3781
White matter fibre tract changes in patients treated with MR imaging-guided focused ultrasound are associated with lesion location and clinical outcome1Department of Radiology, Stanford University, Stanford, CA, United States, 2Department of Diagnostic and Interventional Neuroradiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 3Department of Electrical Engineering, Stanford University, Stanford, CA, United States, 4Department of Neurosurgery, Stanford University, Stanford, CA, United States
Synopsis
DTI is sensitive to tract-specific FA changes and thereby can be used to inform on therapeutic mechanisms and optimal targeting strategies for MRI-guided high intensity–focused ultrasound. Here, we used probablilistic tractography to investigate white matter fibre tract changes in essential tremor patients treated with MRIgHIFU. On the treated side, a significant decrease in FA was detected in the tracts projecting between the thalamus and motor cortex and between the dentate nucleus and the thalamus (i.e. the dentato-rubro-thalamic tract). These decreases in FA were correlated with the degree of tract-lesion overlap. Additionally, the post-treatment FA decrease in the tracts projecting between the thalamus and the motor cortex were positively correlated with clinical improvement. Interestingly, tract changes were also observed in the medial lemniscus of the contralesional side, possibly indicating global changes in brain connectivity.
Introduction
In recent years, MRI-guided high intensity–focused ultrasound (MRgHIFU) has become a new treatment option for movement disorders, including essential tremor.[1,2] However, little is known about the underlying mechanisms leading to tremor suppression or the impact of MRgHIFU on thalamic connectivity. Recent studies demonstrated improving clinical scores by directly targeting pre-defined fibre tracts instead of conventional targeting of the nucleus ventralis intermedius (VIM), suggesting an involvement of specific motor pathways.[3,4] The objective of this study was to investigate global tract fractional anisotropy (FA) changes of several pre-defined white matter tracts in patients with essential tremor who were treated with MRgHIFU.Methods
