3742
Initial Experience of Cerebral Quantitative Susceptibility Mapping in the HIV Neurocognitive Disorder1Department of Radiology and Biomedical Imaging, Zuckerberg San Francisco General Hospital, University of California San Francisco, San Francisco, CA, United States, 2Surbeck Laboratory of Advanced Imaging, Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 3Graduate program in BIoengineering, University of California Berkeley and University of California San Francisco, San Francisco, CA, United States, 4Department of Neurology, Zuckerberg San Francisco General Hospital, University of California San Francisco, San Francisco, CA, United States
Synopsis
This study investigates the patterns of tissue susceptibility within brains of older HIV+ participants using quantitative susceptibility mapping (QSM) as marker of iron deposition in the brain. Four HIV+ participants and one healthy control were recruited, and QSM and T1w (for cortical parcellation) data were acquired on a 3T MRI scanner. Comparison of QSM values by brain region for each HIV+ participant with the control shows a pattern of increased susceptibility in frontal regions, especially in the frontal medial and subcallosal cortices. Although these results warrant further investigation in a larger cohort, this is the first study investigating changes in QSM in the HIV+ population.
Introduction
Despite numerous advances in combination antiretroviral treatments (cART), it is not currently possible to eradicate HIV reservoir from the brain1–3. Moreover, up to 50% of the HIV-infected population in the US suffer from HIV associated neurocognitive disorders (HAND) although its diagnosis is still challenging2,4,5. The physiopathology of HAND is relatively poorly understood but evidences suggest it is associated with microglial inflammation2. Although a few studies have reported higher levels of iron in the brain of HIV+ individuals6,7 especially within microglia, no study has taken advantage of quantitative susceptibility-weighted techniques. The purpose of this study is to investigate tissue susceptibility in the brain of HIV+ patients using quantitative susceptibility mapping (QSM)8 as a marker of iron deposition, which has been shown to be involved in several neurodegenerative diseases9.Methods
