4105
Prospectively Respiratory-Cardiac Double-Triggered Three-Dimensional T2-Weighted Abdominal MRI1Global MR Applications and Workflow, GE Healthcare Japan, Hino, Japan, 2Office of Radiation Technology, Keio University Hospital, Tokyo, Japan, 3Department of Radiology, Keio University School of Medicine, Tokyo, Japan
Synopsis
We developed a prospective respiratory-cardiac double-triggering technique with navigator echo and incorporated it into 3D T2-weighted variable refocusing flip-angle fast spin echo (Cube) for abdominal MRI. The respiratory and cardiac navigator signals synchronized well with the signals from the external devices, and resultant double-triggered Cube images had higher sharpness scores of the left liver lobe than the respiratory-triggered Cube images. The double-triggering technique is feasible and can be applied to other applications where both respiratory and cardiac motions are problematic.
Introduction
Respiratory motion is one of the major issues in abdominal MRI, and cardiac motion also affects image quality of the liver in 3D T2-weighted variable refocusing flip-angle fast (turbo) spin echo imaging.1 External devices such as respiratory bellows and a probe for peripheral gating (PG) can be used for such motion artifact reduction, but their settings are time- and effort-consuming. In this study, we developed a prospective respiratory-cardiac double-triggering technique with navigator echo and we incorporated it into 3D T2-weighted variable refocusing flip-angle fast spin echo (Cube) for abdominal MRI. We demonstrated the feasibility in volunteer abdominal experiments.Methods
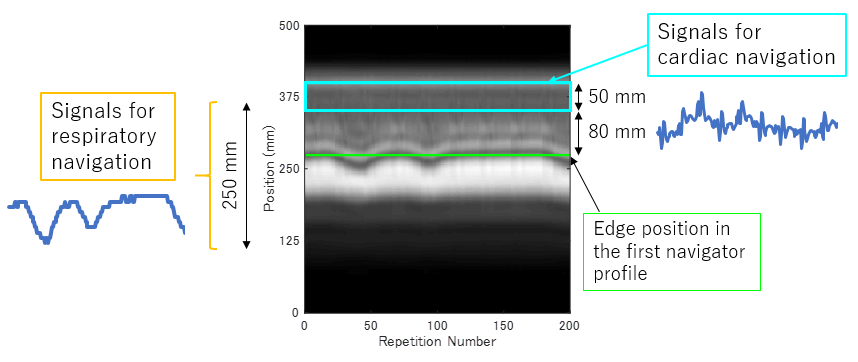
Navigator Pulse Sequence and Signal Processing: A non-selective hard excitation RF pulse was used for excitation of whole volume including the liver and heart. A read-out gradient pulse in the SI direction followed the excitation. The navigator sequence was repeated every 50 ms and signals were used both for respiratory and cardiac navigation (Fig. 1). Respiratory navigator (rNav) signal processing was performed using the least-squares error method2 and 250-mm data sets from 500-mm navigator profiles were used for squared error calculation. Coil selection was performed in rNav signal synthesis for reduction of static tissue signals.3 Cardiac navigator (cNav) signals were synthesized by summing up the signals from the 50-mm region whose bottom is 80 mm above the liver edge in the first navigator profile. Since the cNav signals are also influenced by respiration, cardiac motion detection process was activated only when the rNav displacement value was within a ±6mm window around the end-expiration position. Cardiac trigger points were detected when the cNav signal increased monotonically to exceed a threshold. The threshold was determined based on the cNav signal variation in a 10-sec learning phase scan.
Respiratory-cardiac double-triggering was conducted in a sequential manner. First, rNav detected the end-expiration with the acceptance window of ±2mm. Second, cNav triggered the imaging sequence after it detected a cardiac trigger point.
Data Acquisition: We performed all experiments on a GE 3 T MR750 imaging system. Respiratory-cardiac double-triggered Cube scans were performed with five healthy volunteers using a 32-channel phased array coil. Respiratory-triggered Cube scan was also conducted without cardiac triggering for comparison purpose. 3D data were acquired in the coronal orientation with imaging parameters: parallel imaging using ARC with an acceleration factor of 2 × 1, TR/TE = 1 × respiratory cycle/54–62 ms, FOV = 36–44 cm, matrix = 224 × 192, slice thickness = 3.0 mm, 56 slices, NEX = 1, receiver bandwidth = ±100 kHz, and ETL = 120.