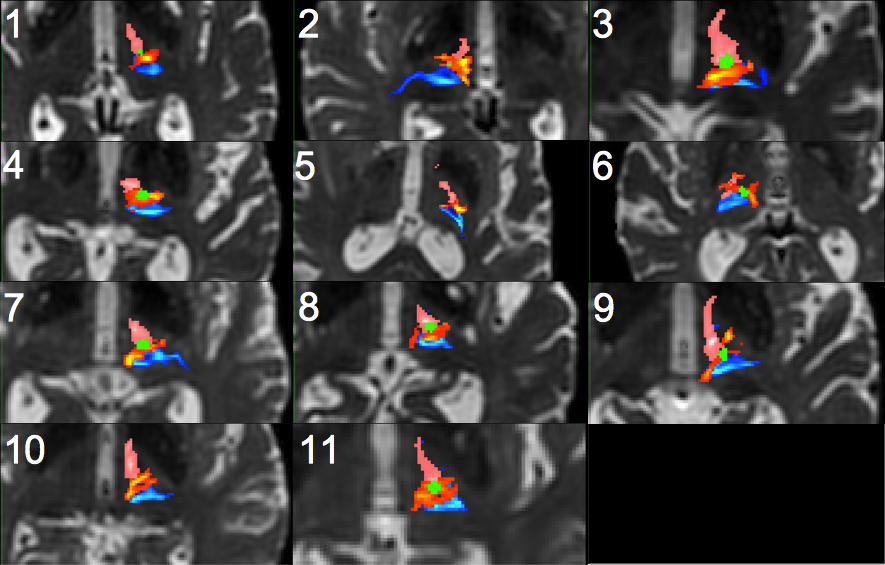
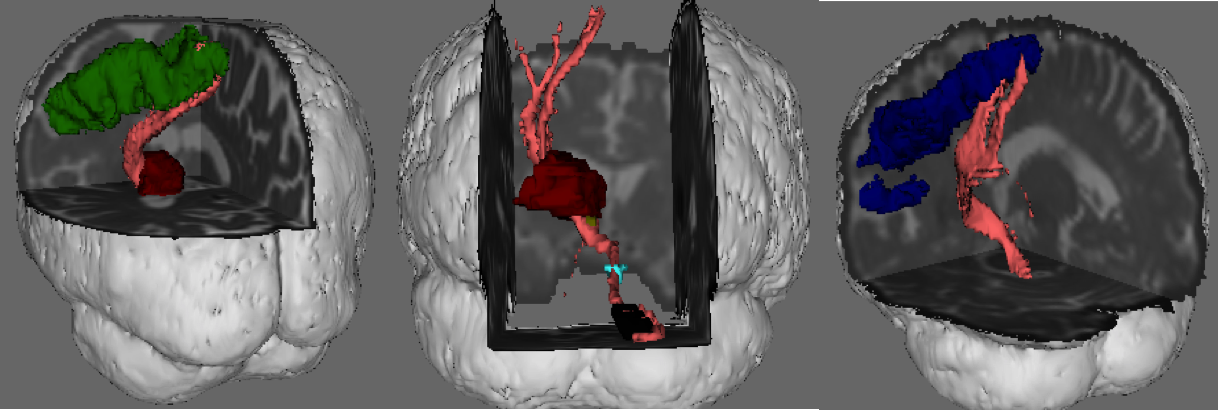
MRgHIFU was performed in 11 patients with medically refractory essential tremor, targeting the VIM contralateral to their dominant hand.[1] All patients received MRI (3T, GE Healthcare) prior to the procedure as well as 1 year after the treatment, including structural and diffusion weighted imaging (b=2500s/mm2, 60 directions, in-plane resolution = 1.875 x 1.875 mm2, acquisition time = 10 min) . Additionally, clinical status was assessed using the Clinical Rating Scale for Tremor (CRST)[5] at both dates. Tractography Image pre-processing and probabilistic tractography were performed using tools from the FMRIB Software Library (FSL, v5.0.7, http://fsl.fmrib.ox.ac.uk/fsl/fslwiki/).[6] Tractography was performed bilaterally to reconstruct the dentato-rubro-thalamic tract (DRTT), the medial lemniscus (ML) and the tracts between thalamus and primary motor cortex on pre-treatment data (Figure1). Tracts from the pre-treatment data were thresholded to 1% of the total number of streamlines between seed and target (i.e. the waytotal number), binarized and multiplied with the corresponding fractional anisotropy (FA) maps. Further, tracts from the pre-treatment data were co-registered to the post-treatment DTI space and multiplied with the post-treatment FA maps. Additionally, an ROI covering the MRgHIFU lesion was drawn for each patient and the mean pre-and post-treatment FA values within the lesion were computed. The overlap between the tracts and the lesion was calculated and correlated with changes in FA values in the corresponding tract. Tract changes