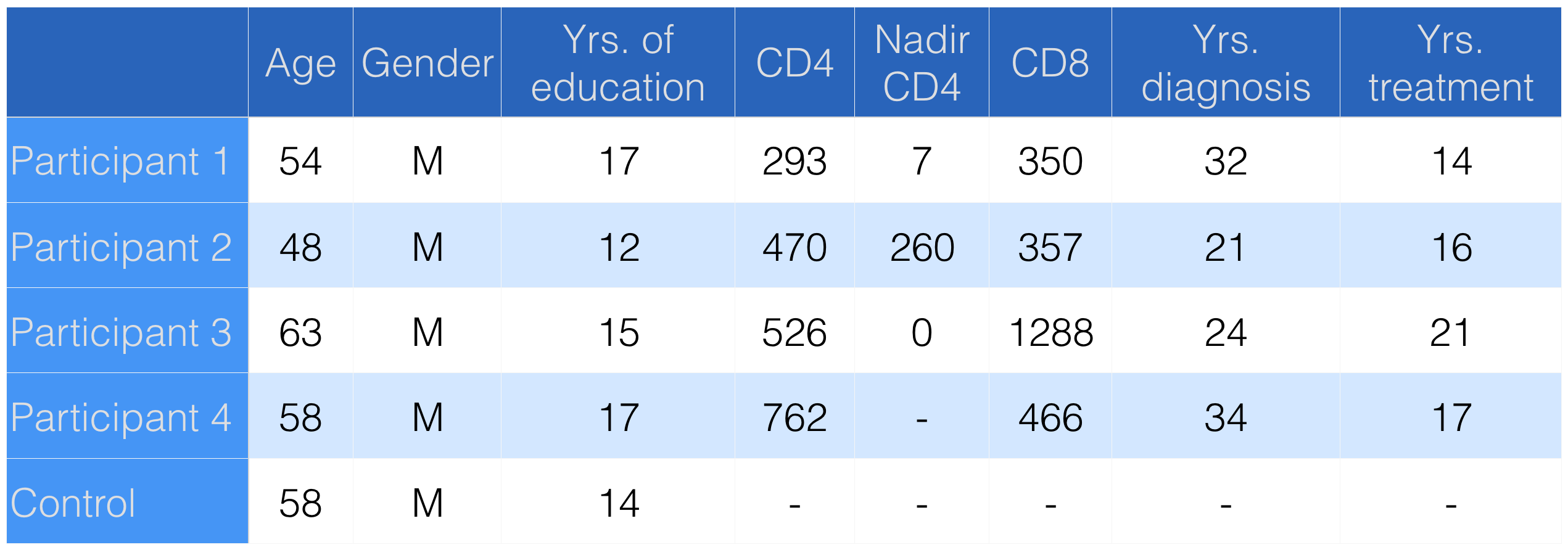
Four HIV positive (HIV+) participants and one healthy control (see Table 1) were recruited and scanned on a 3T MR GE Signa scanner. T1-weighted (T1-w) images were acquired using the following parameters: TR=6.7 ms, TE=2.1 ms, flip angle=12°, resolution=1x1x1mm3 and susceptibility weighted images were collected as complex MRI signals from each receiver channel during the same scan using the following parameters: TR=50.3 ms, TE=13 ms, flip angle=20°, bandwidth=244 Hz per pixel, resolution=0.47x0.47x1.5mm3. QSM images were reconstructed using a laplacian-based phase unwrapping, VSHARP10 for background removal and iLSQR11 for inversion problem solving. T1-w images were used for registration to the Harvard-Oxford cortical atlas using FSL12, and for subsequent parcellation of the QSM maps. The distribution of QSM values over ROIs were plotted for each subject (HIV+ participants and healthy control). The QSM values differences (HIV+ participant-control) were plotted for each HIV+ participant as a bar plot and projected onto a standard brain atlas (Harvard-Oxford cortical and subcortical structural atlas from FSL).Results
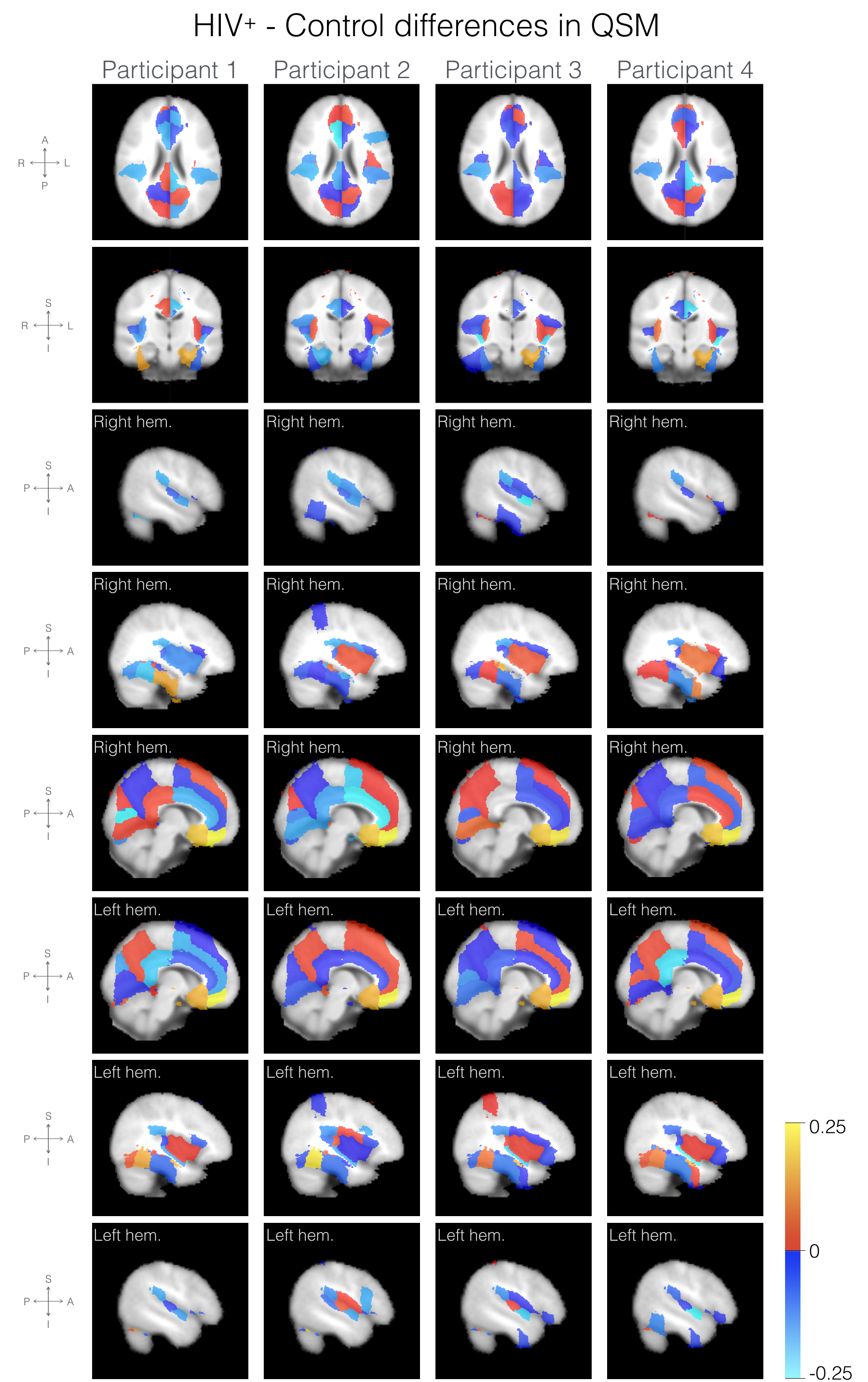
Distribution of the median QSM over ROIs (see Figure 1) were in similar range of values for the four HIV+ participants and control, with higher values in the basal ganglia as a reflection of the higher iron content present in this area13,14, although the patients distributions were less symmetrical for the left and right hemispheres than the control’s distribution. Comparison of QSM values by brain ROI (see Figure 2) showed higher QSM values in the frontal area (frontal medial cortex) and subcallosal cortex in all four HIV+ participants and in the parahippocampal gyrus in three HIV+ participants, compared to the control. The pattern of QSM differences between HIV+ participants and the control were similar across HIV+ participants, as shown in Figure 3. When compared to the control, HIV+ participants exhibited similar global hemispheric values, while higher QSM values in the frontal lobes specifically in the frontal medial, paracingulate, superior frontal and subcallosal cortices. In occipital and temporal regions, results were not consistent between the two groups.Discussion and conclusion
