3833
Pilot Study of Rapid MR Pancreas Screening for Patients with BRCA Mutation1Radiology, MSKCC, New York, NY, United States, 2St. John's University, Jamaica, NY, United States, 3Radiology, Università degli studi di Cagliari, CAGLIARI, Italy
Synopsis
Patients with BRCA mutations are offered breast MRI because of their increased risk of breast cancer, but no screening strategy is available for other BRCA-associated malignancies including pancreatic ductal adenocarcinoma. In this protocol, we optimize the use of several recent developments in body MRI for a rapid pancreatic screening in BRCA mutation carriers: first, rapid relatively motion insensitive T2-weighted imaging (T2WI) and navigator triggering (NT), where real-time tracking of the diaphragm position is performed. Secondly advances in diffusion-weighted-imaging (DWI). These techniques have changed our ability to screen for malignancies, in specific organs, such as the pancreas.
Purpose:
To develop and optimize rapid pancreatic screening magnetic resonance imaging (MRI) protocols to be performed after a screening breast MRI in BRCA mutation carriers. To optimize image quality of novel navigation triggering NT high resolution 3D T1 weighted images. To evaluate the feasibility of reduced field-of-view (FOV) diffusion weighted images (DWI) acquired with FOV optimized and constrained undistorted single-shot (FOCUS) and built-in body coils, for pancreatic study in patients in prone position at the end of a contrast enhanced breast MRI.Methods:
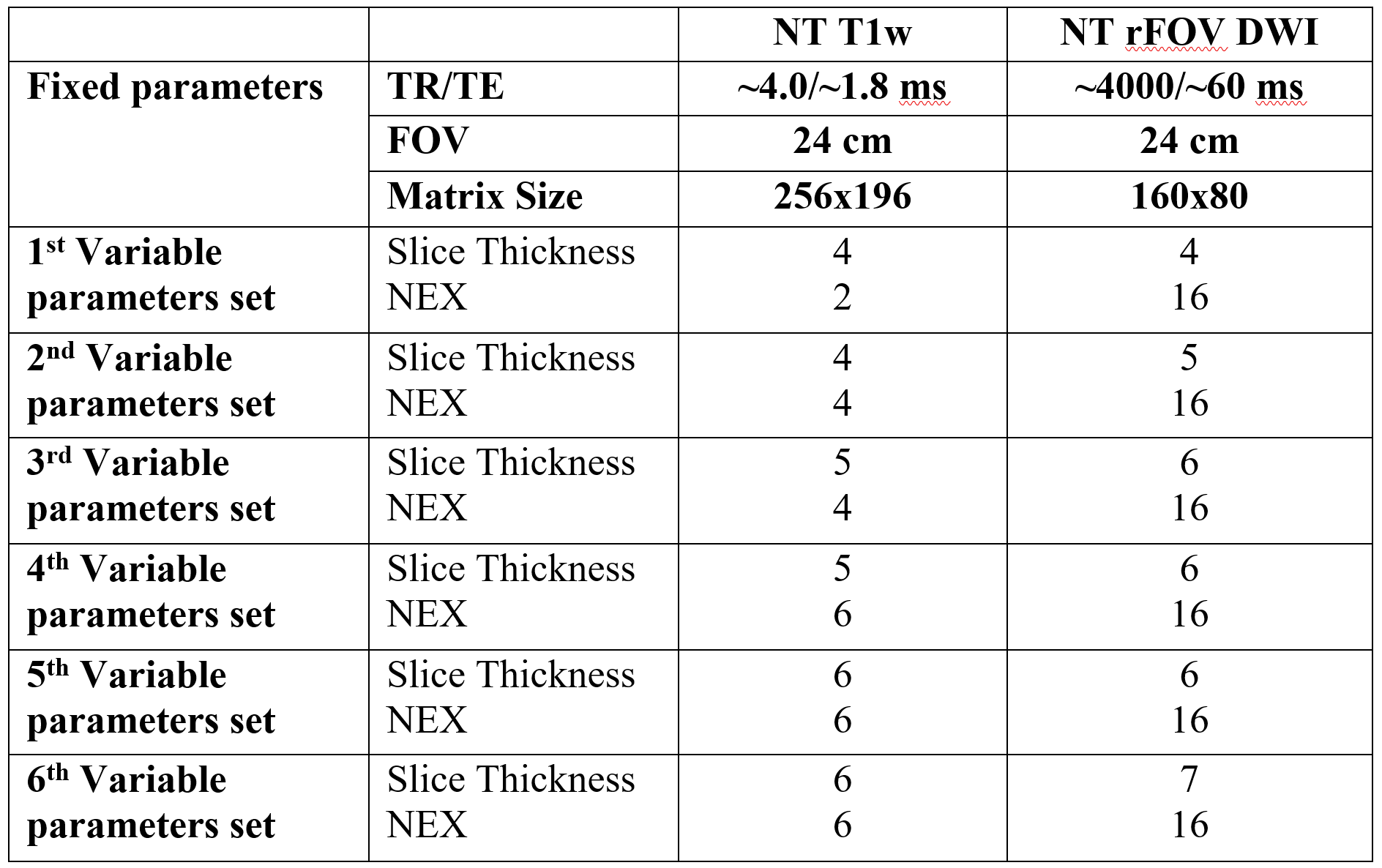
This prospective study was approved by the local IRB and was HIPAA compliant. Written informed consent obtained from each participant. Between July 2015 and August 2017 39 individuals, who were also participating in a prospective Registry for BRCA mutation Carriers with Pancreas Ductal Adenocarcinoma (PDAC), were recruited. The participants in the Rapid Pancreas MRI imaging study were from control cohorts of the Registry, and were themselves known BRCA mutation carriers. Inclusion criteria: BRCA1 or BRCA2 mutation, age 25 years or older, female, and undergoing screening breast MRI. The rapid screening protocol was designed to be completed in less than 10 minutes at the completion of the breast MRI examination. The images were acquired with the patient in the prone position, with the breast coil still in place, but using the built-in body coil without placement of a dedicated phased array body coil. Image quality was qualitatively assessed by two radiologists in consensus. Sequence parameters were changed according to table 1 anytime a patient did not have a complete exam with diagnostic images (score of 1) for all sequences. The protocol was deemed optimized by design once diagnostic images (score of 1) were achieved for 5 consecutive patients. Signal-to-noise-ratio (SNR) and contrast-to-noise-ratio (CNR) were assessed with manually placed 5mm regions-of-interest (ROI)in the pancreatic head, body, and tail. Mean signal intensity (S) and standard deviation (SD) in each ROI were recorded. In those sequences where available (T2 SSFSE axial and T1 post-contrast axial) a ROI was placed in the background air for a direct assessment of image noise according to the following equations:
$$$SNR=Spancreas∖SDair (1)
$$$CNR=Spancreas−Sfat∖SDair (2)
As the rFOV DWI sequences did not include background air, in 8 patients the DWI sequence was repeated during the same examination, allowing SNR to be calculated using subtraction methods (NEMA Standards Publication MS 1-2008 (R2014), Determination of Signal-to-Noise Ratio (SNR) in Diagnostic Magnetic Resonance Imaging). Statistical analysis was performed using Software Package R, version 3.1.
