3681
Radial MS-CAIPIRINHA Efficiently Extends the Anatomical Coverage in MR Myocardial Perfusion Studies on MR-PET Systems1Department of Diagnostic and Interventional Radiology, University Hospital Würzburg, Würzburg, Germany, 2Comprehensive Heart Failure Centre, University Hospital Würzburg, Würzburg, Germany, 3Department of Nuclear Medicine, Klinikum rechts der Isar der Technischen Universität München, München, Germany, 4The Centre for Advanced Imaging, The University of Queensland, Brisbane, Germany, 5Magnetic Resonance, Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
Integrated MR-PET imaging is a versatile tool for the non-invasive characterization of cardiovascular disease. In this work, we developed an MS-CAIPIRINHA-based imaging technique to extend the anatomical coverage of the MRI perfusion assessment to six slices per RR. As a proof of principle, the described approach was combined with simultaneous 18F-FDG viability imaging and Late Gadolinium Enhancement (LGE) imaging investigating improvements in anatomical coverage for a relevant patient cohort.
Target audience
Clinicians interested in cardiac perfusion and
MR physicists interested in using MS-CAIPIRINHA.Purpose
MR-PET is a powerful imaging modality for the non-invasive characterization of cardiovascular diseases [1]. While for PET the assessment of myocardial perfusion and viability is inherently three-dimensional, conventional MRI perfusion techniques typically yield only three short-axis slices with high temporal resolution. An extension of left-ventricular coverage for MRI-based perfusion assessment is desirable especially when comparing functional and metabolic information as enabled by integrated MR-PET imaging.The aim of this study was to develop an MS-CAIPIRINHA-based imaging technique which extends the anatomical coverage of the MRI perfusion assessment to six slices per RR. As a proof of principle, it is combined with simultaneous 18F-FDG viability imaging and Late Gadolinium Enhancement (LGE) in order to investigate improvements over conventional perfusion imaging in the characterization of viability defects in a relevant patient cohort.
Methods
An ECG-gated TurboFLASH prototype similar to [2] was implemented
on a whole-body MR-PET system (Biograph mMR, Siemens Healthcare, Erlangen,
Germany). The pulse sequence featured a dual-band pulse to excite two slices simultaneously,
while the RF phase of the second slice was toggled between 0° and 180°. Within each RR-interval, three saturation
recovery (SR)-prepared acquisition blocks consisting of 52 radial projections
were acquired. A model-based algorithm, which is both enforcing the sensitivity
profiles of the utilized coil array and the sparsity in the spatial wavelet-domain
was then applied to reconstruct the undersampled datasets:
$$ \min_{I_{sl}} \; \biggl\Vert \biggl(\sum_{sl=1}^2 \Phi_{sl} \, E_{sl} \ I_{sl} \biggr)-y \, \biggr\Vert_2^2 + \lambda \sum_{sl=1}^2 \Vert \Psi I_{sl} \Vert_1 $$
$$$y$$$ represents the measured k-t-space multi-coil data
for one of the three dual-slice acquisition.
$$$I_{sl}$$$ corresponds to the temporal image series for
one of the two slices sl.
$$$E_{sl}$$$ is the encoding operator, which incorporates an
inverse Fourier transform, the re-gridding back to the initial radial projections,
and the superposition of the coil sensitivities to obtain multi-coil data. The
coil sensitivities for each slice were
determined by a fully sampled pre-scan under breathhold prior to contrast agent
injection.
$$$\Phi_{sl}$$$ performs the applied CAIPIRINHA phase
modulation, and
$$$\Psi$$$ transforms each frame of the image series into
the spatial wavelet domain.
$$$\lambda$$$ balances the weighting of the sparsity and the
data consistency term and was chosen empirically. A projection onto convex sets
(POCS) implementation in MATLAB (MathWorks, Natick, MA, USA) was used to
perform the optimization on an Intel Core i7-3820 CPU @ 3.60 GHz.
Typical imaging parameters were: Slice distance
between adjacent slices = 2 mm, slice distance between simultaneously acquired
slices = 30 mm, TE = 1.03 ms, TR = 1.33 ms, flip angle = 10°, slice thickness =
8 mm, in-plane resolution = 2.04 × 2.04 mm², 52 radial projections per image
pair, image matrix = 160 × 160, Rtotal ≈ 5.
The described MS-CAIPIRINHA approach was tested
against a conventional 3-slice SR-FLASH perfusion sequence with Cartesian
k-space ordering and similar sequence parameters as described above [3]. Conventional
and MS-CAIPIRINHA perfusion images were acquired separately for 60-90 RR
intervals during the same patient scan using two identical bolus injections 0.05 mM/kg Gd-DTPA.
