3638
Differential diagnosis in Parkinsonism using diffusion tensor as measured from multiple cortical regions1Medical Imaging and Radiological Science, Chang Gung University, Taoyuan, Taiwan, 2Medical Imaging and Radiological Sciences, Chang Gung University, Taoyuan, Taiwan, 3Neurology, Chang Gung Memorial Hospital, Taoyuan, Taiwan, 4Diagnostic Radiology, Keelung Chang Gung Memorial Hospital, Keelung, Taiwan, 5Diagnostic Radiology, Chang Gung Memorial Hospital, Taoyuan, Taiwan, 6University of Electronic Sciencee and Technology of China, School of Electronic Engineering, Chengdu, China
Synopsis
Parkinsonism is a long-term degenerative disorder of the central nervous system that mainly affects the motor system. The cortical parcellation algorithm was applied to evaluate the cortical involvement in the patients with PD by using diffusion tensor image. The fractional anisotropy is feasible in the brain of patients with Parkinsonism. Therefore fractional anisotropy could be a potential image based biomarker for monitoring Parkinson progression.
Introduction
Parkinsonism is major movement disorders which included at least the following syndromes: Parkinson disease (PD), progressive supranuclear palsy (PSP) and multiple system atrophy (MSA). Diffusion tensor imaging (DTI) has been shown sensitive to the changes in the brain of patients with PD (1). Significant decrease in the Fractional Anisotropy (FA) can be noticed in regions located in the nigral-striatal loop. Studies on MSA also