4122
Removal of Pseudo-lesion Artifact in Diffusion-Weighted Echo-Planar Imaging Using Virtual Coil Acquisition and Multiplexed Sensitivity Encoding (MUSE)1Department of Diagnostic Radiology, The University of Hong Kong, Hong Kong, Hong Kong, 2The State Key Laboratory of Brain and Cognitive Sciences, The University of Hong Kong, Hong Kong, Hong Kong
Synopsis
In routine brain DW-EPI with SENSE, the pseudo-lesion artifact due to residual aliasing of eyeball has been previously reported. We have found that the incidence of pseudo-lesion artifact was over 50% when performing double-oblique imaging on stroke patients. The possible cause is highly likely related to inference between residual Nyquist ghost and unfolding process in SENSE reconstruction. In this study, we propose a self-reference method to effectively remove pseudo-lesion artifact in double-oblique DW-EPI using virtual coil acquisition and multiplexed sensitivity encoding (MUSE). Our proposed method reveals higher image quality, better SNR performance, and lower artifact level than conventional SENSE reconstruction.
Introduction
Parallel imaging such as sensitivity encoding (SENSE) has been used to effectively reduce the geometric distortion in diffusion-weighted echo-planar imaging (DW-EPI)1. In routine brain DW-EPI with SENSE reconstruction, the occurrence of pseudo-lesion artifact due to residual aliasing of eyeball has been previously reported2. We have found that the incidence of pseudo-lesion artifact was over 50% when performing double-oblique imaging on stroke patients (from our results). We hypothesize that the residual Nyquist ghost after 1D phase correction interferes with unfolding process in SENSE reconstruction, resulting in residual aliasing artifacts that can cause pseudo-lesion in apparent diffusion coefficient (ADC) map. Thus, an effective method that can simultaneously remove Nyquist ghost and unfold the aliased pixels is highly desired for double-oblique accelerated DW-EPI acquisition. In this study, we first propose a self-reference method to effectively remove pseudo-lesion artifact in double-oblique DW-EPI using virtual coil acquisition3 and multiplexed sensitivity encoding (MUSE)4,5. Second, the proposed method is quantitatively evaluated in patients in terms of measured ADC values, signal-to-noise ratio (SNR), and artifact level.Methods
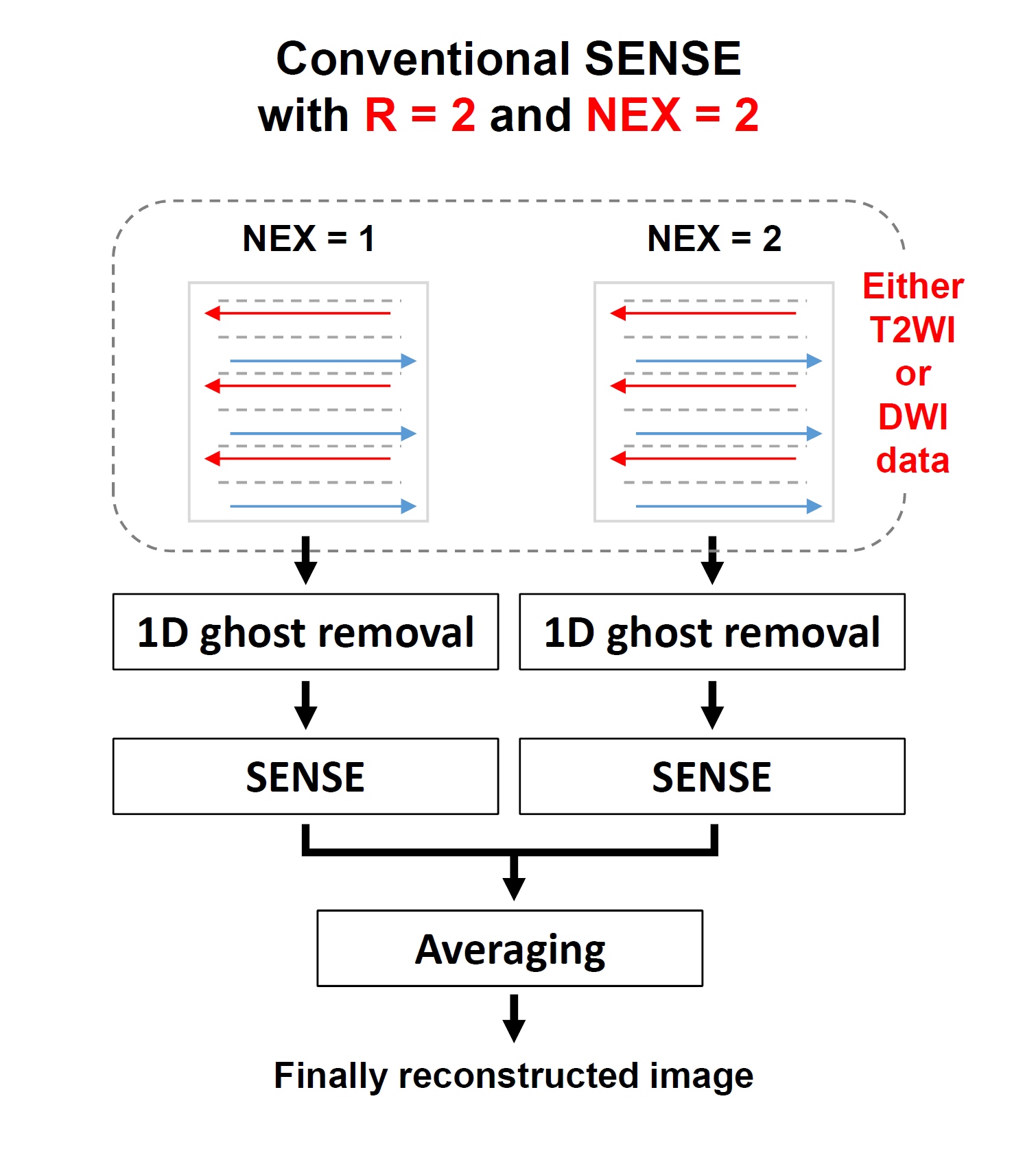
