3984
23NA-MRI of the skeletal muscle and skin in patients with adrenal insufficiency1Department of Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany, 2Department of Medicine I, University Hospital Würzburg, Würzburg, Germany, 3Comprehensive Heart Failure Center, University Hospital Würzburg, Würzburg, Germany
Synopsis
Patients with chronic primary adrenal insufficiency require life-long glucocorticoid- and mineralocorticoid- replacement therapy. Monitoring of treatment is mainly based on clinical parameters and additional measurement of electrolyte status and plasma renin levels. However, obtained values often do not correspond to the patients’ subjective well-being and thus may not fully reflect optimal treatment. The present study investigated sodium content in the calf muscle and the skin obtained via 23Na-MRI in patients with chronic primary AI and healthy controls. Sodium content assessed by 23Na-MRI correlates with further parameters of mineralocorticoid activity and may serve as an objective method to monitor hormone substitution therapy in patients with adrenal insufficiency.
Introduction
Aldosterone plays an important role in sodium homeostasis. Patients suffering from primary aldosteronism (excess production of aldosterone) present with higher sodium concentrations in the skin, the skeletal muscle and the myocardium compared to healthy controls1,2 and values normalize following treatment.2 Patients suffering from adrenal insufficiency (AI) typically present with low concentrations of aldosterone and are treated by hormone substitution which, however, does not completely resemble normal physiology. Adequate substitution is monitored by checking the patients’ subjective well-being, hormone- and electrolyte-status and blood pressure.3 However, often subjective well-being and blood values point in different directions indicating a need for better monitoring strategies that provide more reliable data.3 We aimed to investigate the potential role of 23Na-MRI for monitoring of mineralocorticoid replacement by investigating tissue sodium concentrations in patients with AI.Methods
We examined 16 patients under established hormone substitution therapy (chronic AI, C_AI) and six patients with newly diagnosed adrenal insufficiency (N_AI). Results were compared to data from 16 healthy controls (HC). For determination of sodium concentration in the calf muscle, we set up a 23NA-MRI protocol on a 3T scanner (Magnetom PRISMA, Siemens, Erlangen) implementing a 3D sequence with the following parameters: TR 100 ms; TE 2.01 ms; flip angle 90°; FOV 500 x 500 mm2; acquisition matrix 128 x 128; 10 slices with thickness 20 mm; 8 averages; acquisition time ~17 min. To minimize partial volume effects during sodium content estimation in the skin we adapted the sequence (slice thickness 30 mm, acquisition matrix 384 x 42) to acquire very flat voxels. For signal detection, we used a dual tuned 23Na/1H surface coil (Rapid Biomed, Rimpar). To calculate semiquantitative sodium concentrations external reference standards with known concentrations in aqueous solution were placed inside the FOV during every measurement. Relative sodium signal intensities (rSSI) were calculated as ratio of tissue sodium intensity and the intensity of a vial containing a concentration of 100mmol/l. A clinical score for estimation of the quality of the hydrocortisone-replacement was obtained for C_AI patients and compared to rSSI. Lower values are supposed to indicate insufficient substitution while higher values suggest over-substitution with hydrocortisone. Due to the low number of patients with N_AI, statistical testing for differences in rSSI was only performed for the patients under chronic replacement therapy and healthy controls. rSSI was compared to sodium content in 24-hour urine samples (24h-Sod) using Pearson’s correlation coefficient r. rSSI and 24h-Sod of the two groups (C_AI, HC) was compared by Mann-Whitney-U test.Results
