4162
Real-Time Golden Angle Radial iSSFP: Impact of the Gradient Spoiler Direction on Motion and Flow Effects1Radiological Sciences, University of California, Los Angeles, Los Angeles, CA, United States, 2Physics and Biology in Medicine, University of California, Los Angeles, Los Angeles, CA, United States, 3MR R&D Collaborations, Siemens Healthineers, Los Angeles, CA, United States, 4Bioengineering, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Real-time visualization is crucial to the success of MRI-guided minimally invasive cancer interventions. We have developed golden-angle (GA) ordered radial integrated-SSFP (iSSFP), which can suppress banding artifacts associated with bSSFP while maintaining similar contrast. However, the addition of the gradient spoiler in iSSFP removes the flow and motion compensation along the axis of the gradient. In this work, we analyze pelvic and abdominal iSSFP scans acquired in the axial, sagittal and coronal planes to investigate the effects of having the gradient along different directions with respect to motion/flow. GA radial iSSFP can potentially improve tissue contrast for real-time MRI-guided interventions, after careful consideration for the imaging plane, gradient spoiler direction, and motion/flow direction.
Introduction
Real-time visualization is crucial to the success of MRI-guided minimally invasive cancer interventions, especially in the abdomen. The sequence must be ultrafast, with high soft-tissue contrast. Balanced steady-state free-precession (bSSFP) has good contrast, but suffers from banding artifacts(1). Previously, we have developed golden-angle (GA) ordered radial integrated-SSFP (iSSFP)(2), which suppresses banding artifacts associated with bSSFP while maintaining similar contrast. However, the addition of the iSSFP gradient spoiler removes the flow and motion compensation along the gradient’s axis. In this work, we investigated the motion and flow effects of GA radial iSSFP with the gradient placed along different directions/axes.Methods
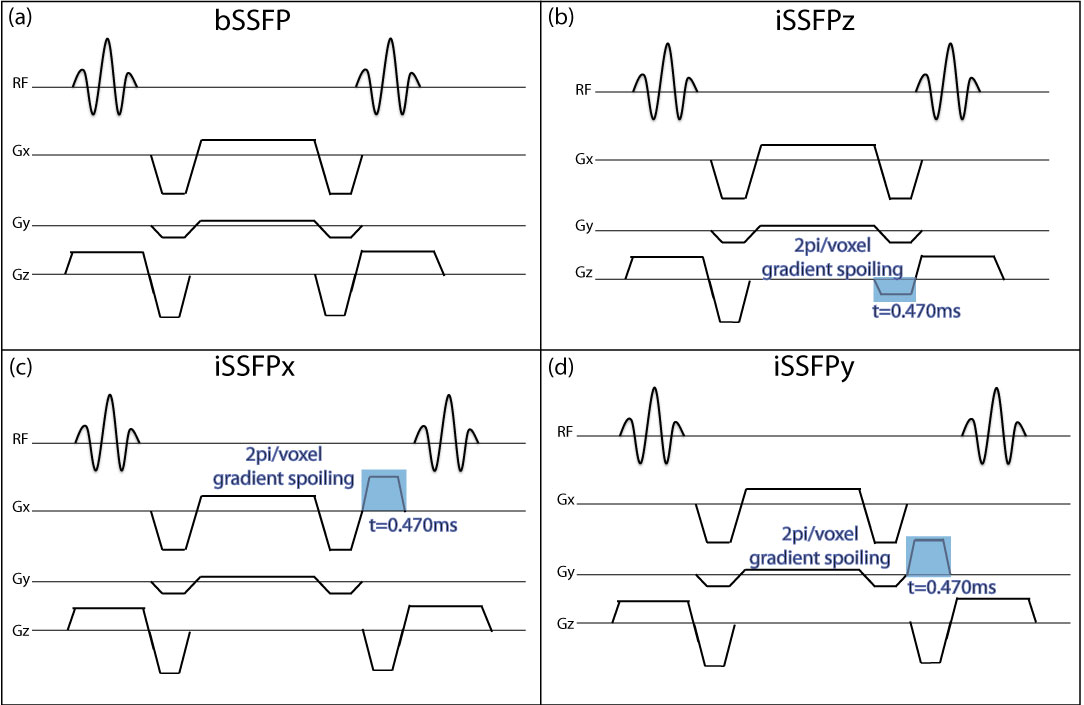
Real-time Golden-Angle Radial iSSFP: The GA radial iSSFP sequence was designed with a gradient spoiler to achieve 2π/voxel dephasing(3) in the logical Z (iSSFPz), X (iSSFPx) or Y (iSSFPy) direction (Fig. 1). Due to the angular rotation of the radial trajectory in the kx-ky plane, the iSSFPx (iSSFPy) gradient was added after the readout dephaser, to achieve consistent gradient spoiling along the logical X (Y) direction for all readouts. Since the logical Z (slice select) direction is not affected by the rotation, the gradient was combined with the slice select dephasing gradient. The radial readouts were continuously acquired with GA ordering(4) and reconstructed using a sliding-window SPIRiT(5) algorithm.