The present study showed altered QSM values in HIV+ participants compared to an age matched healthy control. QSM has been shown to correlate with iron content15–17. The iron content in the brain naturally increases with ageing18 but disrupted iron homeostasis and iron deposition has been shown in multiple sclerosis19 , Alzheimer's and Parkinson diseases20, and is linked with neuroinflammation21. In the HIV context, increased iron stores correlate with rapid HIV progression in AIDS patients22. In vivo CSF collection, postmortem neuropathology and in vivo MRI in HIV have demonstrated iron/ferritin deposition within the CSF associated with activated microglia/macrophages and alteration in T2* 6,7,23. Loss of frontal gray and white matter volume has also been a dominant feature of HIV+ imaging datasets24,25. Hence the results of the present study suggest a change in frontal brain iron content in the ageing HIV population, possibly linked to microglial mediated neuroinflammation. However, given the size of the studied cohort, these results warrant further confirmation in a larger group of participants and controls. Studying the iron deposition patterns in the contemporary HIV+ population may help reveal the pathophysiologic basis of cognitive decline in HAND. To the best of our knowledge, this is the first study investigating iron content through QSM in the HIV+ population.Acknowledgements
This study was supported by the American foundation for AIDS research, and the UCSF Resource Allocation Program.References
1. Price, R. W. et al. Evolving character of chronic central nervous system HIV infection. Semin. Neurol. 34, 7–13 (2014).
2. Valcour, V., Sithinamsuwan, P., Letendre, S. & Ances, B. Pathogenesis of HIV in the central nervous system. Curr. HIV/AIDS Rep. 8, 54–61 (2011).
3. Valcour, V. et al. Central nervous system viral invasion and inflammation during acute HIV infection. J. Infect. Dis. 206, 275–282 (2012).
