3609
Pre-operative DTI of white matter tracts in patients with idiopathic normal pressure hydrocephalus (iNPH) correlates with changes in clinical findings after shunt surgery1Radiology, Clinical Sciences, Uppsala, Sweden, 2Pharmacology and Clinical Neuroscience, Neurology, Östersund, Sweden, 3Neuroscience, Neurology, Uppsala, Sweden
Synopsis
Preoperative prediction of shunt surgery outcome is difficult. A test to predict outcome is missing. The use of diffusion tensor imaging (DTI) as a bioimaging marker was investigated. DTI parameters in white matter tracts were compared between patients and healthy controls, and also correlated with changes in clinical findings after shunt surgery. Significantly differences between healthy controls and patients were found. Correlations were found between preoperative DTI results and changes in clinical findings after shunt surgery, suggesting DTI to be a supportive tool for prediction of clinical outcomes from shunt surgery in patients with idiopathic normal pressure hydrocephalus (iNPH).
Introduction
The symptoms of idiopathic normal pressure hydrocephalus (iNPH) can be improved by shunt surgery, but preoperative prediction of treatment outcome is difficult. A test to predict the outcome after shunt surgery in iNPH is missing and a biomarker, correlating with clinical symptoms, would be valuable. If coupling between diffusion tensor imaging (DTI) and changes in clinical symptoms postoperatively could be found, DTI might give valuable contribution to the preoperative evaluation of these patients.Methods
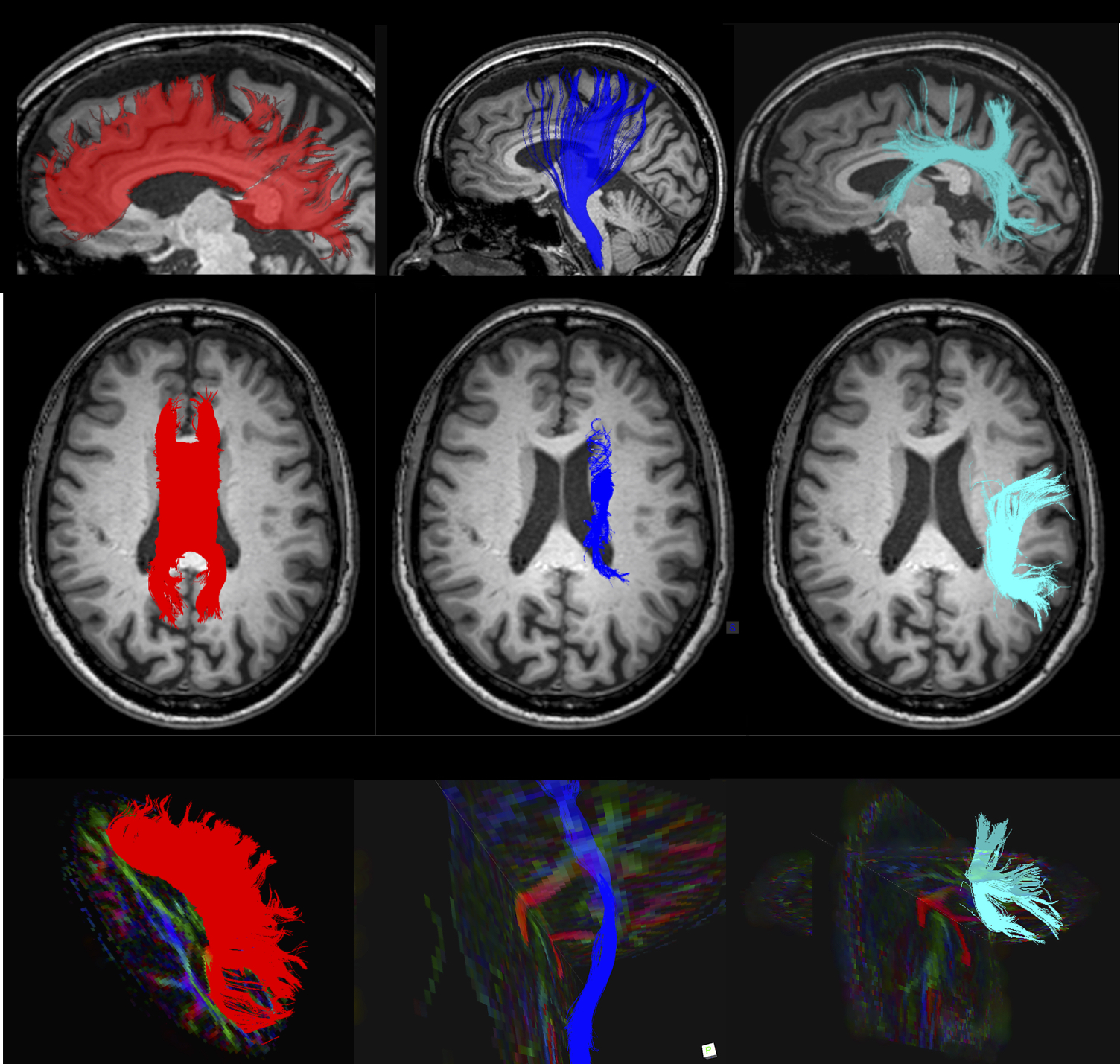
DTI parameters in white matter tracts in the vicinity of the dilated ventricles were analyzed and investigated together with clinical findings of the patients (fig 1). Twelve iNPH patients and twelve paired healthy controls, matched by age and gender, were included. Clinical examination, and morphological and diffusion MRI of the brain, were performed at inclusion and repeated immediately preoperatively as well as three months after shunt insertion. Healthy controls were only investigated at baseline. Tractography was used to evaluate the corpus callosum (CC), the corticospinal tract (CST), and the superior longitudinal fasciculus (SLF). Quantitative gait test, the cognitive test mini mental state examination (MMSE), and clinical assessment were performed. DTI results were compared before and after shunt surgery, and also between patients and healthy controls. Preoperative DTI results were tested for correlations with preoperative clinical findings and with changes in clinical findings after shunt surgery.
