4161
Application of SSFSE T1-weighted imaging for MRI-guided bone biopsy1Memorial Sloan Kettering Cancer Center, New York, NY, United States, 2GE Healthcare, New York, NY, United States
Synopsis
MRI guided biopsy plays an important role in the diagnosis of bone lesions. Although T1w FSE offers exceptional signal-to-noise ratio and resolution, its acquisition time is relatively long. In this study, we evaluate a single-shot FSE with centric partial Fourier encoding, variable refocusing flip angle, and an inversion recovery preparation pulse (vrfSSFSE-IR) for MRI-guided bone biopsy application with the goal to reduce the overall procedure time.
Introduction
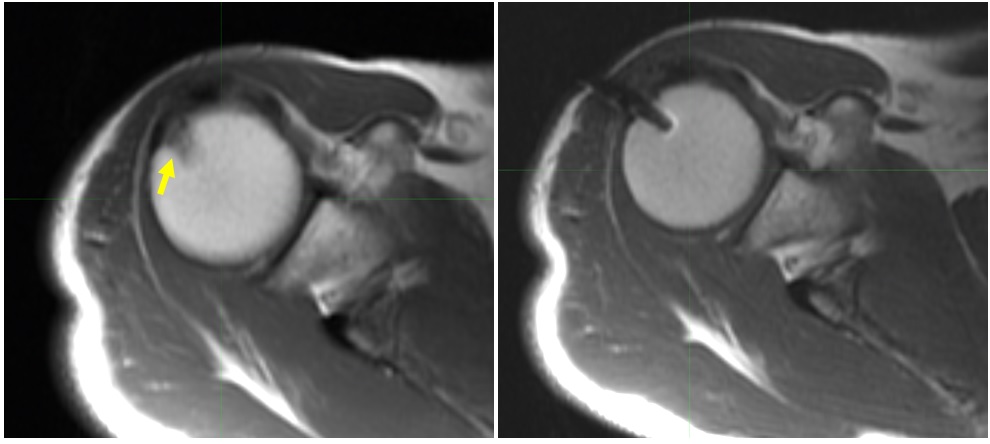
Magnetic resonance imaging (MRI) guided biopsy plays an important role in the diagnosis of bone lesions1-3. Despite excellent MRI visualization of bone tumors and lack of ionizing radiation, the majority of current procedures are carried out under the guidance of computerized tomography4 owing to the superior quality of the biopsy instrument and speed of this imaging modality. The large size of the currently available MR-compatible titanium biopsy needles (3-4 mm diameter) results in substantial image artifacts thus rendering gradient echo-based sequences unsuitable for this procedure. T1-weighted fast spin-echo (FSE) sequence, on the other hand, helps minimize the susceptibility artifact around the needle while still visualizing the bone lesions (Figure 1). Although T1w FSE offers exceptional signal-to-noise ratio and resolution, its acquisition time is relatively long. Hence, when repeated multiple times to guide the placement of the biopsy needle, it substantially impacts the duration of the procedure. On the other hand, single-shot FSE with centric partial Fourier encoding, variable refocusing flip angle, and an inversion recovery preparation pulse (vrfSSFSE-IR)5 can produce T1-like contrast while keeping acquisition time very short. The goal of this work was to evaluate the vrfSSFSE-IR pulse sequence for MRI-guided bone biopsy application.Methods
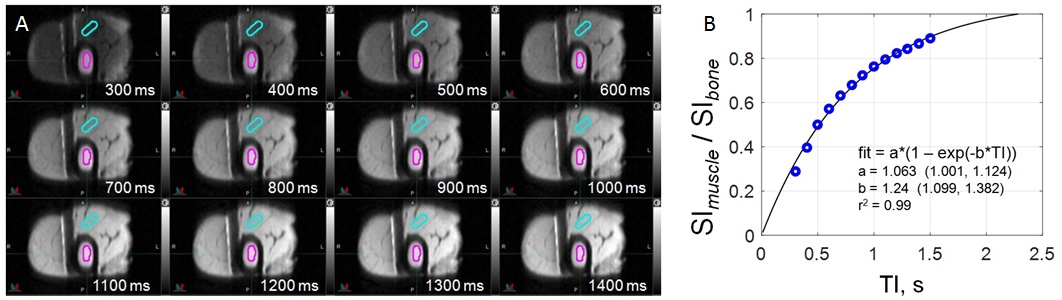
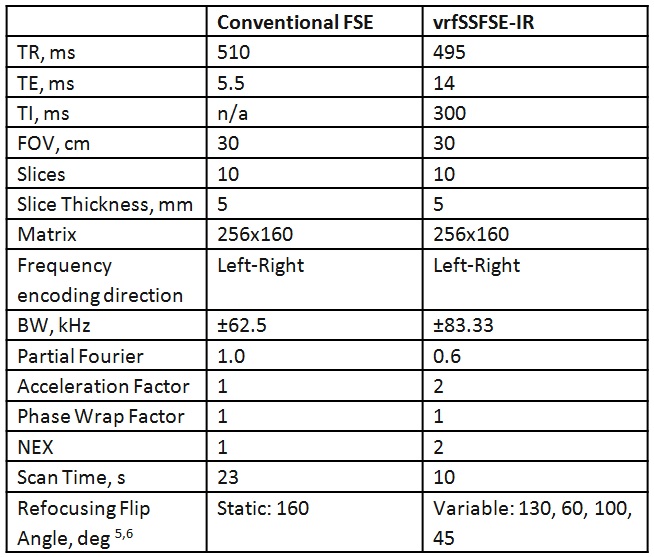
We evaluated the vrfSSFSE-IR sequence on a 1.5T MRI scanner (Discovery MR450w, GE Healthcare, Waukesha, WI) using an 8-channel head coil. An ex vivo bovine bone-muscle tissue sample with a 4-mm titanium bone biopsy needle (Invivo, FL, USA) was first scanned with a conventional FSE sequence from our clinical bone biopsy protocol and then with the vrfSSFSE-IR sequence. The vrfSSFSE-IR sequence was repeated for inversion time (TI) ranging from 300 to 1500 ms. Regions of interest were placed in muscle and bone marrow tissue on both conventional FSE and vrfSSFSE-IR images to calculate the average signal intensity (SI) (Figure 2A). The ratio of muscle to bone marrow average SI obtained from all images was analyzed, and the TI value producing the SI muscle to bone marrow ratio equivalent to that measured on the FSE image was determined. The scan time as a function of number of slices was also evaluated for a fixed set of parameters (Table 1). The appearance of the biopsy needle artifact was also evaluated.Results
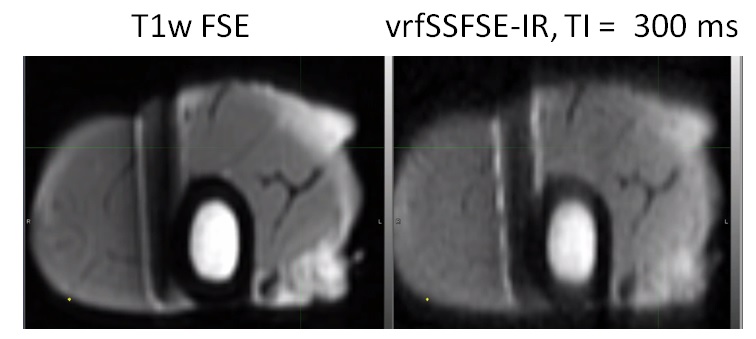
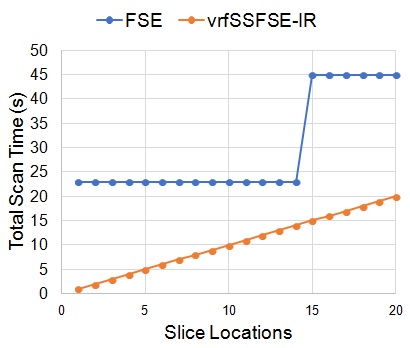