I. Conventional SENSE reconstruction: In routine DW-EPI with SENSE, multiple NEX (e.g., NEX of 2 has been used in our protocol) is always performed to compensate the undesired noise amplification due parallel imaging reconstruction. Figure 1 shows the reconstruction flowchart in clinical MRI scanner for DW-EPI data acquired with acceleration factor R=2 and NEX=2. The data of each NEX acquisition is reconstructed respectively, and then subsequently averaged together to generate a final image.
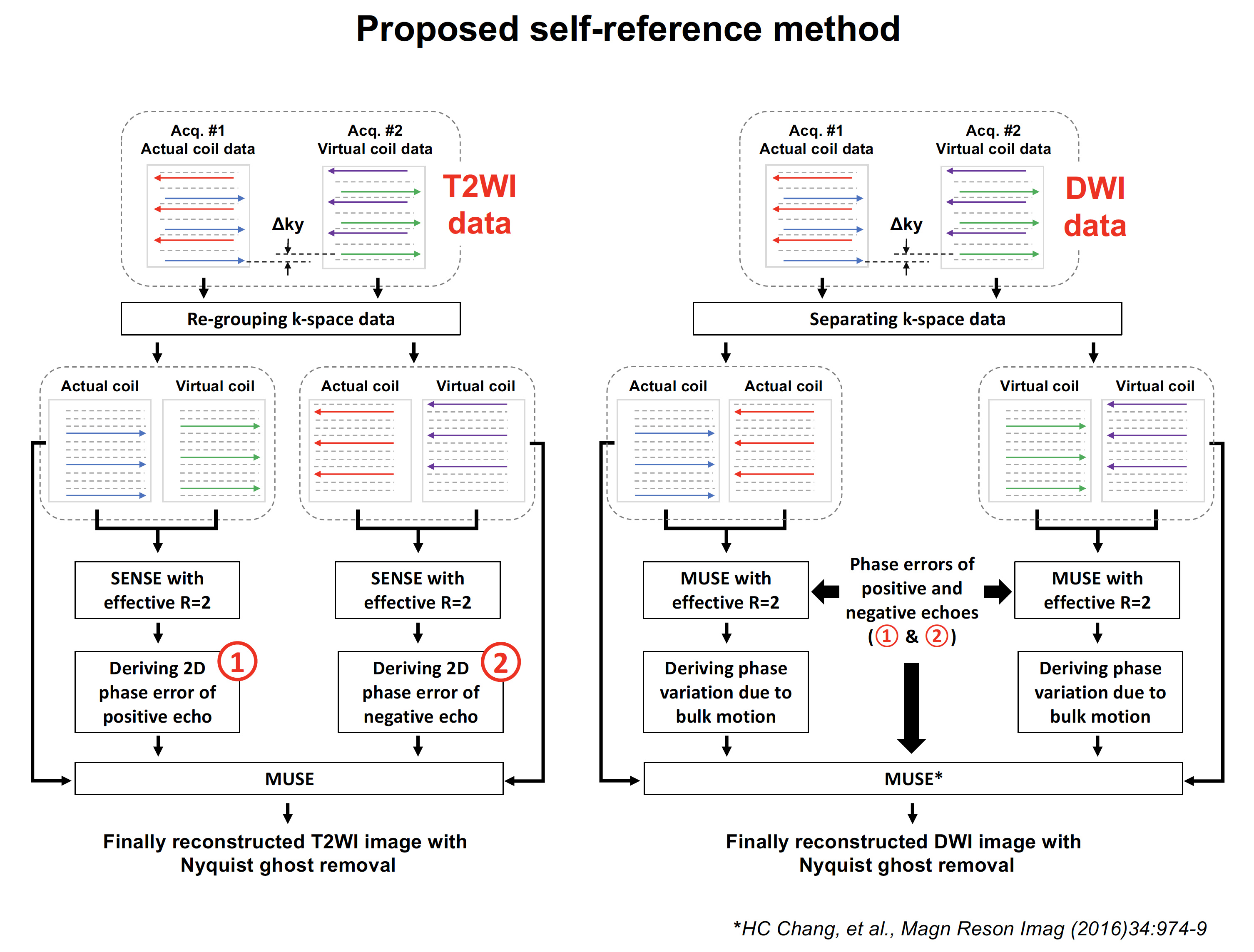
II. Virtual coil acquisition: We propose to adopt a virtual coil acquisition scheme3 during multiple acquisitions of both T2-weighted and DWI data. As shown in Figure 2, the k-space trajectory of second acquisition (i.e., which is equivalent to NEX of 2) shifted in phase encoding direction with Δky to create a virtual coil data set. Afterward, all positive and negative echoes from both actual and virtual coil T2WI data were respectively re-grouped together (i.e., left panel of Figure 2) to generate two data sets with effective R=2. Subsequently, each data set was unfolded with SENSE reconstruction to derive 2D phase error of either positive or negative echo.
III. Data reconstruction with MUSE: For DWI data of each acquisition, the unpredictable phase variations due to bulk motion were measured using MUSE algorithm with known 2D phase errors derived from T2WI data (i.e., right panel of Figure 2). Finally, both actual and virtual coil data were jointly reconstructed using MUSE algorithm4,5 to produce either T2-weighted or diffusion-weighted image without aliasing and Nyquist ghost.
