4184
Variation in RF shimming SAR with patient position for 3 T breast imaging1GE Healthcare, Waukesha, WI, United States
Synopsis
This work investigates the variation in peak spatial SAR for RF shimming for different patient positions in the MR scanner for breast imaging. SAR simulations were performed on the Ella human body model in a 3 T 70 cm-diameter RF birdcage coil. Whole body SAR, peak spatial SAR, and SAR ratio (= peak SAR / whole body SAR) were computed for different patient elevations above the table (i.e., the patient lying on top of a breast coil). Patient position has important implications for setting safe RF shimming ranges due to the variations in peak spatial SAR in different patient positions.
Introduction
One significant safety concern of MR imaging is radio-frequency (RF) induced tissue heating. This effect has been widely investigated for various body models, positions in the coils, and anatomies [1-3]. The work presented here expands on this research by investigating the variation in peak spatial SAR for RF shimming for different patient positions in the MR scanner. Specifically, the case of breast imaging (patient is prone and elevated from the patient table to accommodate the breast coil) is investigated because in this particular case, the patient is typically closer to the whole body transmit RF coil than in other positions, such that peak spatial SAR can become more of a safety concern.Methods
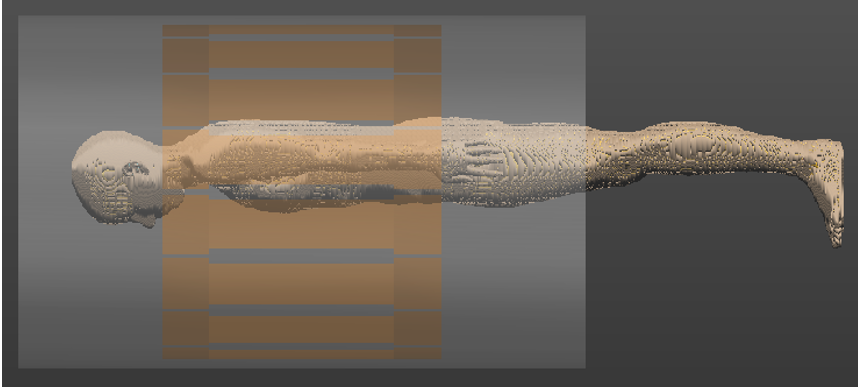
Simulations were performed using SEMCAD X v14.8.6 (SPEAG). The Ella human body model from the Virtual Family [4] (59.6 kg female) was positioned in a prone position in a representative 70 cm-diameter, 16-rung, 3 T body coil in a breast landmark. The model was elevated from the patient table by varying amounts (8-12 cm) in order to simulate the patient position for breast imaging (patient is positioned on top of the breast coil), as shown in Figure 1.
The body coil was excited at 128 MHz using unit voltage source excitations. The resultant electric and magnetic fields in the body for each channel were exported using a uniform (2 mm)^3 grid. The data was post-processed using MATLAB (Mathworks). Whole body SAR, peak spatial SAR, and SAR ratio (= peak SAR / whole body SAR) were computed for quadrature excitation as well as the full RF-shimming space of amplitude and phase offsets between the two RF body channels. The amplitude offsets of channel 2 relative to channel 1 were in the range [-1 5.5] dB, while the phase offsets of channel 2 relative to channel 1 were in the range [-70 10] degrees. The SAR values were scaled to an average B1rms of 1 μT in the central axial (x-y) slice of the body. Peak SAR was computed by averaging over a volume of 10x10x10 voxels.