Tissue Contrast Evaluation Experiments: With IRB approval, n=3 healthy subjects underwent pelvic and abdominal (breath-held) MRI at 3T (Skyra, Siemens) using the GA radial bSSFP, iSSFPx, iSSFPy, and iSSFPz sequences (FOV: 400x400mm2, resolution: 2x2x3mm3, TE/TR: 2.2/4.4ms, FA: 50o). All radial imaging was fully sampled (400 spokes, 4.4 sec) and acquired in the axial, sagittal and coronal planes to investigate the effects of the gradient along different directions with respect to motion/flow.
Free-Breathing Real-Time Experiments: To characterize in vivo real-time imaging performance, healthy subjects (n=2) underwent abdominal scans during free-breathing (FB) using the above four sequences for the three orthogonal imaging planes. The sequences were acquired with increased radial readouts (1000 spokes, 11 sec) to be reconstructed into dynamic series (temporal resolution: 44ms, temporal footprint: 633.6ms).
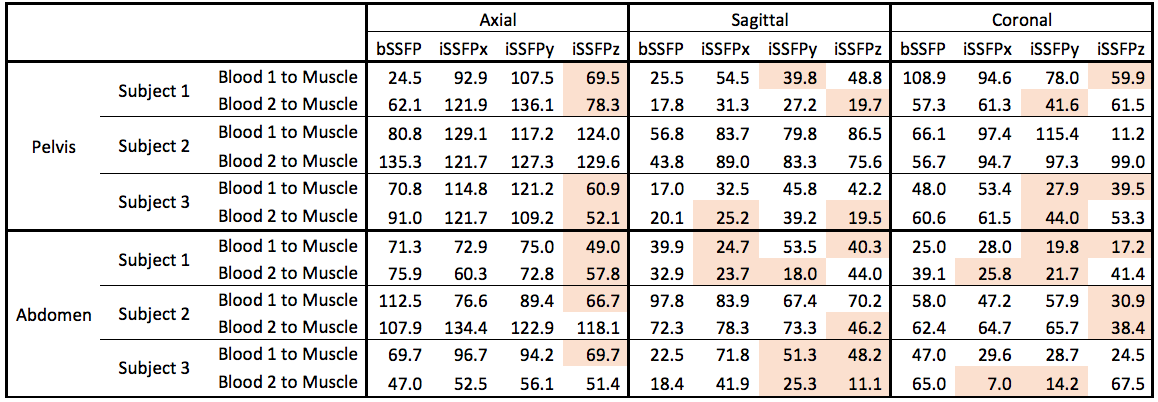
Image Analysis: The CNR of the two branches of the iliac artery (pelvis) and the hepatic and portal veins (abdomen) with respect to muscle were computed and compared across all three imaging planes for all three gradient directions. The images were visually inspected for artifacts and image quality, especially in the areas of blood flow. The FB images were inspected for motion and flow artifacts. The variations in signal magnitude of a vessel were inspected by plotting a profile over time.
Results
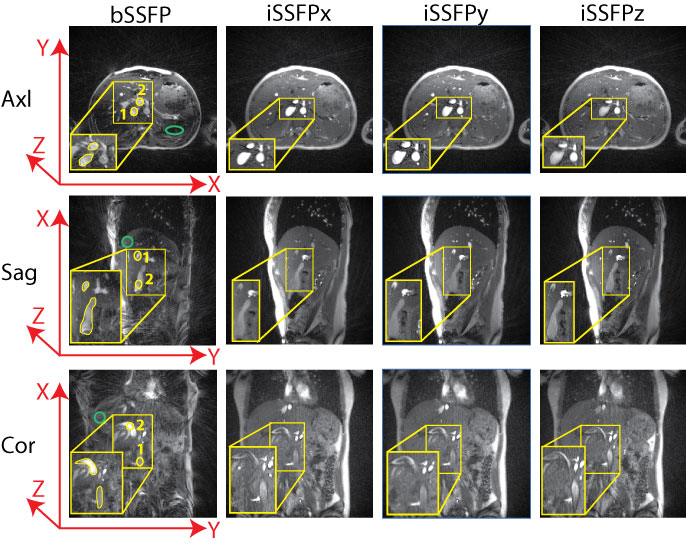
Tissue Contrast: The iSSFP sequences eliminated banding artifacts in the pelvis and abdomen (Fig. 2, 3). In the axial views of both the pelvis and abdominal acquisitions, there was a substantial CNRblood,muscle reduction (Table 1) in only the iSSFPz direction due to the through-plane blood flow. For the sagittal and coronal views, the CNRblood,muscle reduction depended on the orientation of the vessel.