Figure 1 summarizes the rSSI results for all patients and healthy controls. rSSI of the patients with N_AI (skin: 11.8±3.3; calf: 14.0±3.5) was much lower compared to the values from healthy controls (skin: 17.1±4.7; calf: 16.0±2.5) for both compartments. Observed differences between C_AI patients and healthy controls were not significant for rSSI of the skin but significant for rSSI of the calf muscle (C_AI 18.8±2.0 vs HC 16.9±2.0; p<0.05). A significant correlation was found for rSSI in the skin and 24h-Sod for the whole cohort (r=0.474, p<0.05, figure 2). When correlating the subgroups alone we observed r=0.212, p=0.487 (patients) and r=0.516, p<0.05 (HC). No significant correlation was found when comparing rSSI of the calf muscle to 24h-Sod. When comparing rSSI of the skin and the calf muscle of C_AI patients with the obtained clinical score a trend from lower rSSI for low scores to higher rSSI for higher scores was observed (figure 3).Discussion
Our results show that tissue sodium content in patients with newly diagnosed adrenal insufficiency is heavily decreased compared to both healthy controls and patients under established replacement therapy. Patients under hormone replacement therapy did not present with significantly different rSSI in the skin in our cohort. However, rSSI in the calf muscle was significantly higher when compared to healthy controls. The good agreement between rSSI and the obtained clinical score indicates that rSSI obtained from 23Na-MRI might be a quantitative marker when monitoring hydrocortisone replacement. However, the limited spatial resolution might result in partial volume effects when estimating sodium content in the calf muscle. Due to the fast T2 decay of the sodium signal and the echo time used, a great proportion of the overall sodium signal was not detected in our study.Conclusion
In the course of hormone substitution, 23Na-MRI might serve as an additional tool for treatment monitoring.Acknowledgements
No acknowledgement found.References
1. Christa M, et al. Increased myocardial sodium storage in Conn’s syndrome detected by 23Na magnetic resonance imaging. Clin Res Cardiol. 2016;105(Suppl 1):[P753]
2. Kopp C, et al. 23Na Magnetic Resonance Imaging of Tissue Sodium. Hypertension 2012;59:167-172
3. Quinkler M, et al. Mineralocorticoid substitution and monitoring in primary adrenal insufficiency. Best Pract Res Clin Endocrinol Metab. 2015;29(1):17-24
Figures
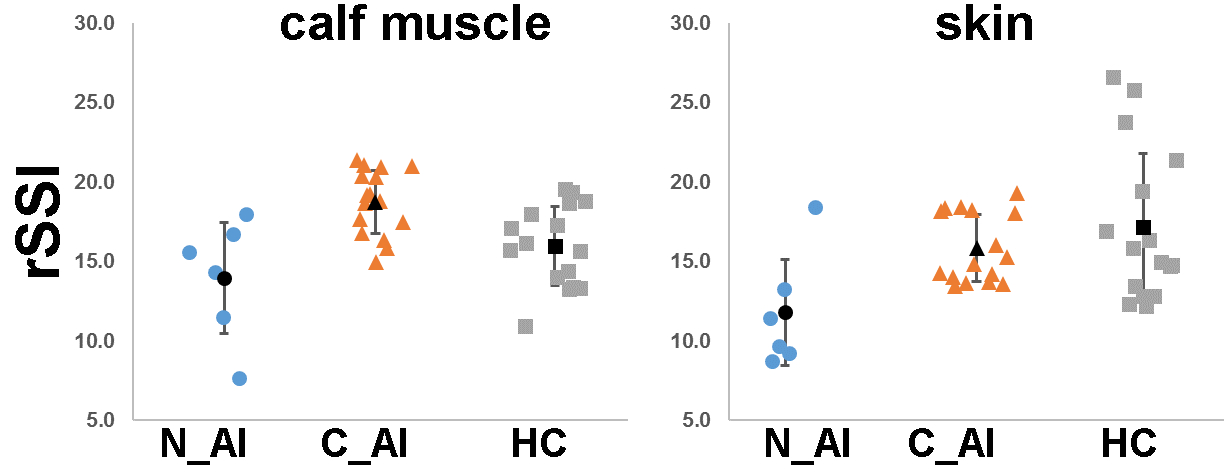
Relative sodium signal intensities (rSSI) for calf muscle and skin for all investigated groups: newly diagnosed adrenal insufficiency (N_AI), patients with chronic adrenal insufficiency (C_AI) and healthy controls (HC).
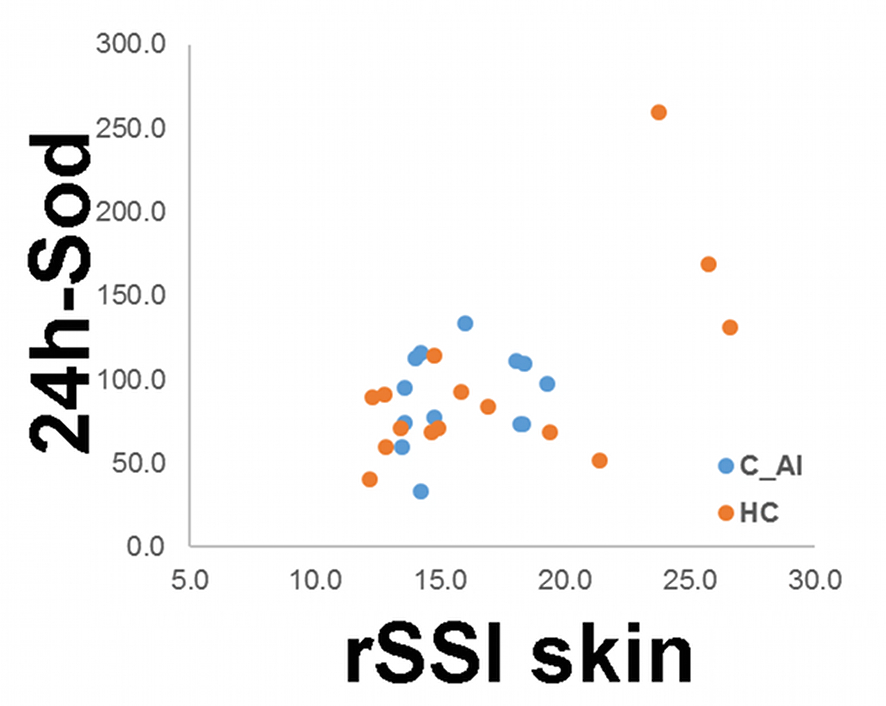
Amount of sodium in 24-hour urine collection vs. relative sodium signal intensity of the skin. A significant overall correlation (C_AI and HC) was observed. However, for patients (C_AI) no significant correlation was found while for the healthy controls (HC) correlation was again significant.
