these cases, root canal treatment is challenging and associated with a high failure rate3. A novel method (“Guided Endodontics”) allows minimal invasive detection of these calcified root canals using printed templates guiding a bur to the root canal orifice4, 5. Beforehand, a Cone Beam Computed Tomography (CBCT) and an intraoral surface scan have to be performed. A special software allows alignment of the scans, the planning of the treatment and the design of the guidance-template. Especially young patients, who often suffer a dental trauma, have an increased biological risk after radiation exposure6, and MRI could be a promising alternative modality to CBCT. Therefore, the aim of this study was to explore standard MRI hardware and sequences in a simple and fast setup to visualize dental structures, such as in a first step, the dental root canal with high-resolution.Materials and Methods
The measurements were performed on a 3T whole body scanner (MAGNETOM Prisma, Siemens Healthineers) using a 64 channel head coil. In vivo volumetric imaging of the upper and lower jaws was performed with a balanced steady state free precession (bSSFP) sequence having a resolution of 0.4x0.4x0.8mm3 with an imaging matrix of 384x336x72. Scan time for one single bSSFP scan was 2 minutes, using parallel imaging with a factor of 2 (GRAPPA), a slice oversampling of 11%, a TR/TE of 8.29/4.14 ms, a flip angle of 50°, and a bandwidth of 250 Hz/Pixel. Overall, four measurements with the different RF increments of [0°, 90°, 180°, 270°] were performed, leading to a total acquisition time of 8 minutes. The four phase-cycled bSSFP scans were combined using a sum-of-squares (SOS) reconstruction. Visualization, semi-automated segmentation, and volumetric rendering of the endodontic roots was performed using ITK-SNAP7.
