4152
Simultaneous 3D Whole-Heart Bright-Blood Visualization of the Coronary Sinus and Heart Anatomy and Black-Blood PSIR Quantification of Atrial Wall Thickness for Non-Contrast Enhanced Interventional Planning1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Atrial wall thickness quantification has the potential of providing important clinical information when planning electrophysiological interventions. Imprecise delivery of thermal energy during catheter ablation can prevent the success of the procedure. Furthermore, pre-interventional knowledge of subject-specific variations in the anatomy of the coronary sinus (CS) is crucial for adequate catheterization. Here, we propose a free-breathing 3D whole-heart phase-sensitive inversion recovery sequence suitable for non-contrast enhanced interventional planning, offering simultaneous visualization of the atrial walls and CS anatomy. The sequence is integrated in a framework with image-based navigation and non-rigid respiratory motion correction for 100% scan efficiency and improved image sharpness.
Introduction
Atrial arrhythmia and atrial fibrillation are conventionally treated with catheter ablation procedures aiming at isolating areas with abnormal electrical activity. Insufficient or excessive thermal energy delivery during catheter ablation may lead to electrical reconnection of the ablated tissue or to thermal injury. Furthermore, complications may arise from improper insertion of the coronary sinus (CS) ablation catheter; this can involve accidental coronary arteries perforation as well as placement of the catheter in an incorrect route. Therefore, pre-interventional quantification of atrial wall thickness as well as knowledge of subject-specific variations in the anatomy of the CS and surrounding vessels have the potential of improving both the efficacy and the safety of catheter ablation procedures. In this study, we propose a 3D whole-heart phase sensitive inversion recovery (PSIR) sequence for simultaneous bright- and black-blood imaging that is suitable for non-contrast enhanced interventional planning. The proposed sequence provides 1) a 3D whole-heart bright-blood volume that is acquired exploiting magnetization transfer (MT) contrast (MTC) for improved visualization of the CS and veins1, and 2) an inherently co-registered black-blood volume allowing for the visualization and the segmentation of the atrial walls. The entire framework is integrated with image-based navigation2, enabling free-breathing data acquisition at 100% scan efficiency and predictable scan time. Furthermore, 3D non-rigid respiratory motion correction3 is exploited for improved image sharpness.Methods
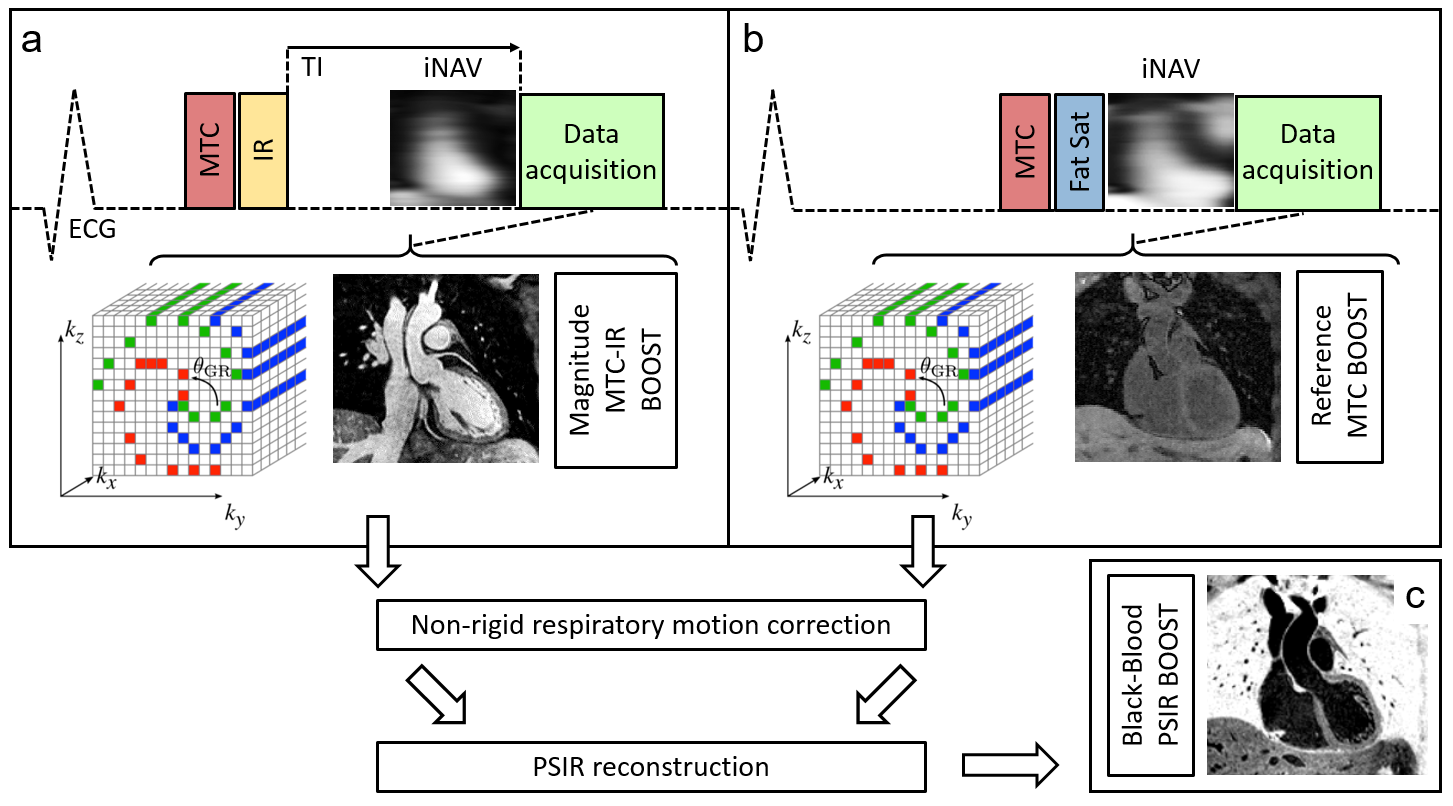
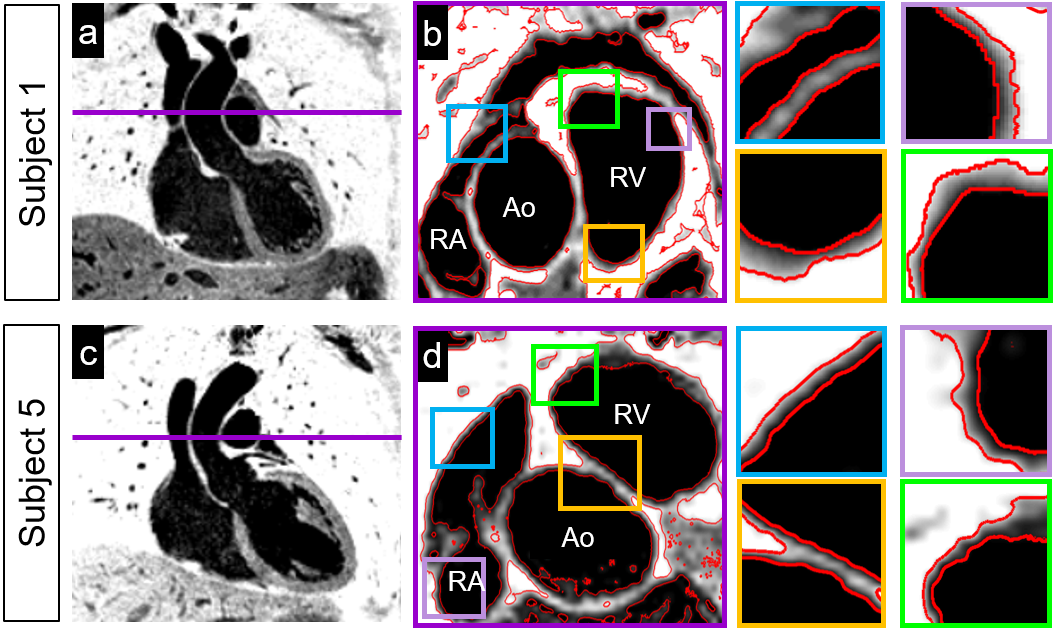
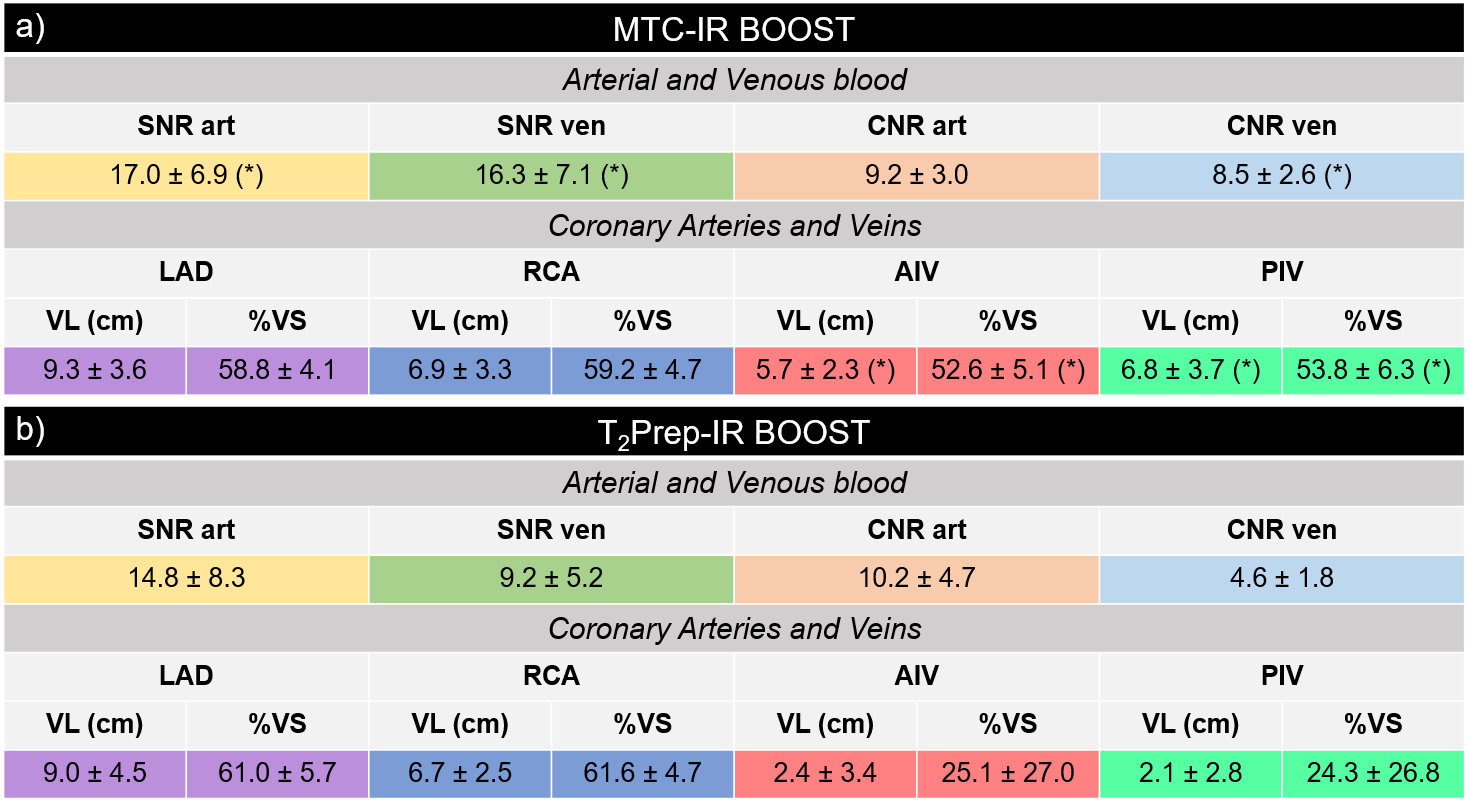
