3743
The Abnormal Cerebral Perfusion Profile in older adults with HIV-Associated Neurocognitive Disorder: Discriminative Power of Arterial Spin Labelling MRI1Department of Radiology and Biomedical Imaging, Zuckerberg San Francisco General Hospital, University of California San Francisco, San Francisco, CA, United States, 2Department of Neurology, University of California San Francisco, San Francisco, CA, United States, 3Division of Geriatric Medicine, University of California San Francisco, San Francisco, CA, United States
Synopsis
This study aimed at evaluating the pattern of cerebral blood flow (CBF) abnormalities in older adults with HIV-associated neurocognitive disorder (HAND) compared to cognitively healthy controls. Pulsed ASL (for CBF quantification) and T1-weighted images (for registration to cortical parcellation atlas) were collected in a retrospective cohort of 19 HIV+ participants and 15 age and education matched controls. To investigate differences in CBF patterns between HIV+ and controls, CBF values were used to train generalized linear models (GLMnet) to predict patient diagnosis. Older HIV+ exhibited lower CBF values in the temporal and occipital lobes compared to controls suggesting a specific pattern of CBF in individuals aging with HAND.
Introduction
Advances in combination antiretroviral treatment (cART) have transformed HIV from a fatal disease into a chronic, manageable condition. Despite these advances, people living with HIV can continue to develop signs and symptoms referable to the central nervous system, even despite perfect adherence to cART. 1–4 The prevalence of HIV-associated neurocognitive disorders (HAND) in the US is now estimated up to 50% of the HIV-infected population2,5,6. Brain gene expression profiles suggest neurovascular endothelial dysfunction may provide a link between HIV in the central nervous system and clinical abnormalities in HAND patients who are virally suppressed. 7 The purpose of this study was to evaluate the pattern of cerebral blood flow (CBF) abnormalities in HIV positive (HIV+) patients compared to cognitively healthy (CH) controls.Methods
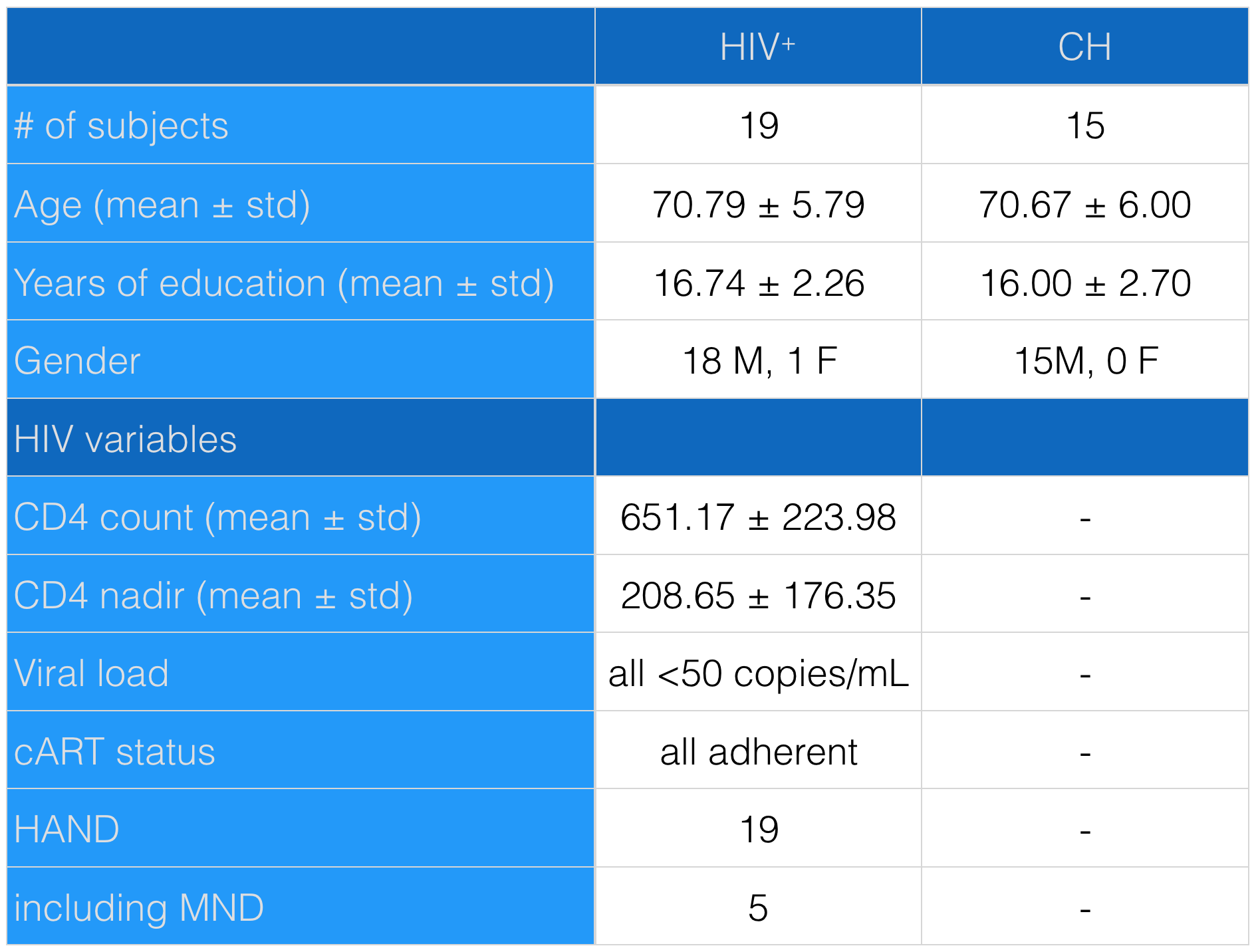
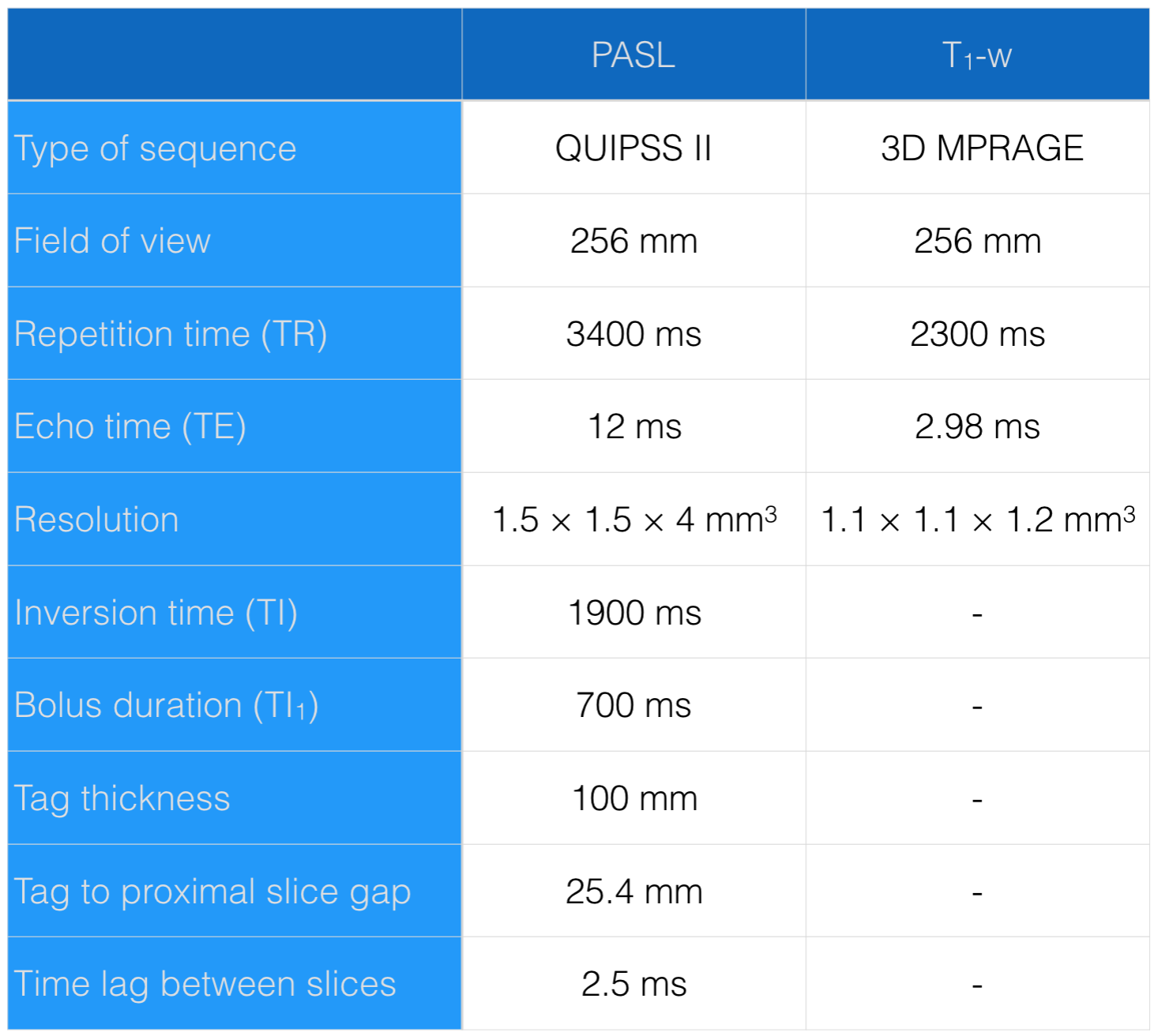
A retrospective cohort of 19 older HIV+ participants with HAND from the UCSF HIV Over 60 cohort. Fifteen age and education matched cognitively healthy (CH) controls from the Alzheimer’s Disease Neuroimaging Initiative cohort (ADNI-2) were selected (see demographics in Table 1). Pulsed arterial spin labeling (ASL)8 and anatomical T1-weighted (T1-w) images were acquired on a 3T Siemens Magnetom Skyra scanner using the parameters listed in Table 2. ASL images were motion corrected. Perfusion weighted images were computed by subtracting the mean-tagged