Results
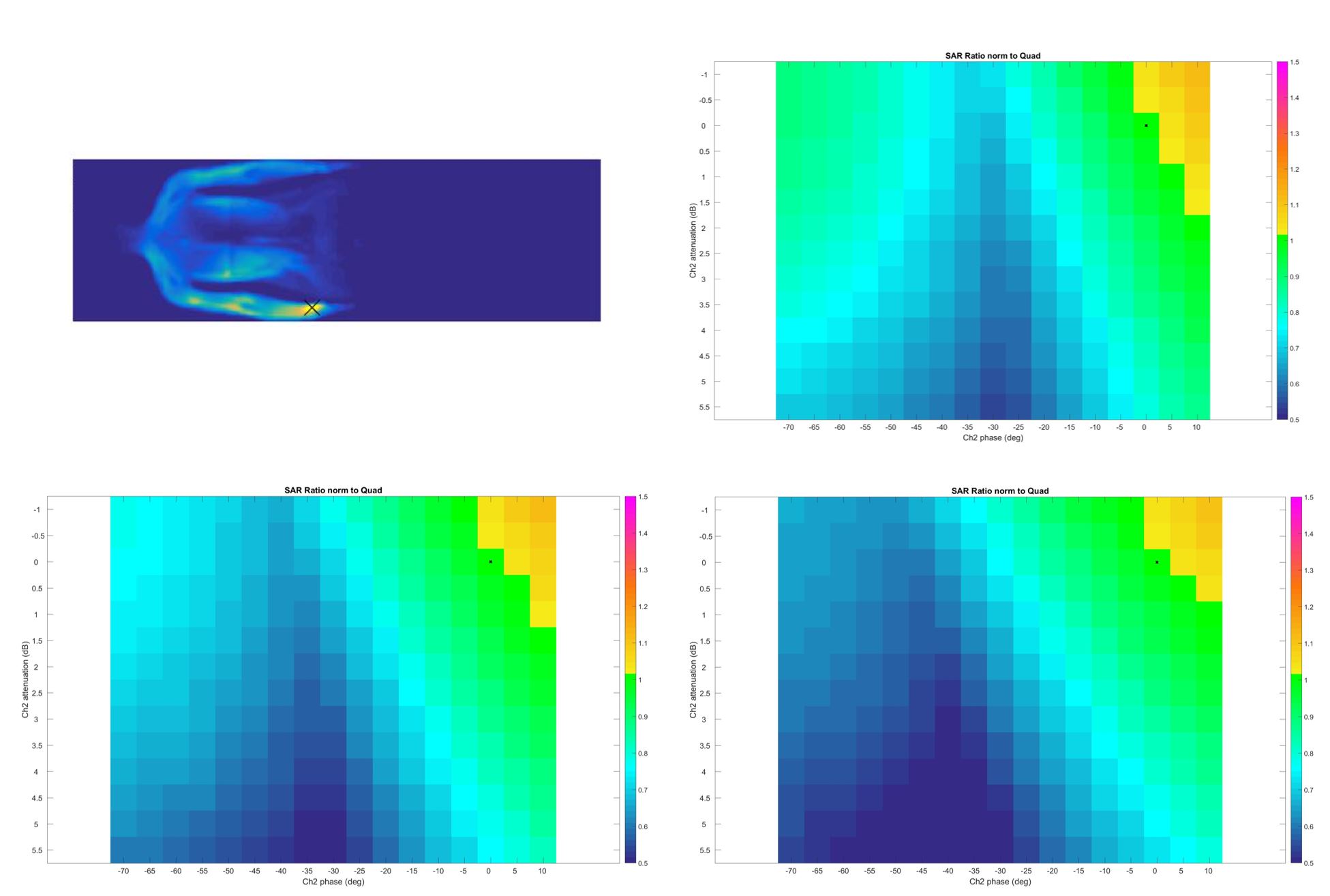
Figure 2 shows the coronal cross-sectional slice for the SAR distributions at the location of the maximum peak spatial SAR for the 8 cm elevation, as well as the SAR ratio (normalized to the SAR ratio at quadrature) for the Ella body model at three different elevations above the patient table. The color scale in all three images is the same: [-0.5 1.5]; green and blue indicate normalized SAR ratio <= 1, while yellow and red indicate normalized SAR ratio > 1. It is implied that SAR ratio <= 1 is safe because it is less than the SAR ratio at quadrature.
The location of maximum peak SAR is in the wrist for all cases. The SAR distributions for the other elevations are very similar. In all cases, the whole body SAR is approximately the same. The peak local SAR is 4.14 W/kg at 8 cm, 4.35 W/kg at 10 cm, and 4.71 W/kg at 12 cm (an increase of ~15%). Accordingly, the SAR ratio (normalized to the SAR ratio at quadrature) is also different for the three different positions, as shown in Table 1 below.
Discussion and conclusion
Safe ranges for RF shimming are often set by comparing the whole body and peak spatial SAR at a specific excitation to the SAR at quadrature. This abstract shows that patient position has important implications for evaluating and setting these RF shimming ranges. For example, the safe range for the 12 cm elevation appears to be larger (larger offsets in amplitude and phase of the two excitation channels) than for 8 cm. Often a larger RF shim range may be advantageous to obtain the best image quality for a particular imaging application. Therefore, it is important to consider a variety of patient positions when performing simulations for setting an appropriate RF shim range that properly balances image quality and patient safety.Acknowledgements
The author would like to thank M. Eash and A. Vu at GE Healthcare for helpful discussions.References
[1] Lazebnik, ISMRM (2016). [2] Wolf S, et al, MRM 69:1157-1168 (2013). [3] Murbach M, et al, MRM 71:839–845 (2014). [4] Christ A., et al, PMB, 55(2):N23-N38, (2010).Figures