Framework: A 3D whole-heart bright-blood and black-blood PSIR (BOOST) bSSFP Cartesian prototype sequence with spiral profile order4 was implemented as shown in Fig1. Such sequence resembles that described in5, but utilizes MT preparation (instead of T2-preparation) for improved CS and coronary veins delineation1 and considers non-rigid motion correction (instead of translational motion correction only) for improved image sharpness. An MTC-IR module is applied in odd heartbeats (MTC-IR BOOST dataset), allowing for bright-blood visualization of cardiac anatomy, CS, coronary arteries and veins. MT preparation solely is applied in even heartbeats (MTC BOOST dataset). A low-resolution image navigator (iNAV) is acquired in each heartbeat. Data acquisition was performed in 7 healthy subjects on a 1.5T system (Siemens Magnetom Aera) using two different implementations of the BOOST sequence: 1) the implementation proposed in this study, exploiting MT preparation and illustrated in Fig1, and 2) the previously published implementation5, alternating the acquisition of a bright-blood T2-prepared IR volume (T2Prep-IR BOOST) and of a T2-prepared volume (T2Prep-BOOST). Imaging parameters for the proposed sequence included: isotropic resolution=1.4mm3, FOV=320x320x90-100mm, coronal orientation, TE/TR=1.56/3.6ms, flip-angle=90deg, TI=140ms. MT preparation consisted of 15 off-resonance Gaussian pulses (BWTP=1.92, flip-angle=800deg, duration=20.48ms, off-resonance frequency offset=3000Hz, pause between pulses=1.5ms). The counterpart sequence5, based on T2-preparation, was acquired with matching imaging parameters, T2-preparation duration=40ms, and TI=110ms. Image reconstruction: For both sequences, iNAVs acquired in odd and even heartbeats were used to estimate translational respiratory motion along the superior-inferior (SI) and right-left (RL) directions. Respiratory motion estimated along the SI direction was used to perform data binning (generating 4-6 bins per dataset). Bins were reconstructed with soft-gated iterative SENSE and non-rigid motion compensation was performed as previously proposed3. The motion corrected MTC-IR BOOST and MTC BOOST datasets were combined in a PSIR reconstruction6 to generate the complementary black-blood PSIR BOOST dataset for the visualization of the atrial walls. Data analysis: For both the bright-blood MTC-IR BOOST (obtained as shown in Fig1) and T2Prep-IR BOOST (obtained as described in 5) datasets, signal to noise ratio of arterial (SNRart) and venous (SNRven) blood, as well as contrast to noise ratio between arterial (CNRart) and venous (CNRven) blood with respect to myocardium were quantified. Furthermore, vessel length (VL) and percentage vessel sharpness (%VS) were computed for the right (RCA) and the left anterior descending (LAD) coronary arteries, and for the