and the mean-untagged ASL images. The first untagged ASL image was used as a proton density weighted reference image for computing CBF (in mL/100g x min) and subsequent co-registration of ASL and T1-w. This registration consisted in linear and non-linear transformations (using mutual information and total variance respectively). To reduce contrast differences, simulated T2-w derived from corresponding T1-w were used as intermediate maps in the coregistration process. Freesurfer was used to correct for partial volume effects and to generate anatomical region of interest (ROI). CBF values were standardized to the left post-central gyrus. A binomial generalized linear model (GLMnet, logistic elastic net regression)9 was trained to predict patient diagnosis based on CBF values by ROI, assuming that if such a model can successfully predicts diagnosis, the CBF pattern differs between HIV+ and CH. All predictors (CBF by ROI, age and education) were centered and scaled in the analysis. The stability of estimated parameters was ensured by bootstrap (500 iterations): at each iteration, the dataset was randomly split between train (60%) and test (40%), the GLMnet model was trained and cross-validated on the training set, and the predictors coefficients, accuracy, sensitivity and specificity of the model were registered. Odds ratios (OR) associated to the predictors were computed by exponentiating the corresponding model coefficient averaged over bootstrap. The predictors used by the GLMnet model in more than 25% of bootstrap iterations were considered to be significantly different between patients and CH.Results
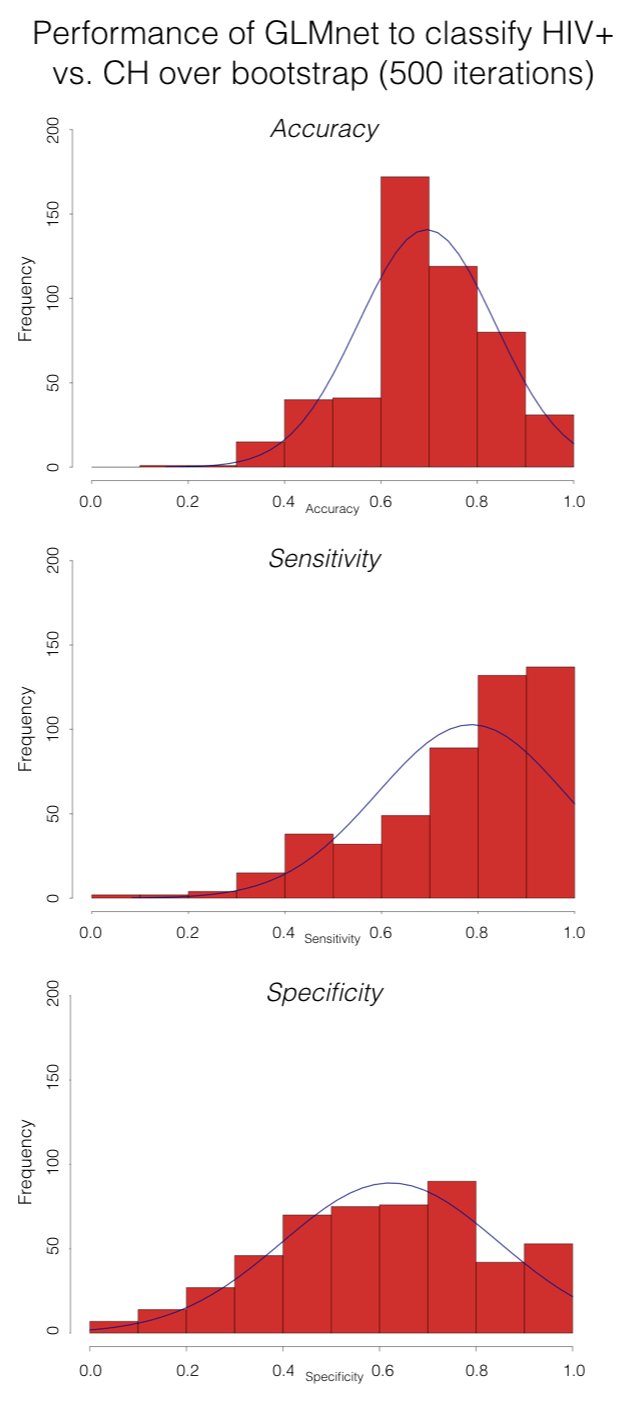
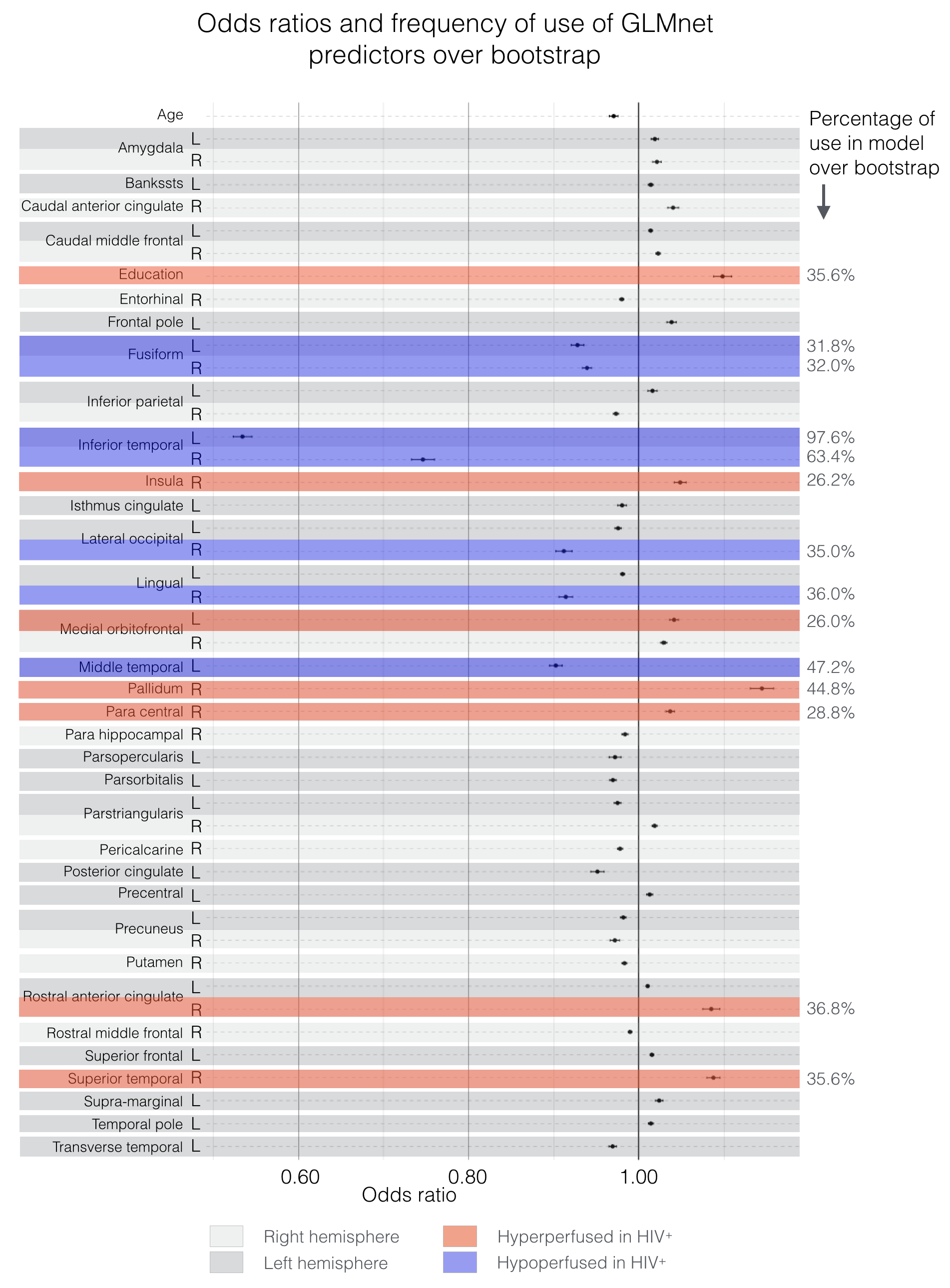
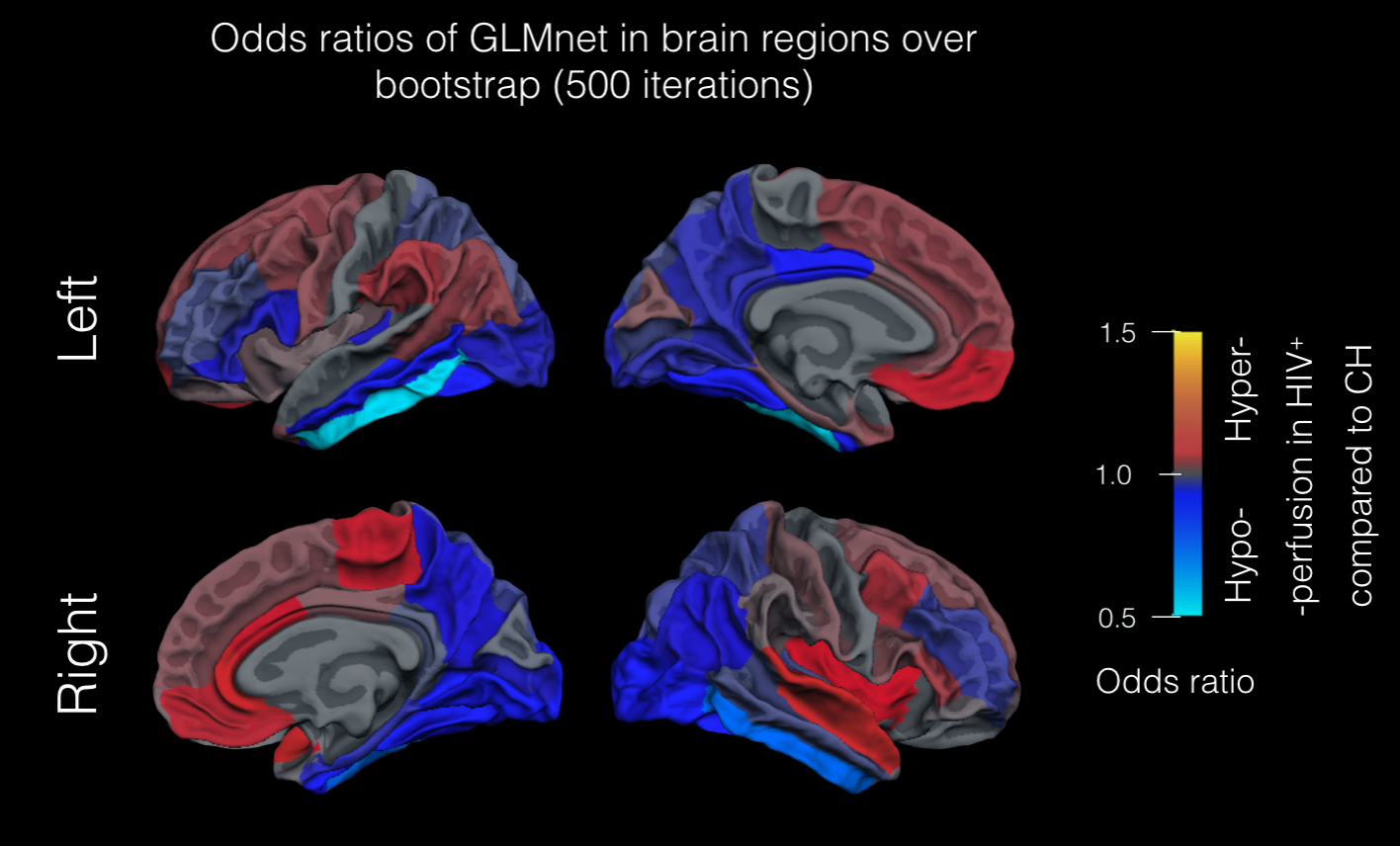
The GLMnet model yielded good accuracy (0.70±0.14), sensitivity (0.83±0.19) and reasonable specificity (0.62±0.22) over bootstrap, as shown in Figure 1. The interpretation of an OR>1 (or OR <1) is that an increase (or decrease) of CBF in the corresponding brain region resulted in an increase of likelihood of being classified as an HIV+ patient, meaning that the corresponding ROI was hyperperfused (or hypoperfused) in HIV+ patients compared to CH. The analysis (Figure 2) showed significant CBF differences between HIV+ and CH in 14 regions, with the inferior temporal gyrus exhibiting the greatest relative hypoperfusion in both hemispheres. HIV+ patients exhibited mild relative hyperperfusion in the medial frontal cortical regions and hypo-perfusion in the parieto-temporal, lateral frontal, and occipital lobes compared to CH (Figure 3).Discussion and conclusion