Results:
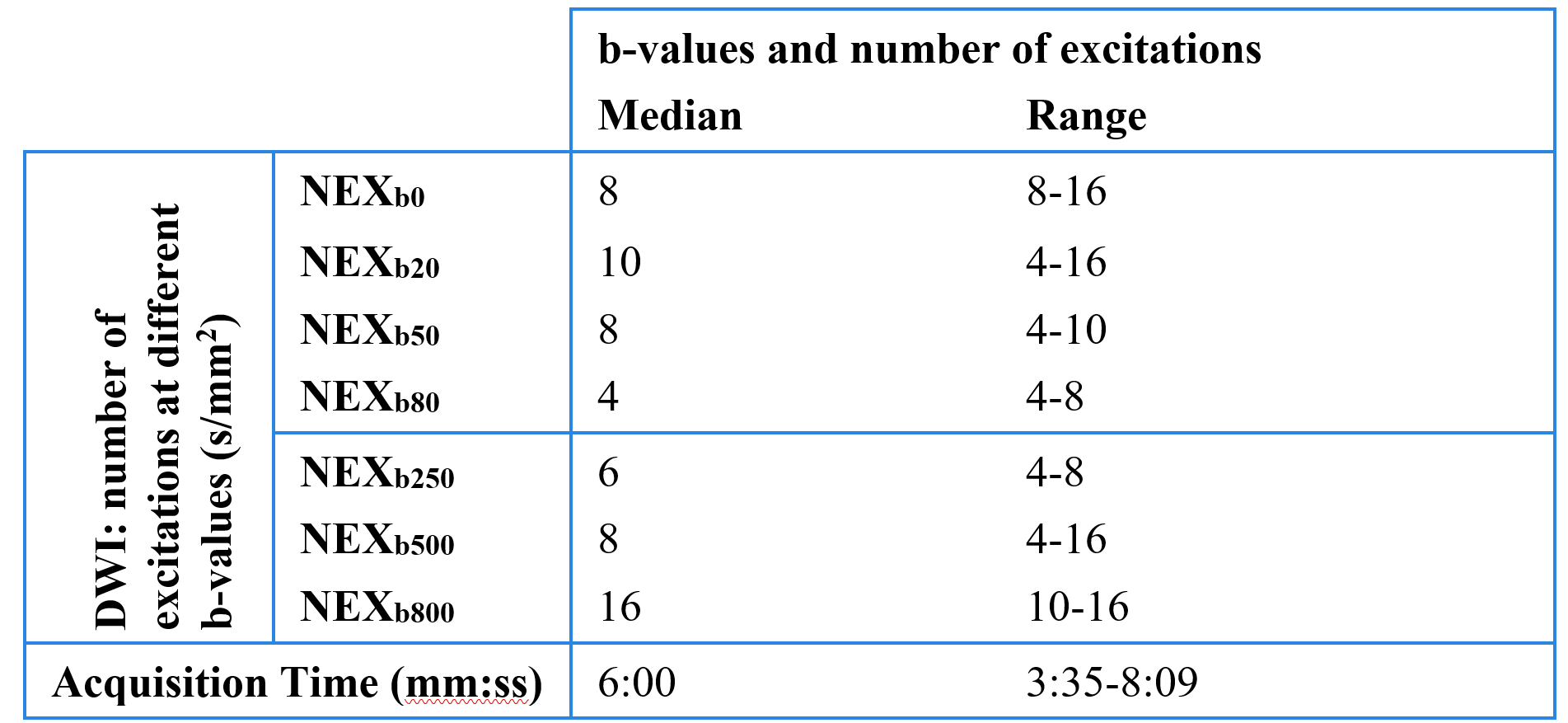
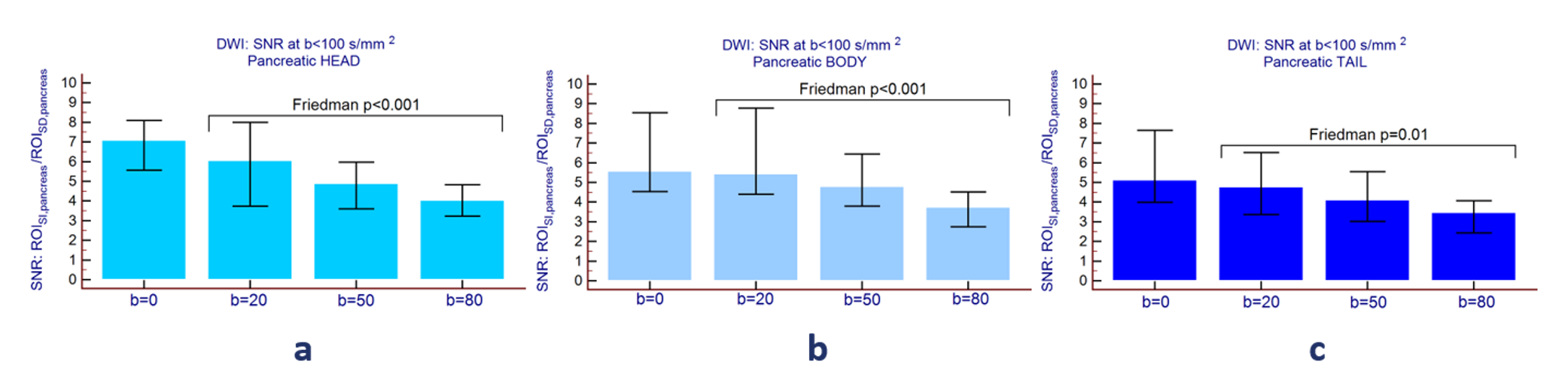
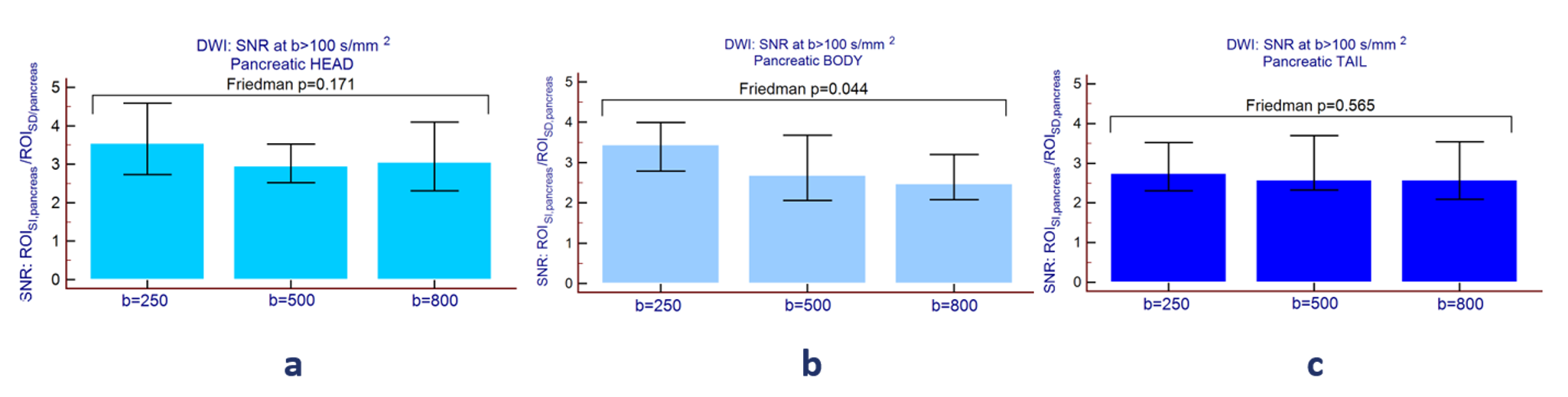
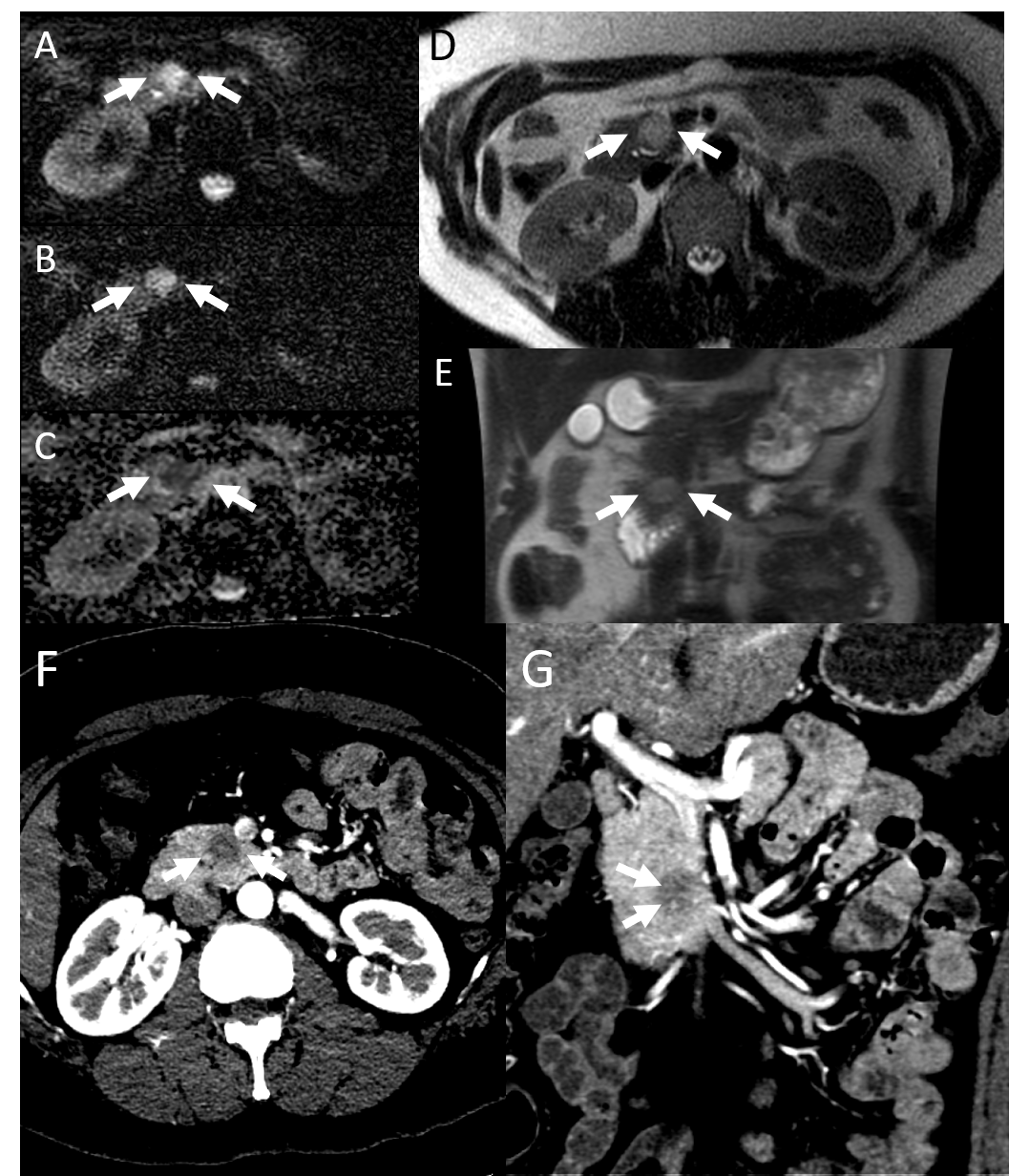
The final population included 40 women. The mean age was 51.4 years (range 32.7 – 76.9). The rapid pancreas MR protocol was successfully completed in all patients with parameters as shown in table in figure 2 for DWI imaging. Diagnostic image quality was achieved for all patients after patient number 7. Excellent image quality was achieved for low b-values; however, image quality at higher b-values was more variable. Adequate SNR and CNR values were obtained using the built-in body coil, particularly for the T2 SSFSE and T1 weighted sequences and lower b values up to 250 s/mm2. For the higher b-values of 500 and 800 s/mm2 the lower SNR obtained accounted for the subjectively lower image quality scores assigned. SNR for the rFOV DWI sequence is reported in Figure 3 for b values < 100 s/mm2 and in figure 4 for b values > 100 s/mm2. In 4 patients, small pancreatic cystic lesions were detected. In one subject a hepatic adenoma was identified. In one patient pancreatic adenocarcinoma was highly suspected and confirmed with a dedicate MR exam (Figure 5).Discussion