anterior (AIV) and posterior (PIV) interventricular veins7. Segmentation of the atrial walls in the black-blood PSIR BOOST datasets was performed using a machine learning based Trainable Weka Segmentation (TWS) algorithm8.Results
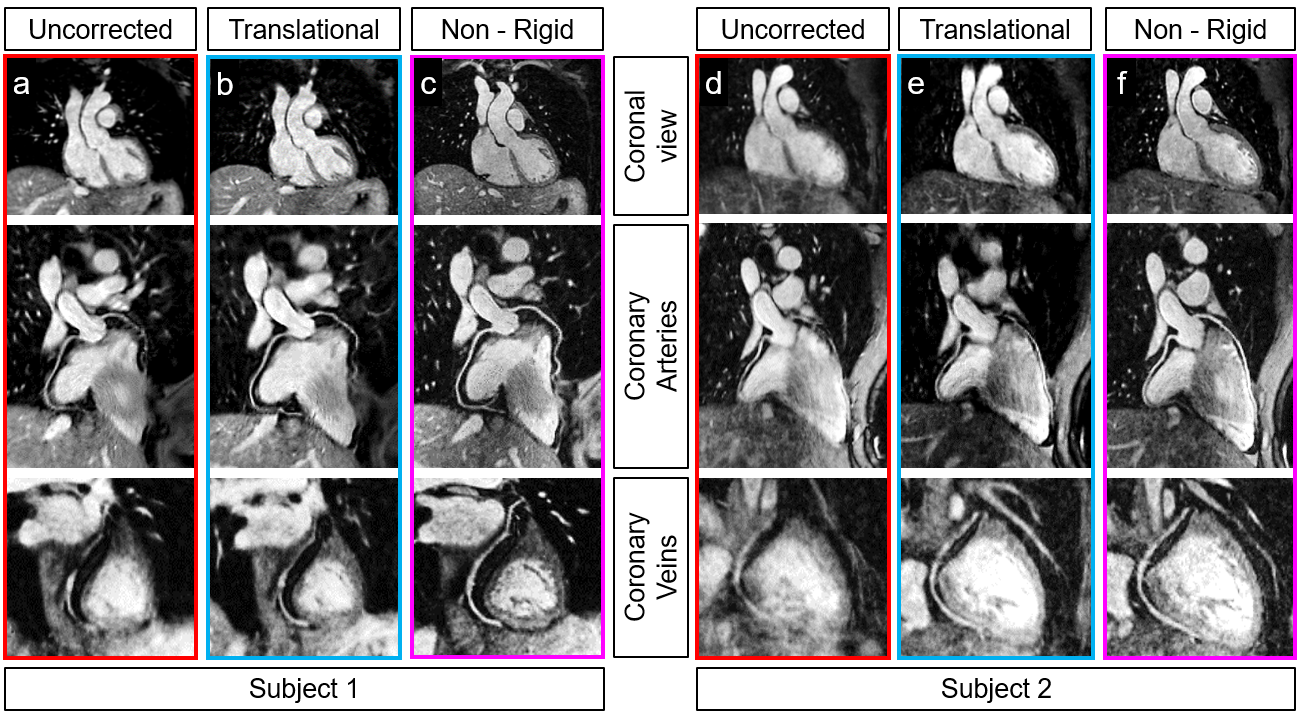
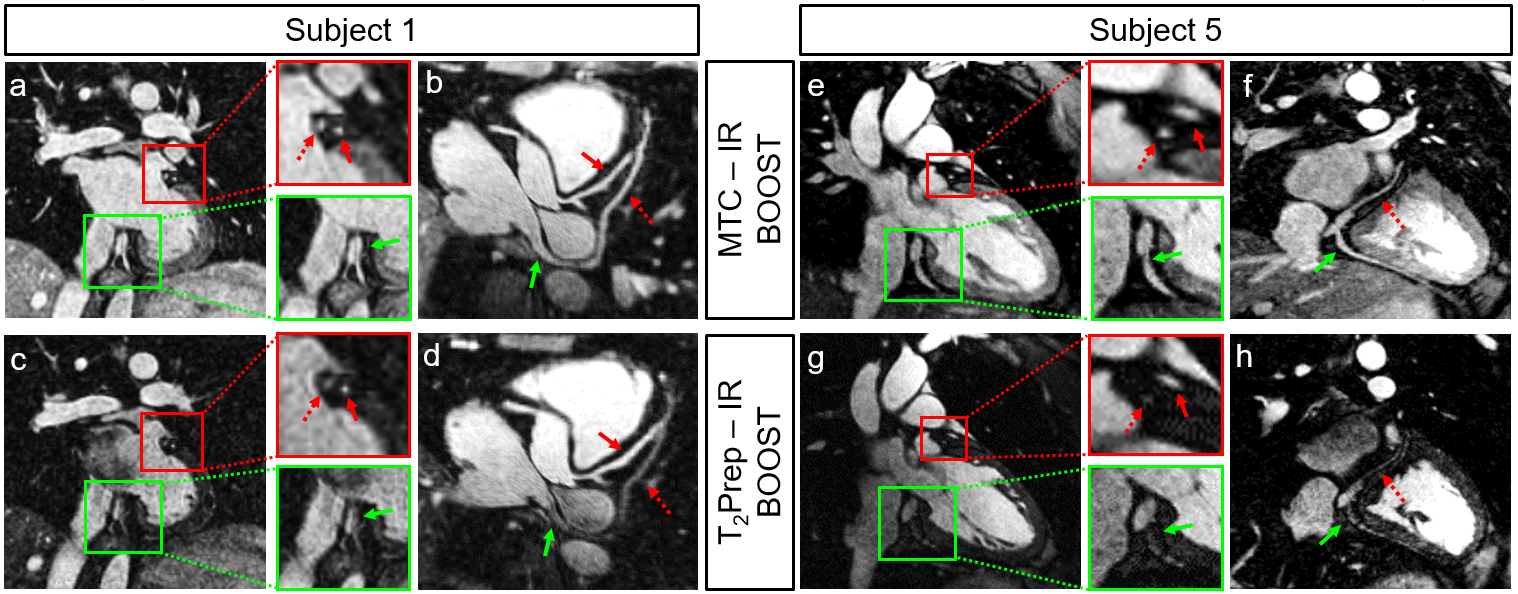
The use of non-rigid respiratory motion correction improved image quality when compared to translational motion correction only (Fig2). MTC-IR BOOST provided improved SNRven (comparable to SNRart), leading to improved visualization of the CS and coronary veins when compared to T2Prep-IR BOOST. Additionally, MTC-IR BOOST provided coronary artery delineation comparable to that of T2Prep-BOOST (Fig3). Quantitative endpoints are summarized in Table1. Atrial wall segmentation obtained with TWS is shown in Fig4.Conclusion
This study introduces a 3D whole-heart free-breathing sequence showing potential for non-contrast enhanced planning of electrophysiology procedures by providing inherently co-registered datasets for high-contrast bright-blood depiction of the heart and CS anatomy, coronary arteries and veins, together with black-blood visualization of atrial walls. Dedicated clinical studies are now warranted.Acknowledgements
This work was supported by the following grants: EPSRC EP/N009258/1, EP/P001009/1, EP/P007619/1, and FONDECYT 1161051.References