These results suggest a significant effect of HIV status on regional CBF compared to age and education matched controls. It implies that in an aging cohort, HIV+ patients with HAND demonstrate a unique CBF profile with relative hypoperfusion in the temporal and occipital lobes. The mechanisms for the observed changes in CBF within an ageing HAND population remains unknown. However, GM loss has previously been reported in the lateral temporal and occipital lobes10,11, possibly suggesting that hypoperfusion in HAND acts as a precursor of volume loss as it does in other neurodegenerative diseases12. Future work should aim to confirm this CBF profile in a larger cohort and control for confounding cerebrovascular diagnosis. If this unique CBF profile is confirmed, it may help to study the effects of HIV in the aging brain and distinguish HAND from other neurocognitive disorders. Additionally, the pathophysiology of CBF abnormalities in HAND warrants further investigations.Acknowledgements
This study was supported by the American foundation for AIDS research, and the UCSF Resource Allocation Program.References
1. Price, R. W. et al. Evolving character of chronic central nervous system HIV infection. Semin. Neurol. 34, 7–13 (2014).
2. Valcour, V., Sithinamsuwan, P., Letendre, S. & Ances, B. Pathogenesis of HIV in the central nervous system. Curr. HIV/AIDS Rep. 8, 54–61 (2011).
3. Valcour, V. et al. Central nervous system viral invasion and inflammation during acute HIV infection. J. Infect. Dis. 206, 275–282 (2012).