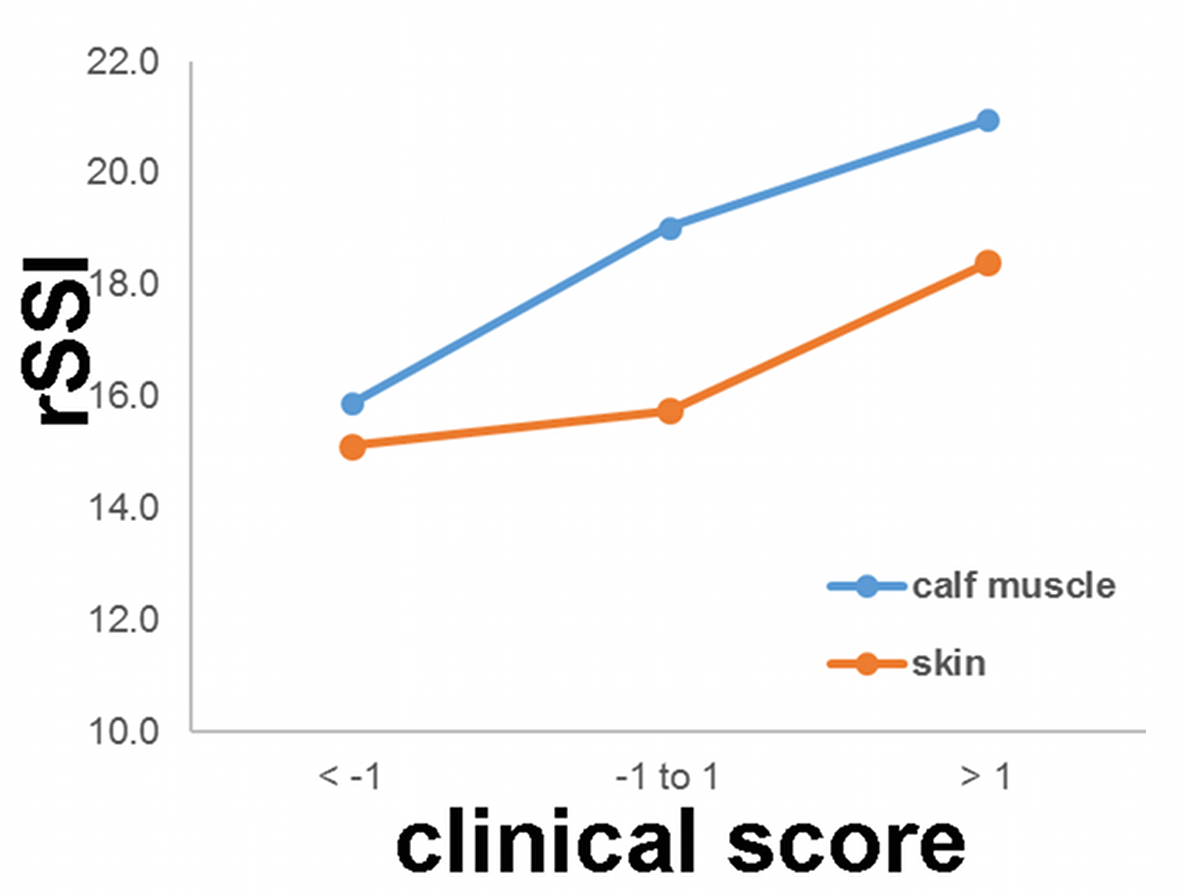
Presented are the mean rSSI of the skin and the calf muscle from the patients (C_AI) versus the obtained clinical scores. Note that lower scores indicate insufficient hormone substitution resulting in lower rSSI values while higher scores indicate over-substitution resulting in higher rSSI values.