1. Nezafat R, Han Y, Peters DC, Herzka DA, Wylie JV, Goddu B, Kissinger KK, Yeon SB, Zimetbaum PJ, Manning WJ; Coronary magnetic resonance vein imaging: imaging contrast, sequence, and timing. Magn Reson Med. 2007 Dec; 58(6):1196-206.
2. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM; Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012 Feb; 67(2):437-45.
3. Cruz G, Atkinson D, Henningsson M, Botnar RM, Prieto C; Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017 May; 77(5):1894-1908.
4. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter T, Botnar RM; Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015 Mar; 41(3):738-46.
5. Ginami G, Neji R, Phinikaridou A, Whitaker J, Botnar RM, Prieto C; Simultaneous bright- and black-blood whole-heart MRI for noncontrast enhanced coronary lumen and thrombus visualization. Magn Reson Med. 2017 Jul 19. doi: 10.1002/mrm.26815.
6. Kellman P, Arai AE, McVeigh ER, Aletras AH; Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002 Feb; 47(2):372-83.
7. Etienne A, Botnar RM, Van Muiswinkel AM, Boesiger P, Manning WJ, Stuber M; “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002 Oct; 48(4):658-66.
8. Arganda-Carreas I, Kayning V, Rueden C, Eliceiri KW, Schindelin J, Cardona A, Sebastian Seung H; Trainable Weka Segmentation: a machine learning tool for microscopy pixel classification. Bioinformatics 2017 Aug 1; 33(15):2424-2426. doi: 10.1093/bioinformatics/btx180.
Figures