Figure 2A shows the images obtained with the vrfSSFSE-IR sequence for a TI of 300 to 1400 ms. An exponential function of the form SImuscle/SIbone = a*(1 – exp(-b*TI) was found to describe the relationship between the muscle to bone marrow SI ratio and the TI with 0.99 correlation coefficient of the fit (Figure 2B). The value varied from 0.29 to 0.89. The SI ratio measured in the FSE image was 0.35. Based on the exponential fit obtained above it was found that a TI of 318 ms would produce a FSE-equivalent muscle to bone marrow SI ratio using the vrfSSFSE. Figure 3 shows the comparable muscle to bone marrow contrast in conventional FSE and vrfSSFSE-IR with TI of 300 ms. The susceptibility artifact caused by the biopsy needle is comparable between the two sequences, with the needle appearing narrower in the SSFSE image due to the slightly higher bandwidth (Table 1). The total scan time, as a function of the number of slices, is shown in Figure 4.Discussion
The results of this study demonstrate that T1-like contrast in muscle to bone marrow tissue can be achieved using the vrfSSFSE-IR sequence at a shorter acquisition time while keeping the biopsy needle artifact comparable. Depending on the conspicuity and size of the bone lesion being targeted, the lower signal-to-noise ratio and the blurring that is inherent to the SSFSE sequences may be a limitation. However, even in that scenario, vrfSSFSE-IR may be useful to guide placement of the needle after the conventional FSE image is acquired for target visualization. The linear relationship between the scan time and number of slices is especially valuable in an interventional setting where only a very limited region needs to be imaged repeatedly in order to depict the progress of the needle placement. Using vrfSSFSE-IR to image 6 slices, for example, there will be ~4 fold reduction in scan time compared to imaging with FSE.Conclusion
This preliminary evaluation shows that the vrfSSFSE-IR sequence may play a valuable role in reducing the overall procedure time of the MRI-guided bone biopsy. As part of future work, this sequence will be accessed in the bone biopsy procedures to establish its true clinical value.Acknowledgements
No acknowledgement found.References
1. König CW, TRüBENBACH J, Böhm P, Fritz J, Duda SH, Pereira PL. Magnetic resonance-guided transcortical biopsy of bone marrow lesions using a magnetic resonance imaging-compatible piezoelectric power drill: preliminary experience. Investigative radiology. 2003;38(3):159-63.
2. Neuerburg JM, Adam G, Buecker A, et al. MRI‐guided biopsy of bone in a hybrid system. Journal of Magnetic Resonance Imaging. 1998;8(1):85-90.
3. Parkkola R, Mattila K, Heikkilä J, et al. Dynamic contrast-enhanced MR imaging and MR-guided bone biopsy on a 0.23 T open imager. Skeletal radiology. 2001;30(11):620-4.
4. Leffler SG, Chew F. CT-guided percutaneous biopsy of sclerotic bone lesions: diagnostic yield and accuracy. AJR American journal of roentgenology. 1999;172(5):1389-92.
5. Litwiller DV, Taviani, V, Estkowski L, Bayram E. Fast, motion-robust T1-weighted body imaging with single-shot fast spin echo via centric partial Fourier encoding and variable refocusing flip angle. ISMRM; 2016; Singapore.
6. Busse RF, Hariharan H, Vu A, Brittain JH. Fast spin echo sequences with very long echo trains: design of variable refocusing flip angle schedules and generation of clinical T2 contrast. Magnetic resonance in medicine. 2006;55(5):1030-7.
Figures