reported reduced FA in the cerebellum (2). We therefore hypothesized that the involvement of different parts of the brain might be useful in the differential diagnosis of Parkinsonism. The current study aimed to evaluate the diagnostic performance of DTI on Parkinson disease, multiple system atrophy, progressive supranuclear palsy, and normal subjects (NC) by using a multivariate analysis.Materials and Methods
The study was approved by the Institutional Review Board, and complied with the Declaration of Helsinki. Diffusion Weighted Imaging (DWI) with the whole brain coverage were acquired from 274 PD patients (aged 59.9 ± 9.3year old), 50 MSA patients (aged 62.5 ± 6.9 year old), 357 PSP patients(aged 65.3 ± 6.2 year old), and 210 NC subjects (aged 62.4 ± 8.3year old) by using a 3T scanner (Trio, Magnetom, Siemens, Erlangen Germany). The imaging parameters included TR/TE = 5700 ms/108 ms; voxel size=2*2*2 mm, b=0 and 1000 s/mm2; 30 directions). The procedure of image processing followed Lu et al (ref). Fractional Anisotropy (FA) and Mean/Axial/Radial Diffusivity (MD/AD/RD) were calculated from the diffusion tensor, which were parcellated into 116 region of interest based on the Automatic Anatomic Labeling template. From each region of interest, the median, mean, 10th and 90th percentiles of each diffusion index were extracted. Discriminant Functional Analysis was used to determine the best model of discriminant formula. All statistical analyses is performed By PASW statistics 21 (IBM SPSS Staistics. Armonk, NY).Results