Data Analysis: After selection of the images including both the liver and heart, sharpness of the left liver lobe was evaluated quantitatively. 4 In short, edge values were calculated for both upper and lower sides of the left liver lobe using a first-order derivative, and final sharpness was defined as the average score of both sides divided by the liver parenchyma signal.
Results
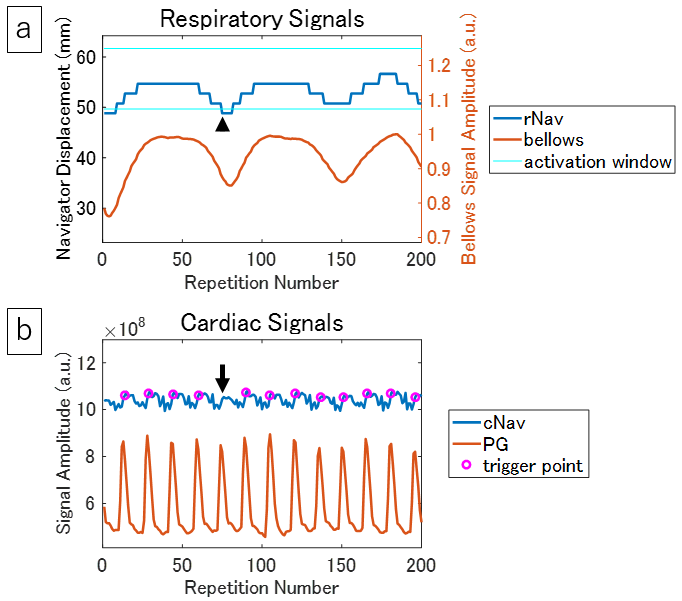
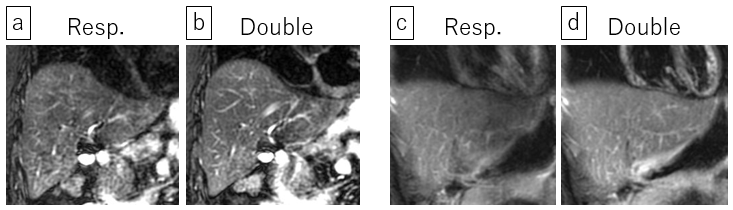
Figure 2 shows rNav and cNav signals obtained from the same navigator raw data in a 10-sec learning phase scan. Good synchronization was observed between rNav and bellows signals, and between cNav and PG signals. Trigger points in cNav were detected at similar timings of the PG signal peaks. The average scan times were 177 sec and 240 sec for respiratory-triggered and respiratory-cardiac double-triggered Cube scans, respectively. Figure 3 shows the quantitative sharpness values of the left liver lobe in respiratory-triggered and double-triggered Cube images. The sharpness value of double-triggered Cube was more than 10% higher than that of respiratory-triggered Cube for four subjects. The score of double-triggering was lower for volunteer 4, but the difference was less than 3%. Examples of Cube images are shown in Figure 4. Delineation of the left liver lobe and myocardium was improved in double-triggered images.Discussion and Conclusion
We have demonstrated that both respiratory and cardiac motions can be detected from navigator echoes with whole volume excitation, and that prospectively double-triggering technique improves delineation of the left liver lobe in T2-weighted Cube images. This double-triggering technique can be applied to other applications such as DWI where both respiratory and cardiac motions can deteriorate image quality of the liver. Clinical evaluation with a large number of subjects is required in future.Acknowledgements
References
1. Takayama Y, Nishie A, et al. Three-dimensional T2-weighted imaging for liver MRI: clinical values of tissue-specific variable refocusing flip-angle turbo spin echo imaging. J Magn Reson Imaging. 2015;41:339–346.
2. Wang Y, Grimm RC, et al. Algorithms for extracting motion information from navigator echoes. Magn Reson Med. 1996;36:117–123.
3. Iwadate Y, Nozaki A, et al. Silent navigator-triggered silent MRI of the abdomen. Magn Reson Med. 2017;DOI:10.1002/mrm.26869.
4. Botnar RM, Stuber M, et al. Improved coronary artery definition with T2-weighted, free-breathing, three-dimensional coronary MRA. Circulation. 1999;99:3139–3148.
Figures