LGE images were acquired across
the whole LV myocardium after a cumulative dose of 0.2 mM/kg Gd-DTPA and 15 min
equilibration time.
MR imaging was performed in five patients with
collateralized coronary total occlusions (CTO) in combination with a
simultaneous 18F-FDG viability scan after metabolic preparation by
insulin-clamping. List-mode PET data were acquired for 45 min starting 60 min
after injection of 18F-FDG.
Results
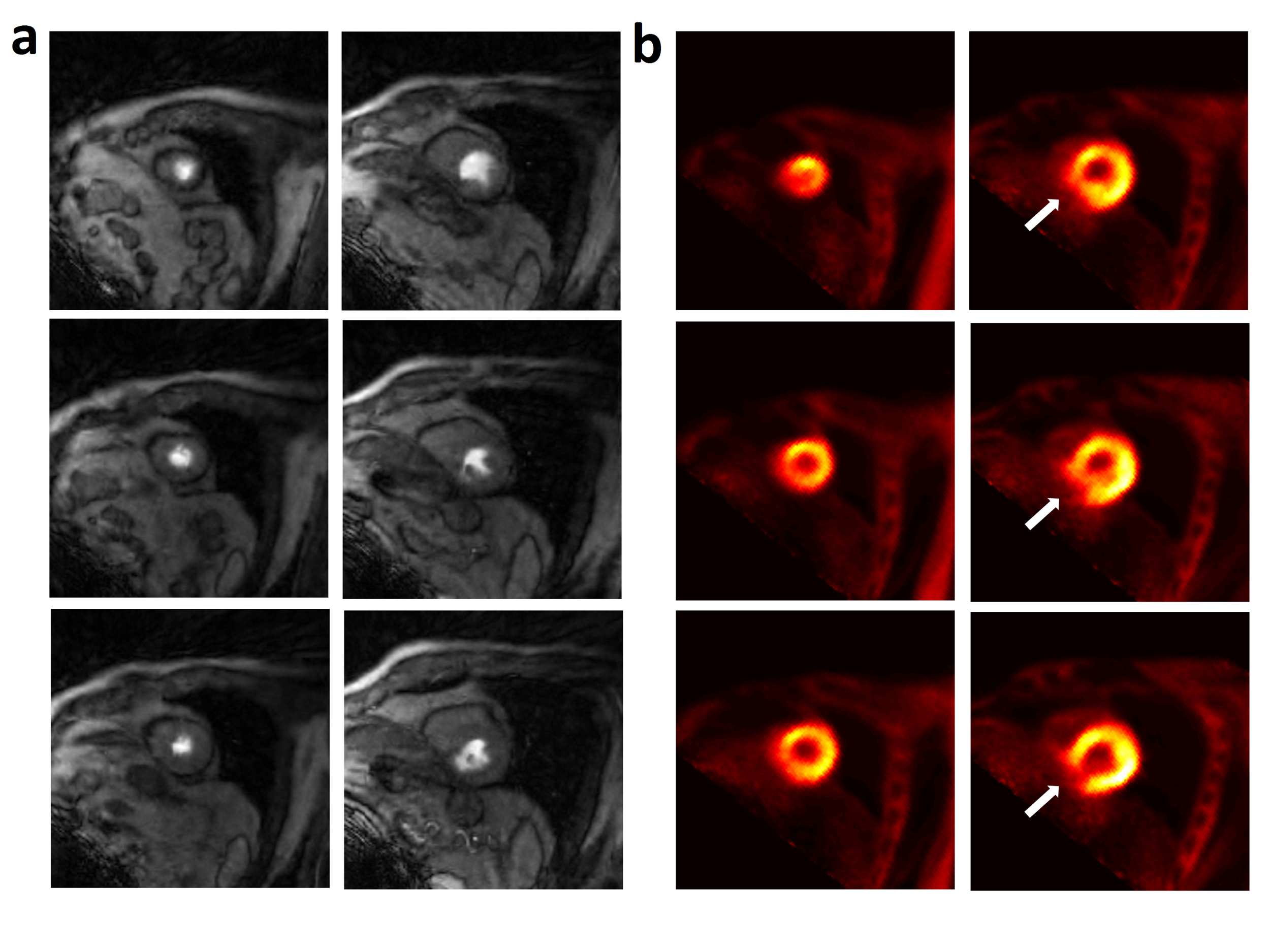
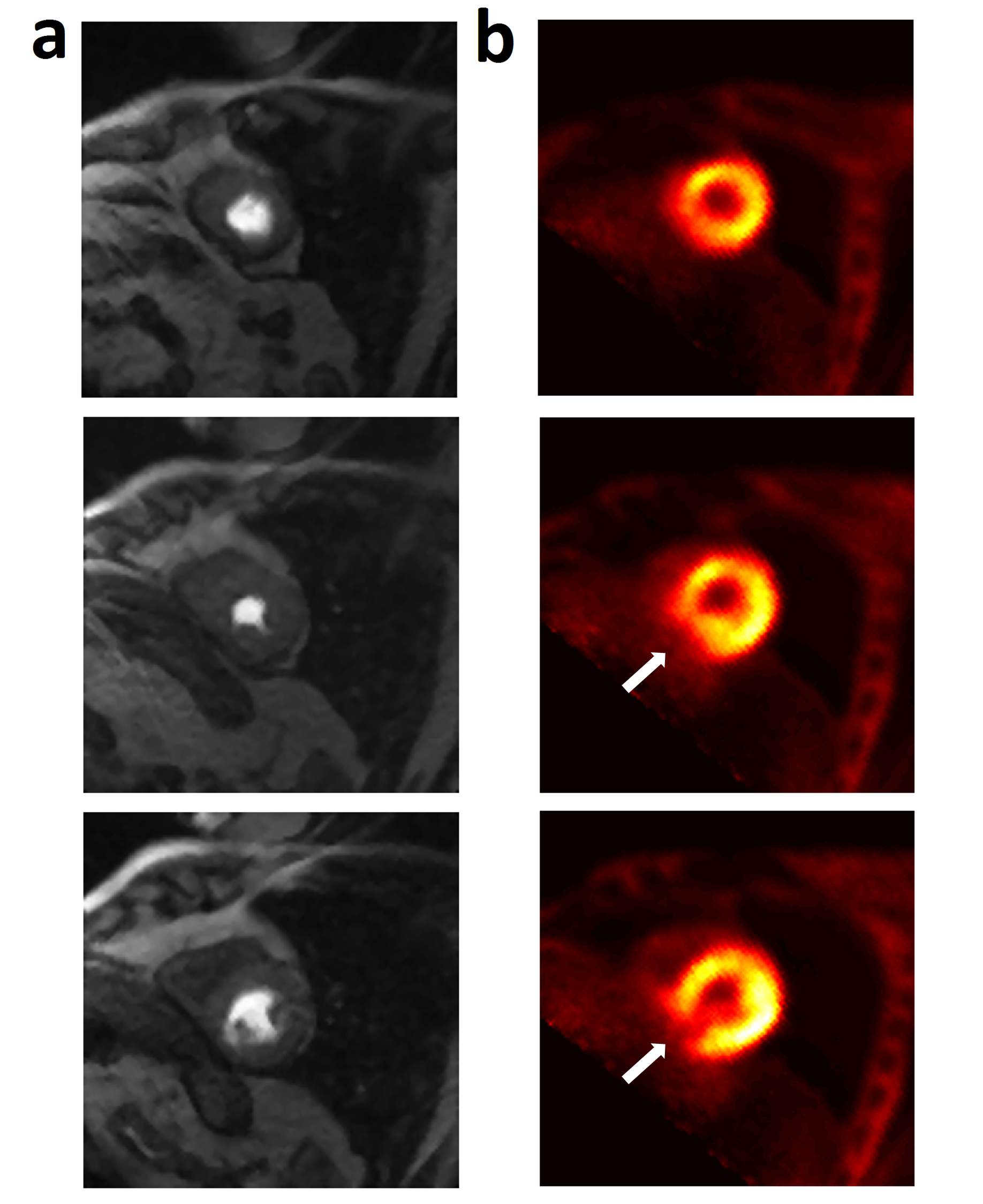
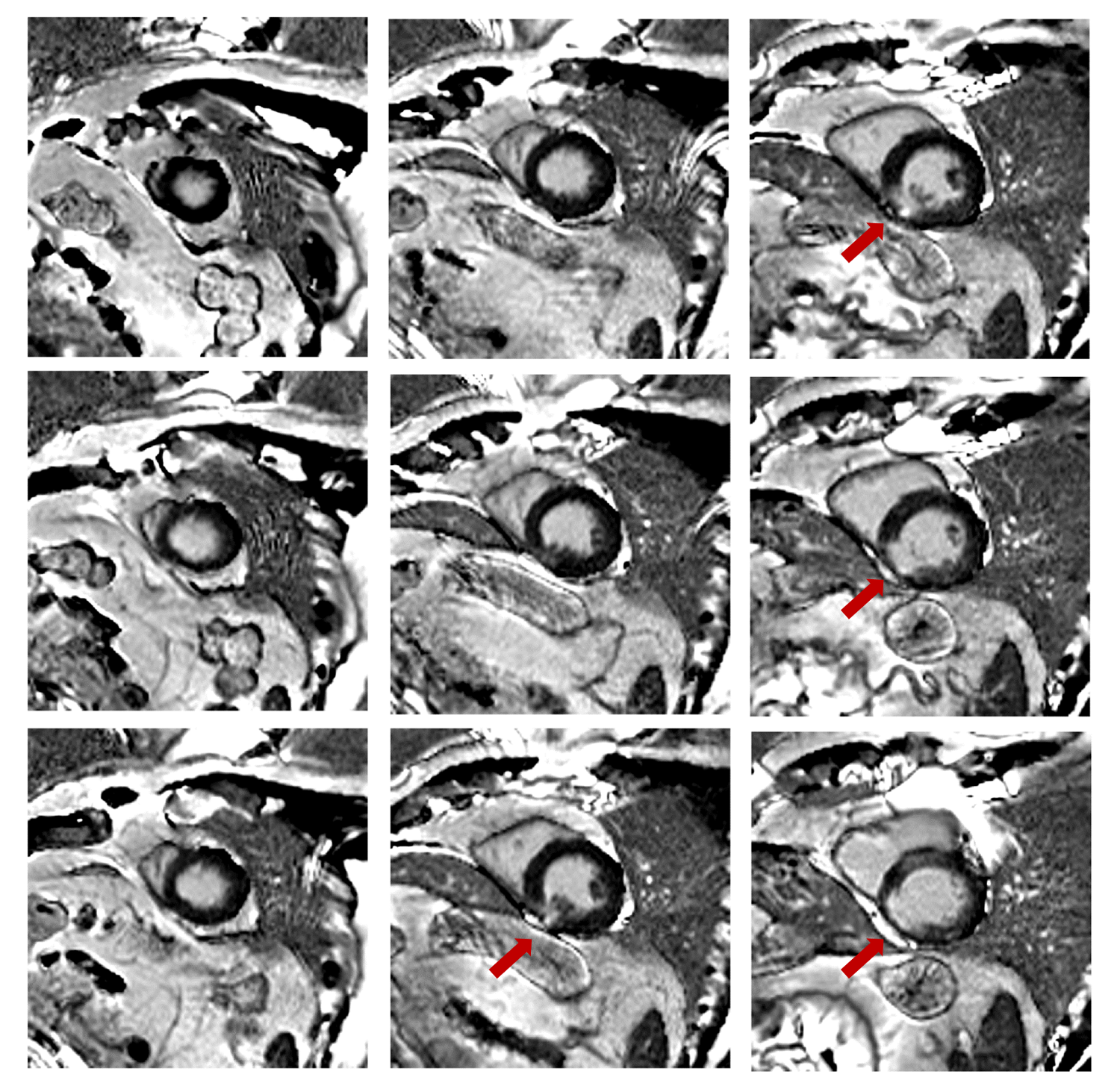
Images from 18F-FDG and both perfusion series were fused to the same short-axis slice positions and compared visually with respect to LV coverage and relation to the extent of viability defects. LGE and PET data covering the whole LV myocardium were used as references for defect size; an example of a patient exhibiting a medium-sized defect is shown in Figs. 1-3. The described MS-CAIPIRINHA approach was generally better able to characterize perfusion across areas of decreased tissue vitality as indicated by 18F-FDG uptake (Fig. 1). LV coverage was almost equivalent to LGE imaging and therefore better comparable to 3D PET results, while conventional perfusion images acquired from only three slice positions were often missing significant parts of the viability defect (Fig. 2).Discussion & Conclusion
The results of our study demonstrate that the proposed MS-CAIPIRINHA technique is a valuable means to extend the anatomical coverage for myocardial perfusion studies. This may be especially relevant for integrated MR-PET systems, where making use of the full potential of combining three-dimensional molecular PET information with simultaneously acquired dynamic MRI requires adequate coverage on the MRI-side.Acknowledgements
Funding: DFG (KO 2938/4-1)References
[1] Schwaiger et al., JNC 24(3): 1019–31 (2017) [2] Stäb et al., ISMRM 2015 #2686 [3] Kunze MRM 77:2320-2330 (2017)Figures