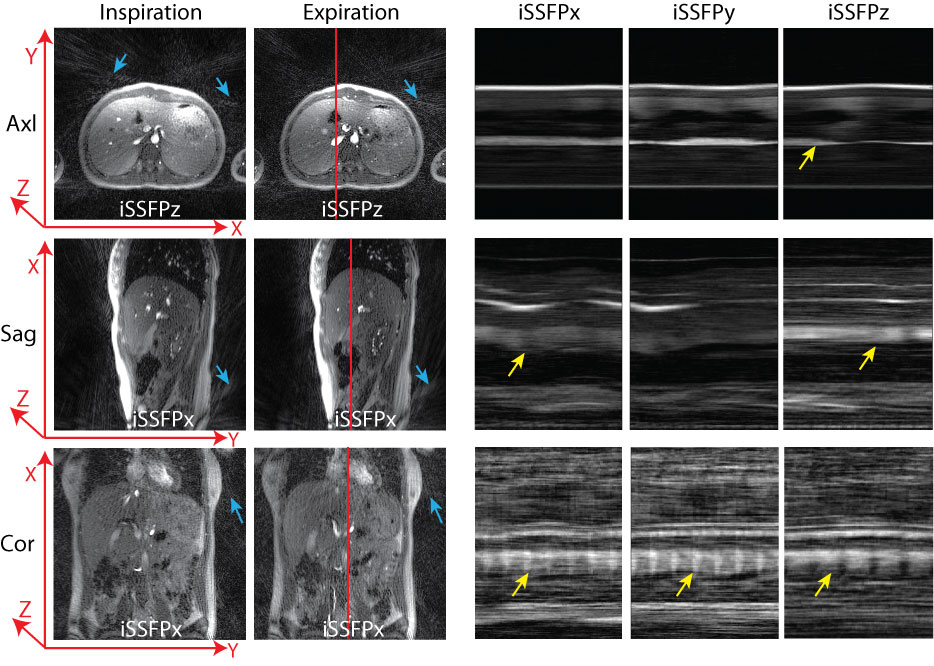
Free-Breathing Real-Time Evaluation: Frames of the FB abdominal scans were chosen to compare motion artifacts (Fig 4). The profile-over-time plots show if the gradient is along the flow direction in a vessel, the contrast fluctuates accordingly. However, if the gradient direction is orthogonal to the flow, the vessel contrast stays more constant (Fig 4). The motion artifacts can be visualized by increased streaking artifacts. The degree of the motion artifacts was higher when the motion was along the gradient direction in almost all cases.
Discussion
GA radial iSSFP achieves the tissue contrast benefits of bSSFP without the banding artifacts consistently for all gradient spoiler directions. The direction of the iSSFP gradient has a considerable impact on the flow and motion effects in the image. When the gradient is along the axis/direction of flow/motion, (i.e. axial slice with iSSFPz) there is a CNRblood,muscle reduction. Although bSSFP has inherent motion compensation, banding artifacts reduce the CNRblood,muscle.
The gradient direction versus blood signal relationship is more complex in the sagittal and coronal planes due to vessel orientation. Vessels are rarely along a single axis, thus the flow component reduces the contrast for multiple gradient directions. Also, the temporal rate of the flow through a vessel affects the CNR reduction. Larger vessels have a higher flow rate, increasing flow effects. During interventional procedures, a steady signal is desired to achieve consistent visualization of vascular landmarks for guidance and safety. Ideally, the direction of the iSSFP spoiling gradient should be orthogonal to the orientation of major vessels or motion to improve image quality.
Conclusion
This study shows that iSSFP can potentially improve tissue contrast for real-time MRI-guided interventions, provided the axis/direction in which the spoiling gradient is placed is chosen in careful consideration with respect to the imaging plane and flow/motion direction.Acknowledgements
No acknowledgement found.References
1. Hargreaves BA. Rapid gradient-echo imaging. J. Magn. Reson. Imaging 2012;36(6):1300-13. doi:10.1002/jmri.23742.
2. Mikaiel S, Martin T, Sung K, Wu HH. Quantitative Image Analysis of Real-Time Golden Angle Radial iSSFP for Interventional MRI. In: ISMRM 25th Annual Meeting.; 2017:5556. doi:10.1002/jmri.23742.2.
3. Martin T, Wang Y, Moeller S, Sung K, Wang DJ. Accelerated Multiband SSFP Imaging with Controlled Aliasing in Parallel Imaging and integrated-SSFP (CAIPI-iSSFP). Investig. Magn. Reson. Imaging 2017;21(4).
4. Winkelmann S, Schaeffter T, Koehler T, Eggers H, Doessel O. An optimal radial profile order based on the Golden Ratio for time-resolved MRI. IEEE Trans. Med. Imaging 2007;26(1):68-76. doi:10.1109/TMI.2006.885337.
5. Lustig M, Pauly JM. SPIRiT: Iterative self-consistent parallel imaging reconstruction from arbitrary k-space. Magn. Reson. Med. 2010;64(2):457-71. doi:10.1002/mrm.22428.
Figures