IV. Evaluation study: The proposed method was tested on one healthy subject and 50 stroke patients at 1.5T MRI scanner (GE Healthcare) using an 8-channel head coil with 160x160 matrix size. All images reconstructed using proposed method were examined for each subject, and then compared with the images produced from scanner in terms of the occurrence of pseudo-lesion artifact, ADC measurement, SNR, and ghost-to-signal ratio (GSR). Only the subject data without pseudo-lesion artifacts were selected for quantitative assessment.
Results
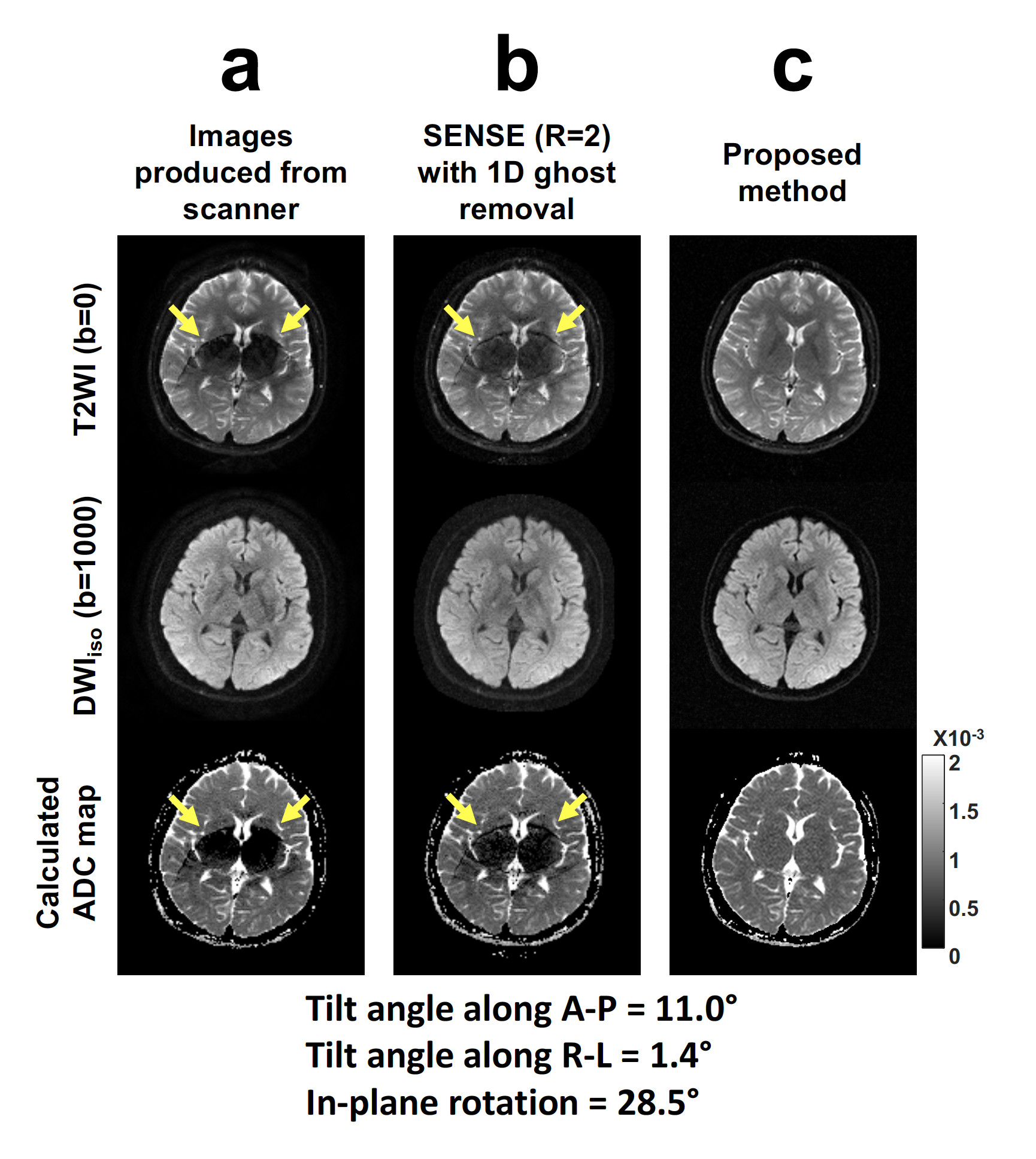
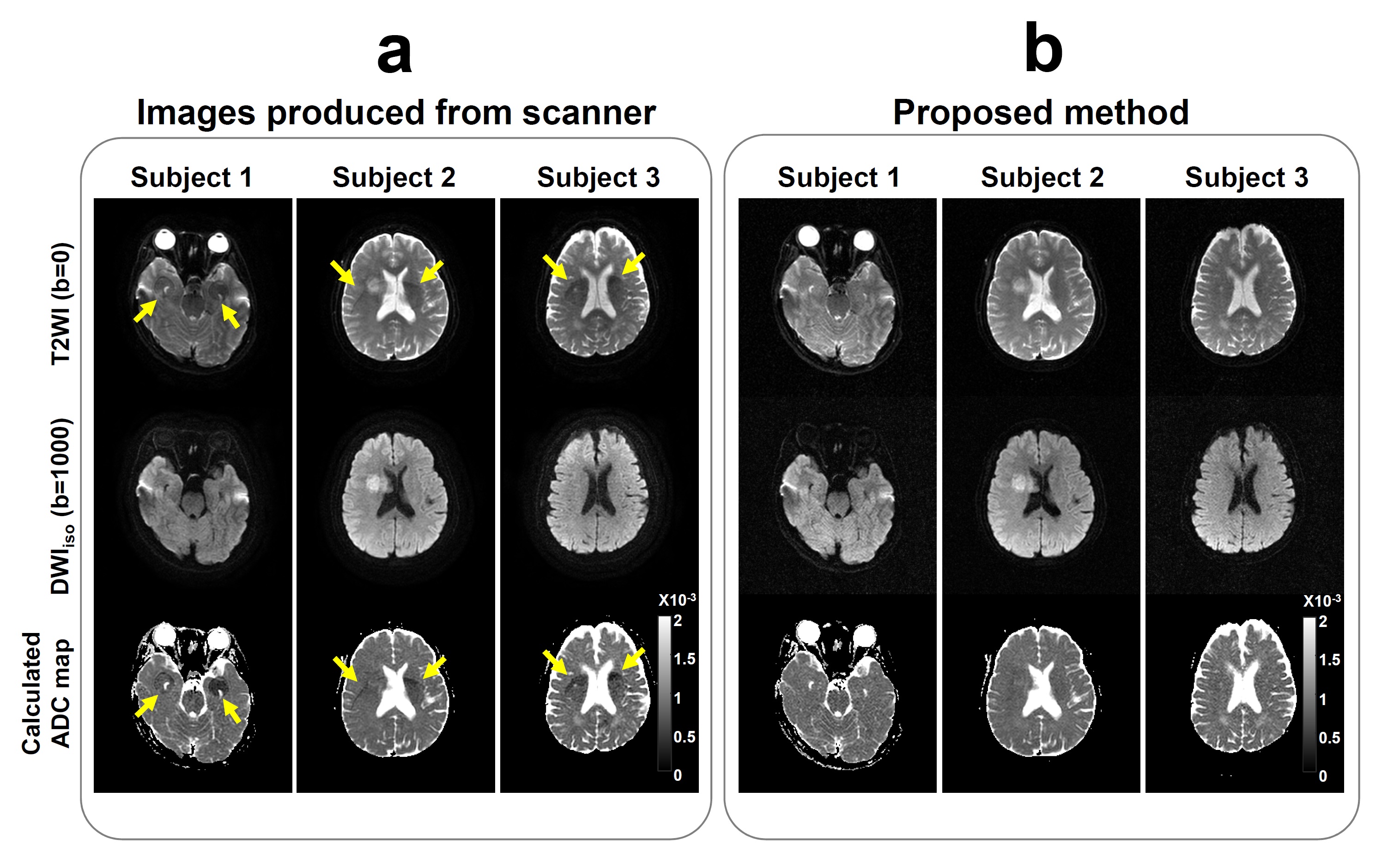
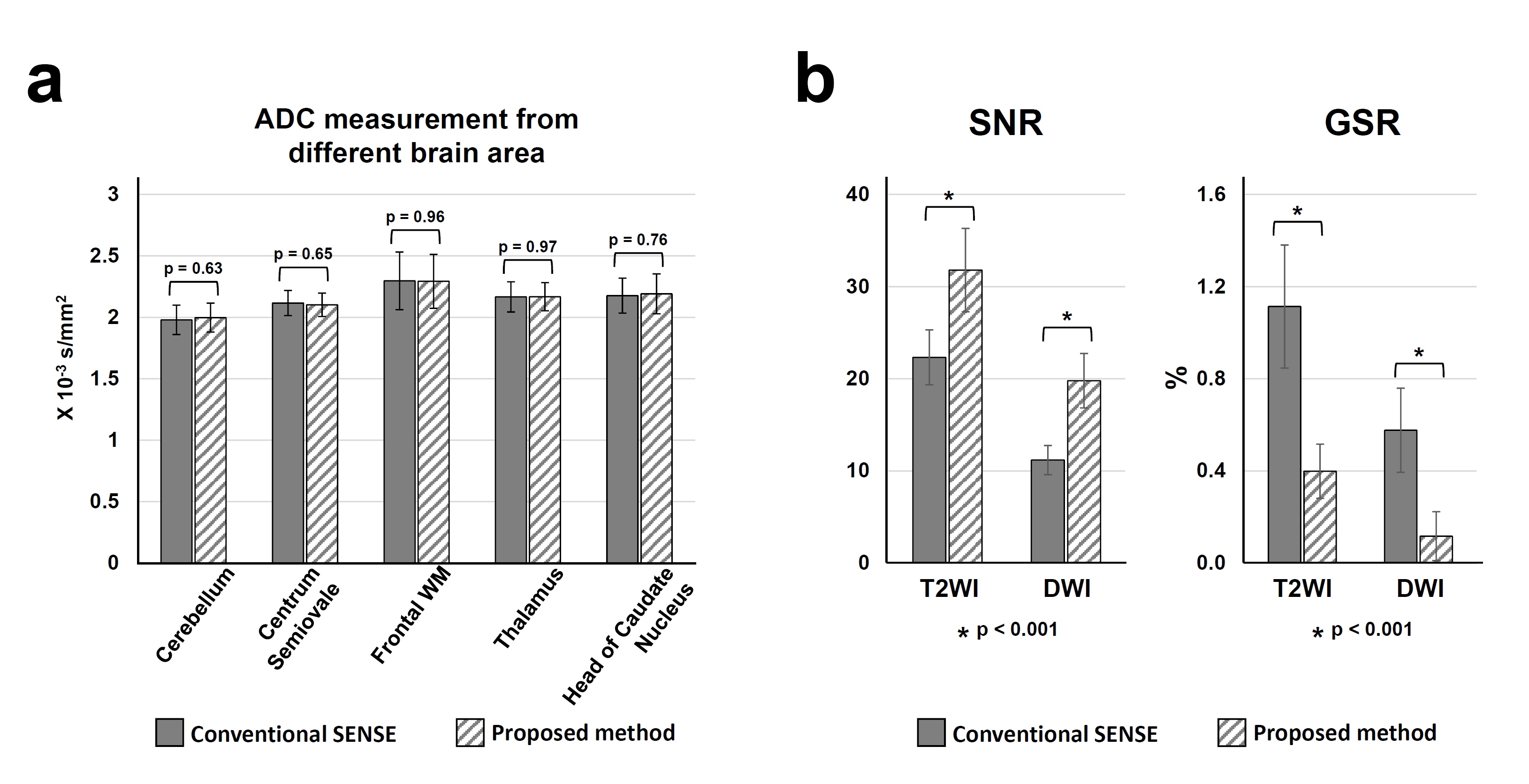
The incidence of pseudo-lesion artifact was 60% (i.e., 30 out of 50) from collected patient data. Figure 3 shows the double-oblique accelerated DW-EPI data acquired from a healthy subject with R=2 and NEX=2. The T2WI image produced from scanner shows prominent residual artifact which leads to pseudo-lesion artifact in calculated ADC map (arrows in Figure 3a). The raw data of images shown in Figure 3a was reconstructed using conventional SENSE