This study demonstrates that rapid pancreas MRI screening using the built-in body coil on a 3T magnet is feasible under 10 minutes, yielding diagnostic image quality for the pancreas. Combined with breast MRI screening, this study offers a rapid, non-invasive, and potentially inexpensive screening tool of the pancreas for BRCA patients. With minimal inconvenience to the patient, this screening protocol can be potentially useful in the high-risk BRCA population where currently there is no established screening tool available.Conclusion
Rapid MR protocol for pancreatic cancer screening with subjects in the prone position and use of the built-in body coil is feasible and provides diagnostic quality images, helping in the detection of benign and malignant alterations.Acknowledgements
No acknowledgement found.References
1Greer JB, Whitcomb DC. Role of BRCA1 and BRCA2 mutations in pancreatic cancer. Gut. 2007;56(5):601-605 2 Petrucelli N, Daly MB, Feldman GL. Hereditary breast and ovarian cancer due to mutations in BRCA1 and BRCA2. Genet Med. 2010;12(5):245-259 3 Chang MC, Wong JM, Chang YT. Screening and early detection of pancreatic cancer in high risk population. World J Gastroenterol. 2014;20(9):2358-2364 4 Hahn SA, Greenhalf B, Ellis I, et al. BRCA2 germline mutations in familial pancreatic carcinoma. J Natl Cancer Inst. 2003;95(5):214-21 5 Canto MI, Harinck F, Hruban RH, et al. International cancer of the pancreas screening (CAPS) consortium summit on the management of patients with increased risk for familial pancreatic cancer. Gut 2013;62(3):339-47 6 National Comprehensive Cancer Network. Breast cancer screening and diagnosis (Version 1.2016). https://www.nccn.org/professionals/physician_gls/pdf/breast-screening.pdf Accessed September 5, 2016. 7 Ludwig E, Olson SH, Bayuga S, et al. Feasibility and yield of screening in relatives from familial pancreatic cancer families. Am J Gastroenterol. 2011;106(5):946-954 8 Vasen H, Ibrahim I, Ponce CG, et al. Benefit of surveillance for pancreatic cancer in high-risk individuals: outcome of long-term prospective follow-up studies from three European expert centers. J Clin Oncol. 2016;34(17):2010-2019 9 Cucchetti A, Ercolani G, Cescon M, et al. Estimation of the survival benefit obtainable from screening for the early detection of pancreatic cancer. Pancreas 2016;45(5):714-719 10 Pandharipande PV, Heberle C, Dowling