were also correlated with clinical outcomes. FA values within the DRTT and ML were normally distributed and therefore a one-sided paired T-test was used to compare pre and post-treatment mean FA means. FA values within the thalamus-motor cortex tract were not normally distributed and therefore a Wilcoxon Signed Rank Test was used to compare pre and post-treatment FA. Pearson correlation was used to test for associations between tract changes and clinical outcome as well as tract changes and lesion overlap.Results
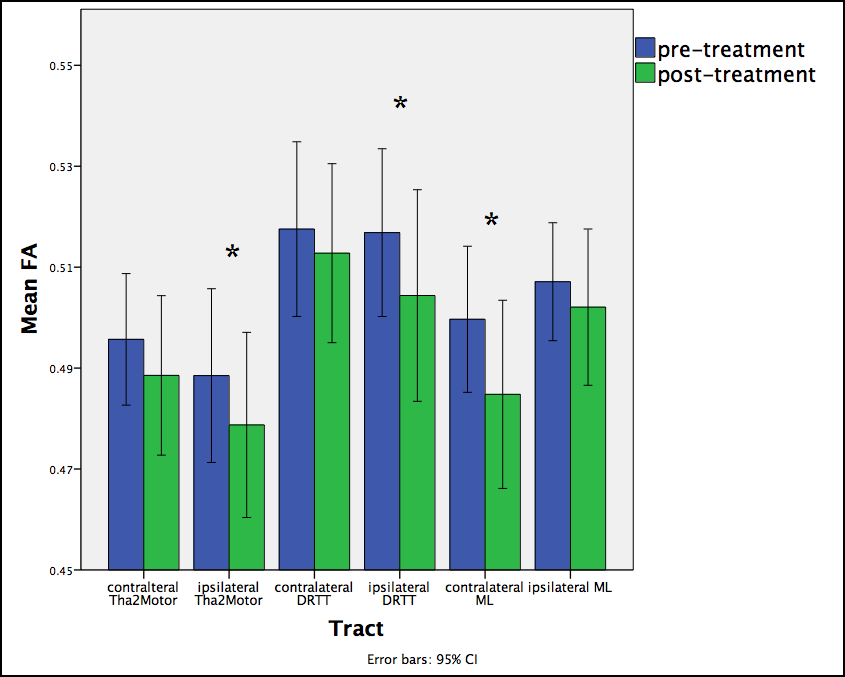
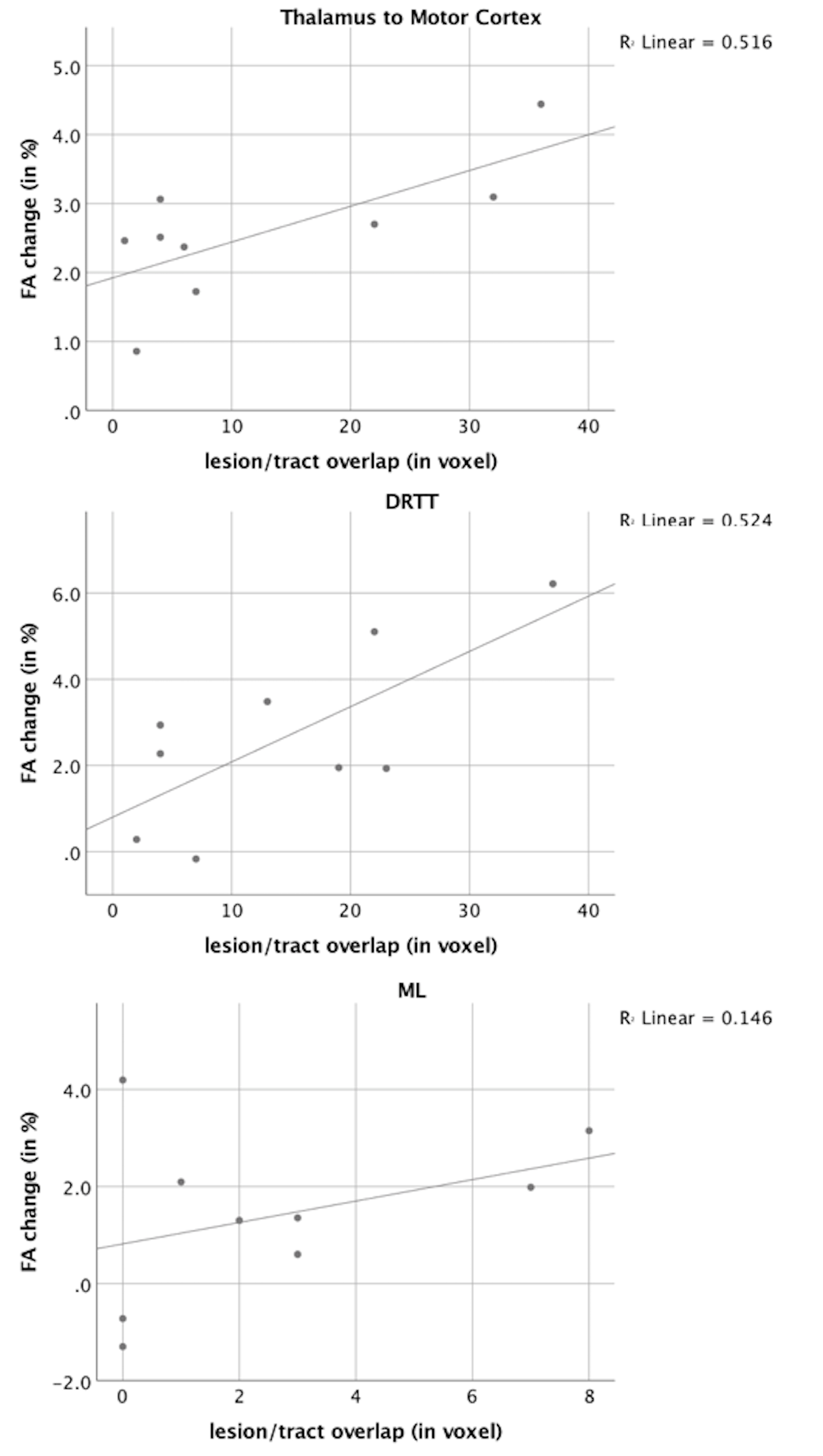
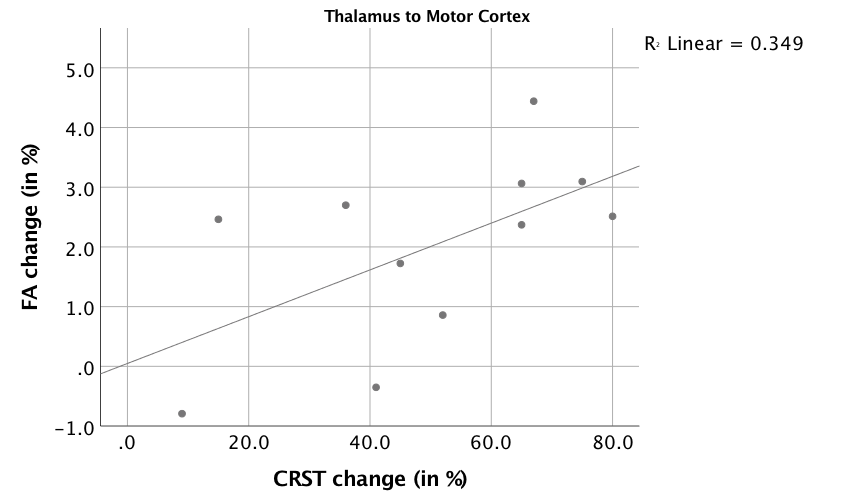
All patients experienced tremor suppression contralateral to the treated side with CRST scores (Part A and B for the dominant hand) improving significantly from 19.8 (± 4.0) at baseline to 9.8 (± 5.1) after 12 months (-50.5%; p<0.001). FA values in the lesional ROI decreased significantly from 0.457 (± 0.082) to 0.207 (± 0.042) (n=9, -63.5%, p<0.001). In two patients (5 and 10), no lesion could be detected at follow-up MRI. Significant changes in FA values were detected in the ipsilesional tracts projecting from the thalamus to the motor cortex (-2.0%; p=0.001), ipsilesional DRTT (-2.5%, p=0.001) and contralesional ML (-3.0%; p=0.002). An overview of all tracts is given in Figure 2. Further, our data demonstrates significant correlations for lesion/tract overlap and FA decrease in the corresponding tracts (p<0.05) (see Figure 3 and 4). Decreasing FA values in the ipsilesional tracts projecting from the thalamus to the motor cortex correlated with clinical improvement (R=0.59; p=0.03)(Figure 5) but no such correlation was found for the ipsilesional DRTT or ML (R=0.19, p=0.29; R=0.44, p=0.09).Discussion