Results
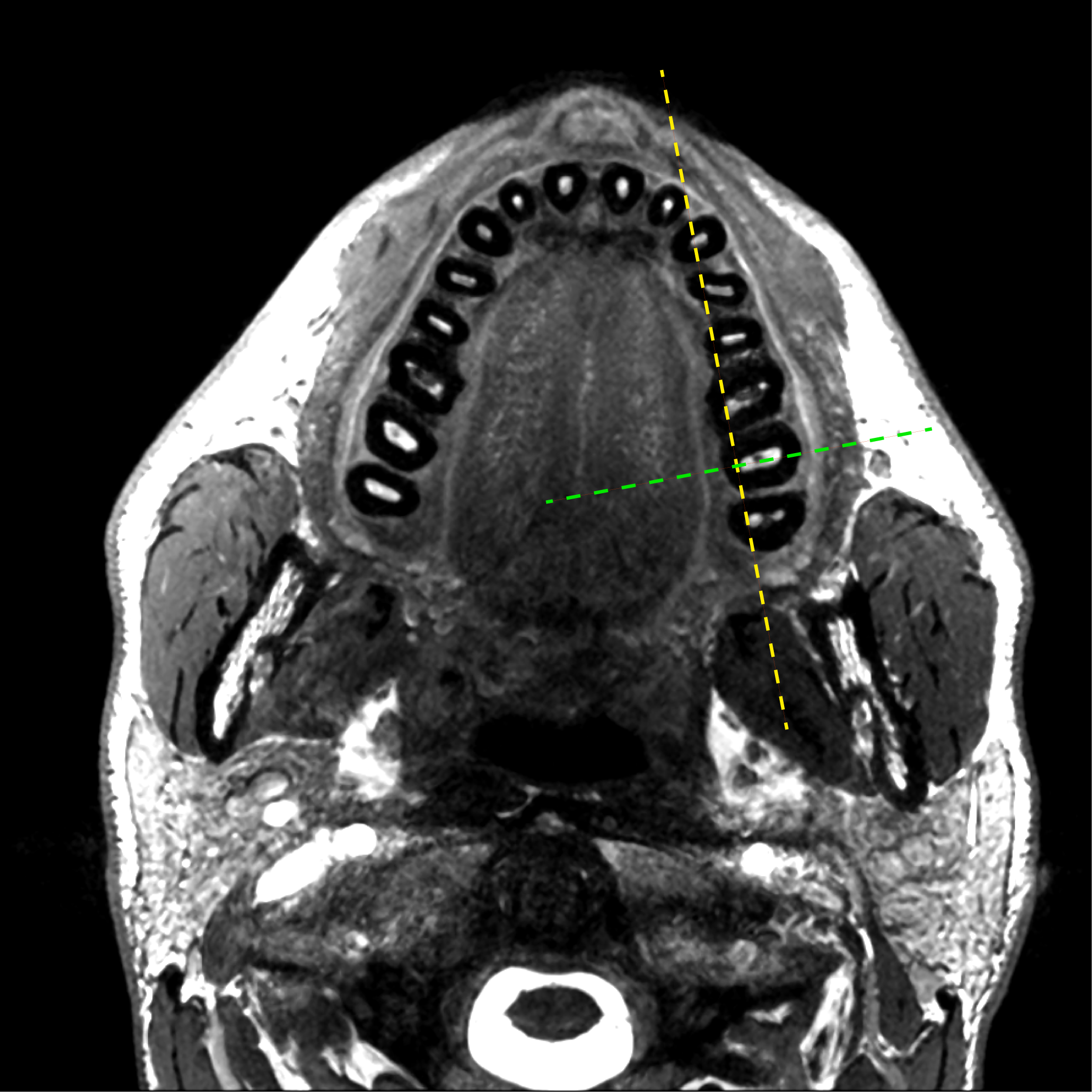
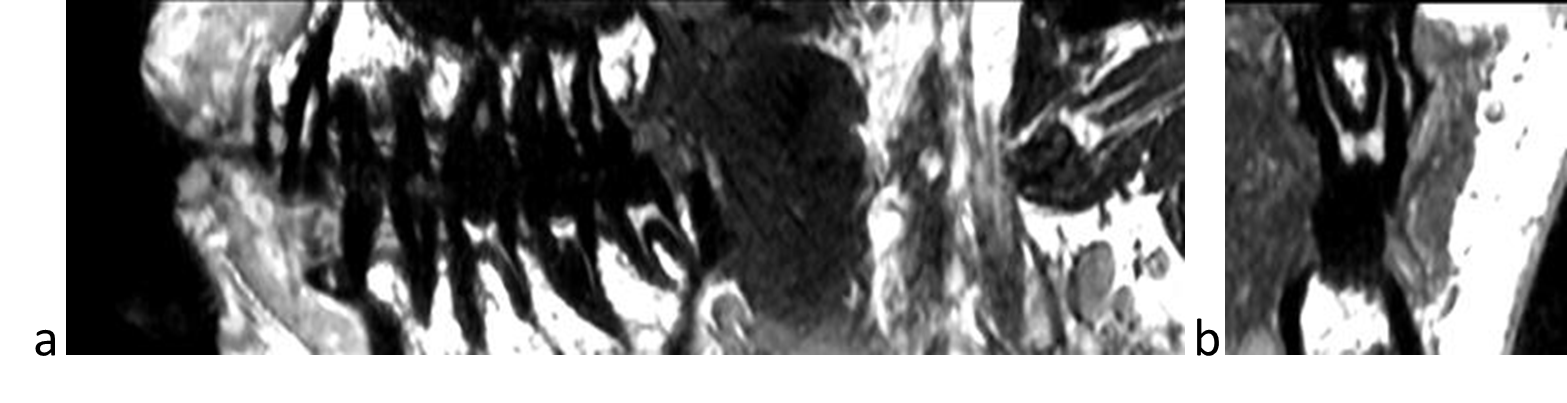
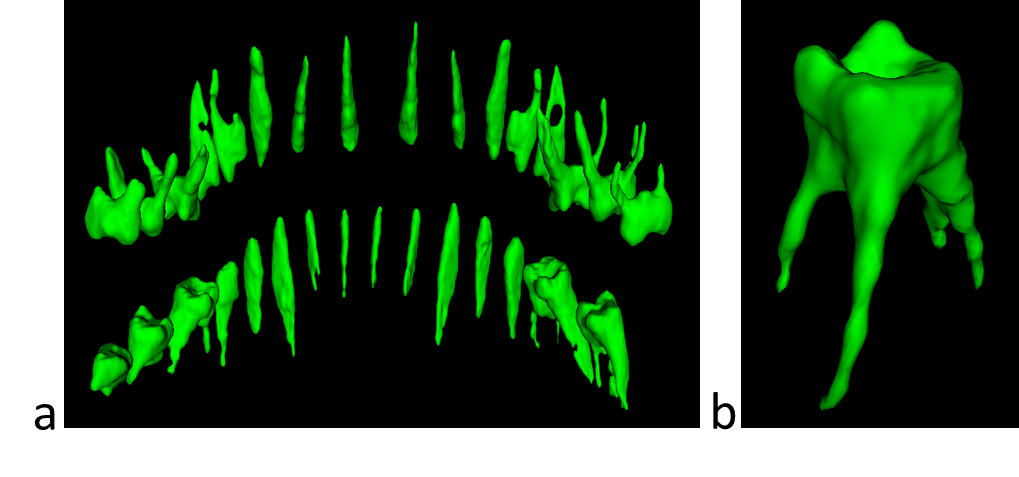
No co-registration of the four individual bSSFP scans was required prior to the SOS reconstruction. Exemplary axial, sagittal, and coronal slices acquiered with SOS bSSFP are shown in Figure 1. The dental pulp in the root canal reveals a strong signal with bSSFP and can be traced down to the single voxel level due to the surrounding dentine; exhibiting no signal. As can be seen in an para-sagittal and para-coronal reconstruction of the volumetric dataset (Fig. 2), the branches of the dental nerves are clearly resolved and delineated. A volumetric rendering of the segmented endodontic root canals of the upper and lower jaws is shown in Figure 3, revealing artefact-free, rich and high-resolution.Discussion and Conclusion
Endodontic imaging was performed in vivo using standard MRI equipment. Balanced SSFP is able to capture the signal of the soft pulp tissue with high signal-to-noise offering resolutions down to about 400µm. Off-resonance related banding artifacts were removed using multiple phase-cycled bSSFP acquisitions. Since SNR, however, does not seem to be a limiting factor in the current setup, a compressed sensing approach, such as the recently proposed trueCISS method8, will be explored to considerably shorten the overall acquisition time to about 4 minutes.
In conclusion, fast, high-resolution endodontic MRI is feasible with balanced SSFP down to voxel sizes of about 400µm using standard MRI equipment. This may represent an interesting and valuable approach in combination with an intraoral surface scan for the planning and guidance of the bur to the root canal orifice.
Acknowledgements