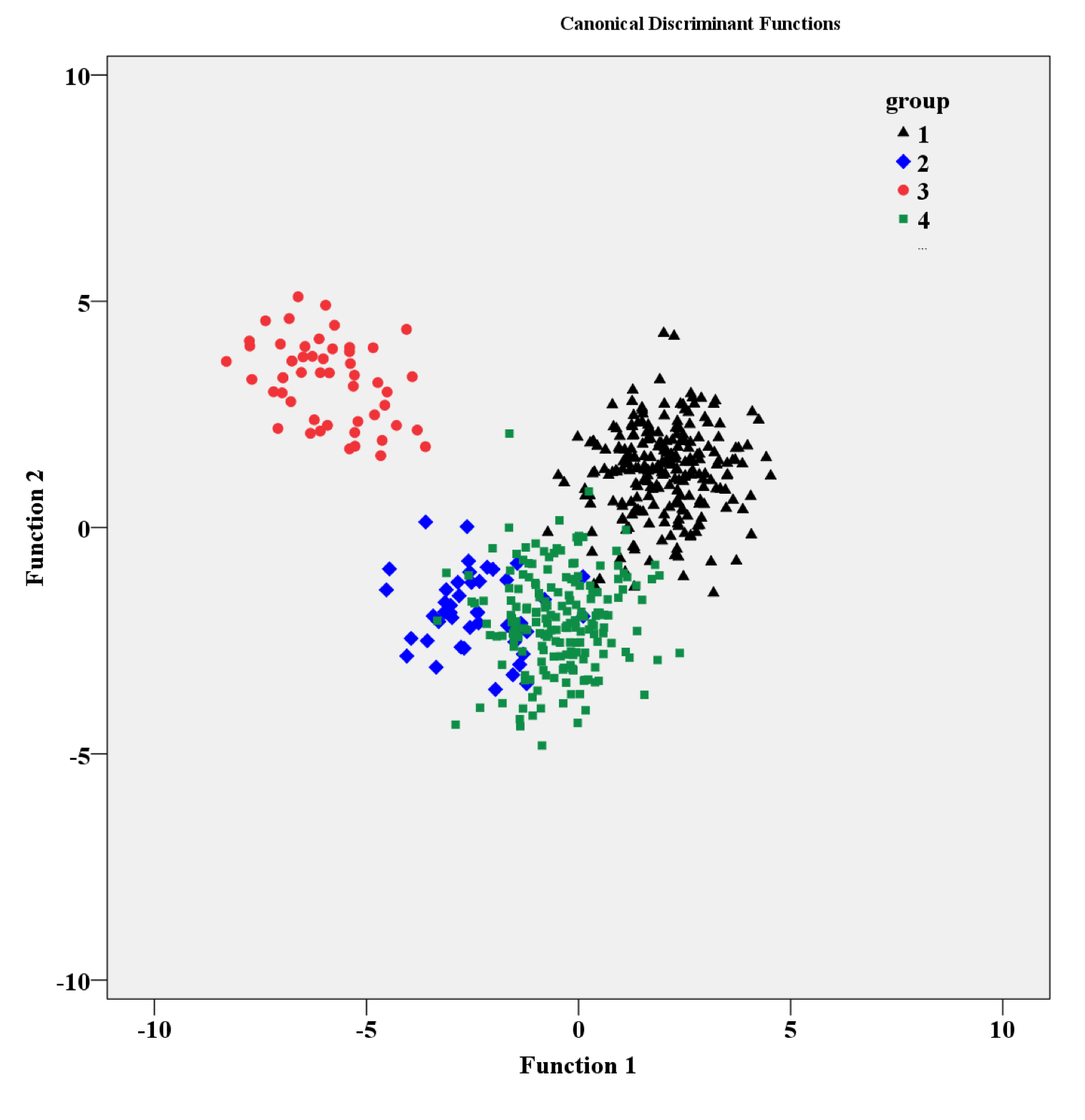
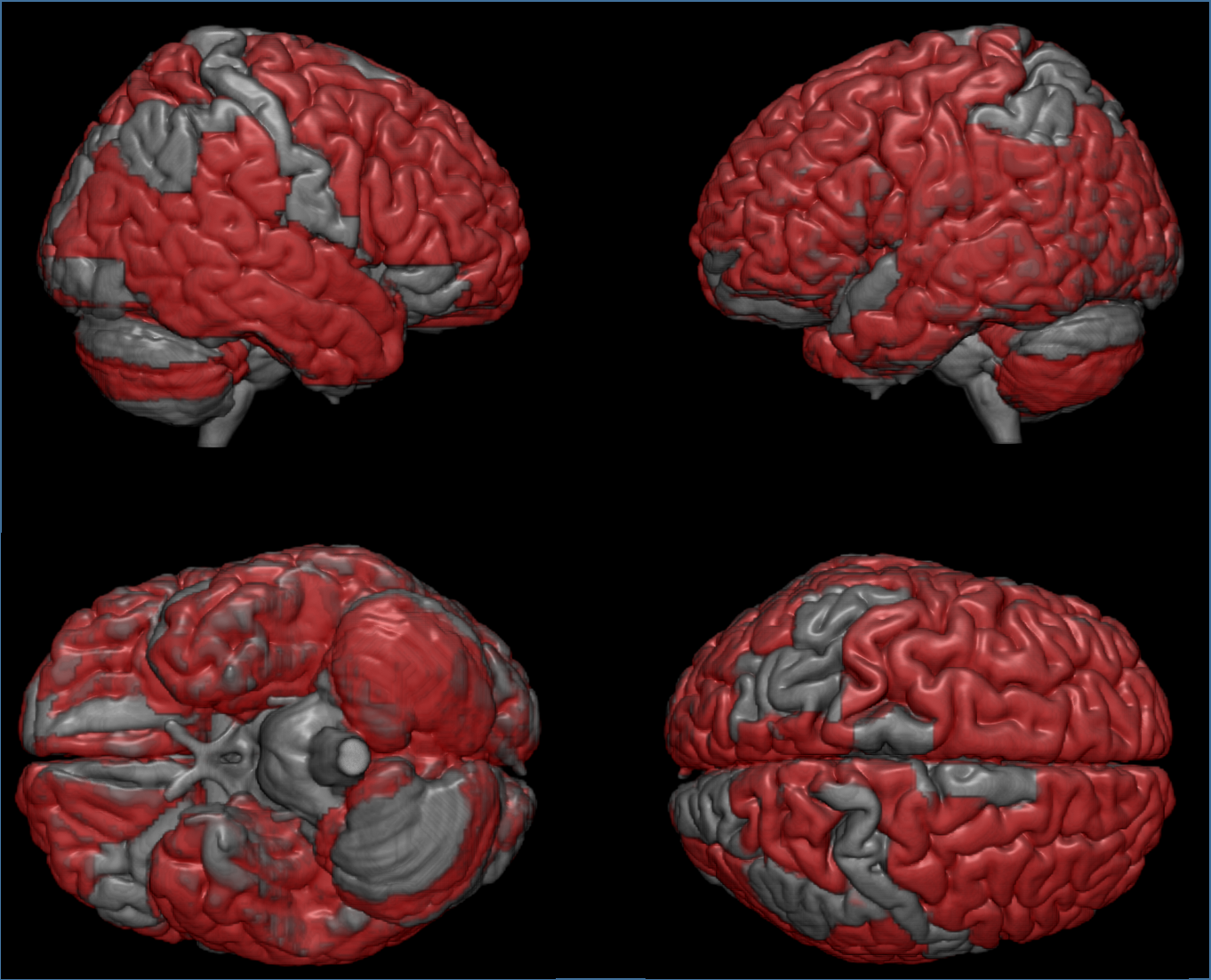
The classification accuracy with leave-one-out cross validation for patients with PD, MSA, PSP and NC is 91.5%, 86.7%, 94.2% and 90.5%, respectively (Figure1). In total, 98.5% of the participants were correctly classified. Figure 2 showed the identified brain regions from which the extract values of diffusion indices were selected into the discriminant model. The affected regions were mainly located in cerebellum, anterior corpus callosum, frontal and parietal white matter and thalamus.Discussion and Conclusion
The diagnosis of the Parkinsonism disease remained clinical. The current study provided objective evidence that could distinguish patients with different types of Parkinsonism disorders with good accuracy. Because diffusion tensor imaging is often part of the brain imaging that is prescribed to rule out the concomitant neurological diseases, the result might significantly increase the diagnostic confidence of the neurologists. Acknowledgements
No acknowledgement found.References
1. Yoshikawa K, Nakata Y, Yamada K, Nakagawa M. Early pathological changes in the parkinsonian brain demonstrated by diffusion tensor MRI. J Neurol Neurosurg Psychiatry. 2004;75(3):481-4.
2. Nilsson C, Markenroth Bloch K, Brockstedt S, Latt J, Widner H, Larsson EM. Tracking the neurodegeneration of parkinsonian disorders--a pilot study. Neuroradiology. 2007;49(2):111-9.
Figures