reconstruction (Figure 1) that result in similar residual artifacts (arrows in Figure 3b) compared to images produced from scanner. Our proposed method could effectively remove the residual artifact (Figure 3c), thereby avoiding pseudo-lesion artifact. Figure 4 shows the comparison of images produced from scanner and reconstructed using our proposed method. Figure 5 shows the quantitative assessments of proposed method for 20 subjects with no prominent artifacts.Discussion
We have demonstrated that the proposed method can effectively remove 2D Nyquist ghost and unfold the aliased pixels for accelerated DW-EPI data with virtual coil acquisition (which is equivalent to NEX=2), thereby eliminating the occurrence of pseudo-lesion artifact due to double-oblique acquisition. The ADC values measured from images produced with proposed method are comparable with conventional SENSE reconstruction (Figure 5a). In addition, the joint reconstruction with both actual and virtual coil data can significantly improve SNR performance and reduce artifact level, compared with conventional SENSE reconstruction (Figure 5b). In conclusion, our proposed method can significantly improve the image quality of accelerated DW-EPI that is particularly useful in routine brain examination to obtain optimal image orientation for clinical diagnosis without suffering from pseudo-lesion artifact.Acknowledgements
This research is supported by grant from Hong Kong Research Grant Council (GRF HKU17121517).References
[1] Bammer R, Auer M, Keeling SL, Augustin M, Stables LA, Prokesch RW, Stollberger R, Moseley ME, Fazekas F. (2002) Diffusion tensor imaging using single-shot SENSE-EPI. Magn Reson Med. Vol.48(1), p.128.
[2] Chou MC, Wang CY, Liu HS, Chung HW, Chen CY. (2007) Pseudolesion arising from unfolding artifacts in diffusion imaging with use of parallwl acquisition: origin and remedies. Am J Neuroradiol. Vol.28, p.1099.
[3] Blaimer M, Cutberlet M, Kellman P, Breuer FA, Kostler H, Griswold MA. (2009) Virtual coil concept for improved parallel MRI employing conjugate symmetric signals. Magn Reson Med. Vol.61, p.93.
[4] Chen NK, Guidon A, Chang HC, Song AW. (2013) A robust multi-shot scan strategy for high-resolution diffusion weighted MRI enabled by multiplexed sensitivity-encoding (MUSE). Neuroimage. Vol.72, p.41.
[5] Chang HC, Chen NK. (2016) Joint correction of Nyquist artifact and minuscule motion-induced aliasing artifact in interleaved diffusion weighted EPI data using a composite two-dimensional phase correction procedure. Magn Reson Imag. Vol.34, p.974.
Figures