Our data demonstrates significant tract changes of the ipsilesional tracts projecting between the thalamus and the motor cortex and DRTT after MRgHIFU, which are associated with lesion location. Decreasing FA values in the tracts projecting between the thalamus and the motor cortex were positively correlated with clinical improvement. These results support the findings of previous studies suggesting that the decrease in FA might represents degenerative processes of fibre tracts that are involved in the pathophysiology of essential tremor. [7] However, tract alterations were also detected in fibre tracts of the untreated side, possibly indicating a global impact on the brain connectivity network.Conclusion
DTI is a useful imaging biomarker to detect white matter tract changes in patients treated with MRgHIFU while diffusion tractography can improve lesion targeting in the thalamus.Acknowledgements
No acknowledgement found.References
- Elias WJ, Lipsman N, Ondo WG, et al. A randomized trial of focused ultrasound thalamotomy for essential tremor. N Engl J Med. 2016;375:730–739.
- Lipsman N, Schwartz ML, Huang Y, et al.MR-guided focused ultrasound thalamotomy for essential tremor: a proof-of-concept study. Lancet Neurol. 2013 May;12(5):462-8.
- Chazen JL, Sarva H, Stieg PE, et al. Clinical improvement associated with targeted interruption of the cerebellothalamic tract following MR-guided focused ultrasound for essential tremor. J Neurosurg. 2017 Oct 20:1-9.
- Fenoy AJ, Schiess MC. Deep Brain Stimulation of the Dentato-Rubro-Thalamic Tract: Outcomes of Direct Targeting for Tremor. Neuromodulation. 2017 Jul;20(5):429-436.
- Fahn S, Tolosa E, Marin C. Clinical rating scale for tremor. Parkinson’s disease and movement disorders. 1993;2:271-80.
- Jenkinson M, Beckmann CF, Behrens TEJ, Woolrich MW, Smith SM. FSL. NeuroImage. 2012;62(2):782-90.
- Wintermark M, Huss DS, Shah BB, et al. Thalamic connectivity in patients with essential tremor treated with MR imaging-guided focused ultrasound: in vivo fiber tracking by using diffusion-tensor MR imaging. Radiology. 2014 Jul;272(1):202-9.
Figures