We would like to thank Nguyen Damien for his great help and patience. This work was funded by the Freiwillige Akademische Gesellschaft Basel and the Center of Dental Traumatology Basel.References
- Andreasen FM, Zhijie Y, Thomsen BL, Andersen PK. Occurrence of pulp canal obliteration after luxation injuries in the permanent dentition. Endod Dent Traumatol 1987;3(3):103-115.
- Oginni AO, Adekoya-Sofowora CA, Kolawole KA. Evaluation of radiographs, clinical signs and symptoms associated with pulp canal obliteration: an aid to treatment decision. Dental traumatology : official publication of International Association for Dental Traumatology 2009;25(6):620-625.
- Cvek M, Granath L, Lundberg M. Failures and healing in endodontically treated non-vital anterior teeth with posttraumatically reduced pulpal lumen. Acta odontologica Scandinavica 1982;40(4):223-228.
- Connert T, Zehnder MS, Amato M, Weiger R, Kuhl S, Krastl G. Microguided Endodontics: a method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. International endodontic journal 2017.
- Zehnder MS, Connert T, Weiger R, Krastl G, Kuhl S. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. International endodontic journal 2016;49(10):966-972.
- Dula K, Bornstein MM, Buser D, Dagassan-Berndt D, Ettlin DA, Filippi A, et al. SADMFR guidelines for the use of Cone-Beam Computed Tomography/ Digital Volume Tomography. Swiss dental journal 2014;124(11):1169-1183.
- Paul A. Yushkevich, Joseph Piven, Heather Cody Hazlett, Rachel Gimpel Smith, Sean Ho, James C. Gee, and Guido Gerig. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006 Jul 1; 31(3):1116-28.
- Hilbert T, Nguyen D, Thiran JP, Krueger G, Kober T, Bieri O. True constructive interference in the steady state (trueCISS). Magn Reson Med. 2017 Jul 24. doi: 10.1002/mrm.26836
Figures