4. Hellmuth, J., Milanini, B. & Valcour, V. Interactions between ageing and NeuroAIDS. Curr. Opin. HIV AIDS 9, 527–532 (2014).
5. Chiao, S. et al. Deficits in self-awareness impact the diagnosis of asymptomatic neurocognitive impairment in HIV. AIDS Res. Hum. Retroviruses 29, 949–956 (2013).
6. Yoshioka, M. et al. Simultaneous detection of ferritin and HIV-1 in reactive microglia. Acta Neuropathol. 84, 297–306 (1992).
7. Miszkiel, K. A. et al. The measurement of R2, R2∗ and R2′ in HIV-infected patients using the prime sequence as a measure of brain iron deposition. Magn. Reson. Imaging 15, 1113–1119 (1997).
8. Wang, Y. & Liu, T. Quantitative susceptibility mapping (QSM): Decoding MRI data for a tissue magnetic biomarker. Magn. Reson. Med. 73, 82–101 (2015).
9. Piñero, D. J. & Connor, J. R. Iron in the Brain: An Important Contributor in Normal and Diseased States. Neuroscientist 6, 435–453 (2000).
10. Wu, B., Li, W., Guidon, A. & Liu, C. Whole brain susceptibility mapping using compressed sensing. Magn. Reson. Med. 67, 137–147 (2012).
11. Li, W. et al. A method for estimating and removing streaking artifacts in quantitative susceptibility mapping. Neuroimage 108, 111–122 (2015).
12. Smith, S. M. et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage 23 Suppl 1, S208–19 (2004).
13. Morris, C. M., Candy, J. M., Oakley, A. E., Bloxham, C. A. & Edwardson, J. A. Histochemical distribution of non-haem iron in the human brain. Acta Anat. 144, 235–257 (1992).
14. Haacke, E. M. et al. Imaging iron stores in the brain using magnetic resonance imaging. Magn. Reson. Imaging 23, 1–25 (2005).
15. Bilgic, B., Pfefferbaum, A., Rohlfing, T., Sullivan, E. V. & Adalsteinsson, E. MRI estimates of brain iron concentration in normal aging using quantitative susceptibility mapping. Neuroimage 59, 2625–2635 (2012).
16. Poynton, C. B. et al. Quantitative susceptibility mapping by inversion of a perturbation field model: correlation with brain iron in normal aging. IEEE Trans. Med. Imaging 34, 339–353 (2015).
17. Langkammer, C. et al. Quantitative susceptibility mapping (QSM) as a means to measure brain iron? A post mortem validation study. Neuroimage 62, 1593–1599 (2012).
18. Acosta-Cabronero, J., Betts, M. J., Cardenas-Blanco, A., Yang, S. & Nestor, P. J. In Vivo MRI Mapping of Brain Iron Deposition across the Adult Lifespan. J. Neurosci. 36, 364–374 (2016).
19. Wisnieff, C. et al. Quantitative susceptibility mapping (QSM) of white matter multiple sclerosis lesions: Interpreting positive susceptibility and the presence of iron. Magn. Reson. Med. 74, 564–570 (2015).
20. Berg, D. & Youdim, M. B. H. Role of iron in neurodegenerative disorders. Top. Magn. Reson. Imaging 17, 5–17 (2006).
21. Gerlach, M., Ben-Shachar, D., Riederer, P. & Youdim, M. B. Altered brain metabolism of iron as a cause of neurodegenerative diseases? J. Neurochem. 63, 793–807 (1994).
22. McDermid, J. M. et al. Elevated iron status strongly predicts mortality in West African adults with HIV infection. J. Acquir. Immune Defic. Syndr. 46, 498–507 (2007).
23. Granziera, C. et al. Micro-structural brain alterations in aviremic HIV+ patients with minor neurocognitive disorders: a multi-contrast study at high field. PLoS One 8, e72547 (2013).
24. Nir, T. M. et al. Mapping white matter integrity in elderly people with HIV. Hum. Brain Mapp. 35, 975–992 (2014).
25. Ances, B. M. & Hammoud, D. A. Neuroimaging of Hiv-associated neurocognitive disorders (hand). Curr. Opin. HIV AIDS 9, 545–551 (2014).
Figures