4. Hellmuth, J., Valcour, V. & Spudich, S. CNS reservoirs for HIV: implications for eradication. J Virus Erad 1, 67–71 (2015).
5. Hellmuth, J., Milanini, B. & Valcour, V. Interactions between ageing and NeuroAIDS. Curr. Opin. HIV AIDS 9, 527–532 (2014).
6. Chiao, S. et al. Deficits in self-awareness impact the diagnosis of asymptomatic neurocognitive impairment in HIV. AIDS Res. Hum. Retroviruses 29, 949–956 (2013).
7. Gelman, B. B. et al. The National NeuroAIDS Tissue Consortium brain gene array: two types of HIV-associated neurocognitive impairment. PLoS One 7, e46178 (2012).
8. Luh, W. M., Wong, E. C., Bandettini, P. A. & Hyde, J. S. QUIPSS II with thin-slice TI1 periodic saturation: a method for improving accuracy of quantitative perfusion imaging using pulsed arterial spin labeling. Magn. Reson. Med. 41, 1246–1254 (1999).
9. Friedman, J., Hastie, T. & Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 33, 1–22 (2010).
10. Becker, J. T. et al. Factors affecting brain structure in men with HIV disease in the post-HAART era. Neuroradiology 54, 113–121 (2012).
11. Küper, M. et al. Structural gray and white matter changes in patients with HIV. J. Neurol. 258, 1066–1075 (2011).
12. Sanford, R. et al. Regionally Specific Brain Volumetric and Cortical Thickness Changes in HIV-Infected Patients in the HAART Era. J. Acquir. Immune Defic. Syndr. 74, 563–570 (2017).
Figures