EC, et al. Targeted screening of individuals at high risk for pancreatic cancer: results of a simulation model. Radiology 2015;275(1):177-187 11 Kim H, Lee JM, Yoon JH, et al. Reduced field-of-view diffusion-weighted magnetic resonance imaging of the pancreas: comparison with conventional single-shot echo-planar imaging. Korean J Radiol. 2015;16(6):1216-1225 12 Canto MI, Hruban RH, Fishman EK, et al. Frequent detection of pancreatic lesions in asymptomatic high-risk individuals. Gastroenterology. 2012;142(4):796-804 14 Del Chiaro M, Verbeke CS, Kartalis N, et al. Short-term results of a magnetic resonance imaging-based Swedish program for individuals at risk for pancreatic cancer. JAMA Surg. 2015;150(6):512-518 15 Canto MI, Goggins M, Hruban RH, et al. Screening for early pancreatic neoplasia in high-risk individuals: a prospective controlled study. Clin Gastroenterol Hepatol. 2006;4(6):766-781 16 King SB, Matwiy J, Bewsky C, Lin HY, Haider MA. An indenting abdominal array for 2-fold SNR improvement in pancreatic MRI. Abstract presented at ISMRM 24th Annual Scientific Meeting, Singapore, May 2016. http://cds.ismrm.org/protected/16MPresentations/abstracts/0531.html Accessed September 5, 2016Figures