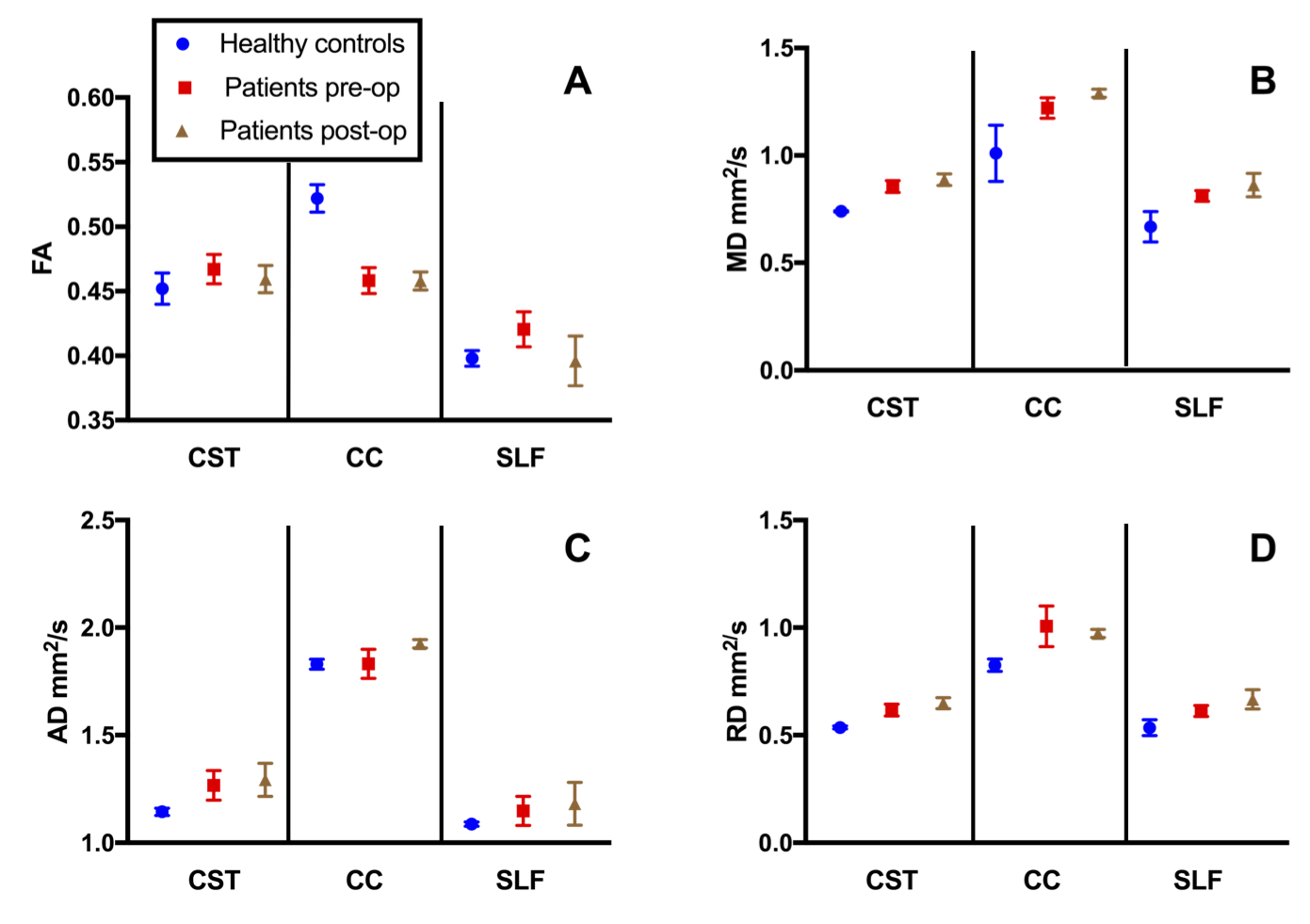
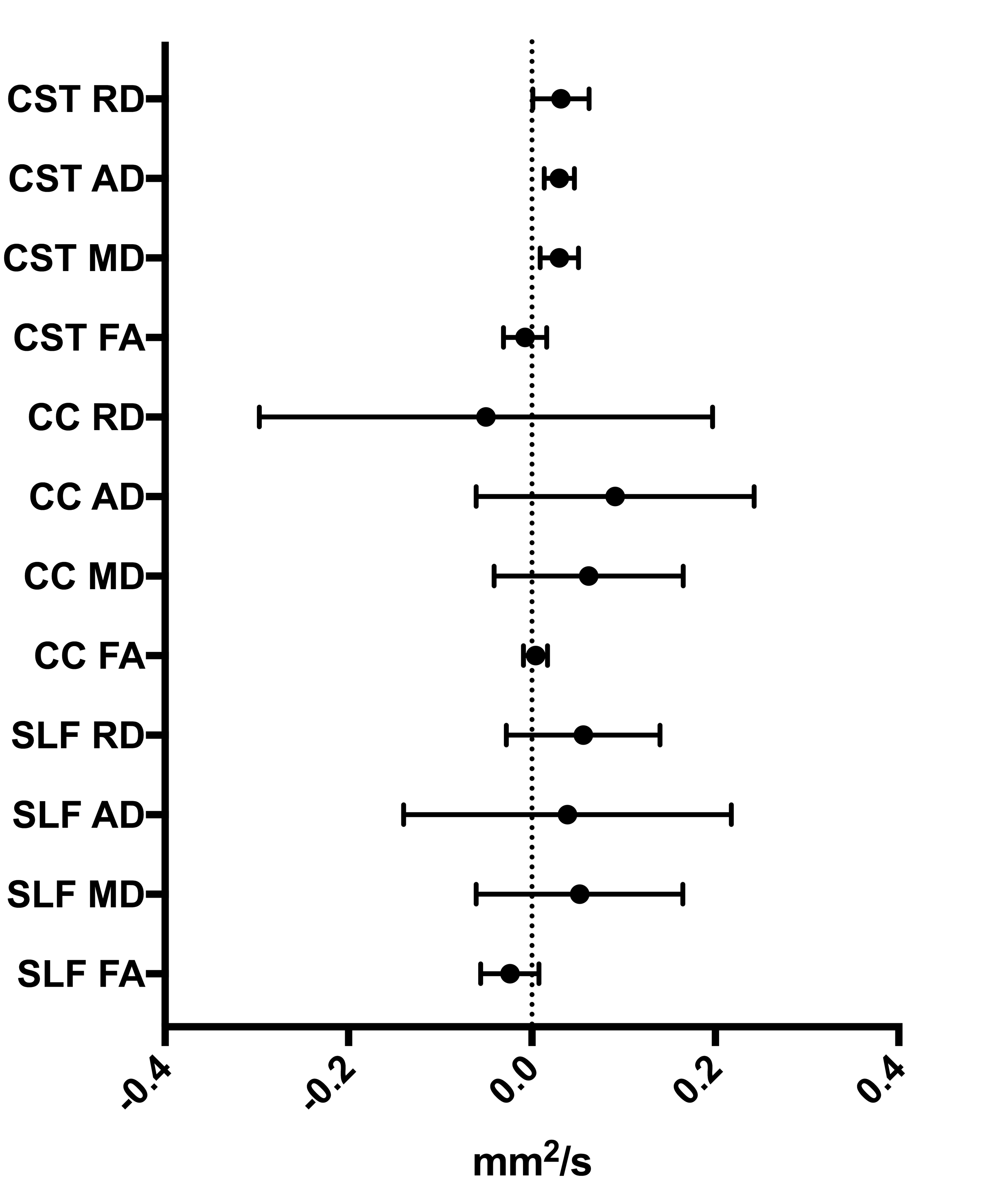
The presence of white matter lesions was quantified by scoring T2 weighted images using the Fazekas scale.1 An analysis including fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), and radial diffusivity (RD) was performed of CC, CSF, and SLF, and compared group-wise within the patients before and after shunt surgery, and measures of the matched healthy controls were used as reference (fig 2). For each patient, differences between pre- and postoperative values were calculated and averaged for all of the DTI parameters in each white matter tract (fig 3). In order to investigate if DTI might possibly predict shunt surgery outcome, pre-operative DTI measures were compared with the clinical findings before shunt surgery and also with changes in clinical findings after shunt surgery.
Results
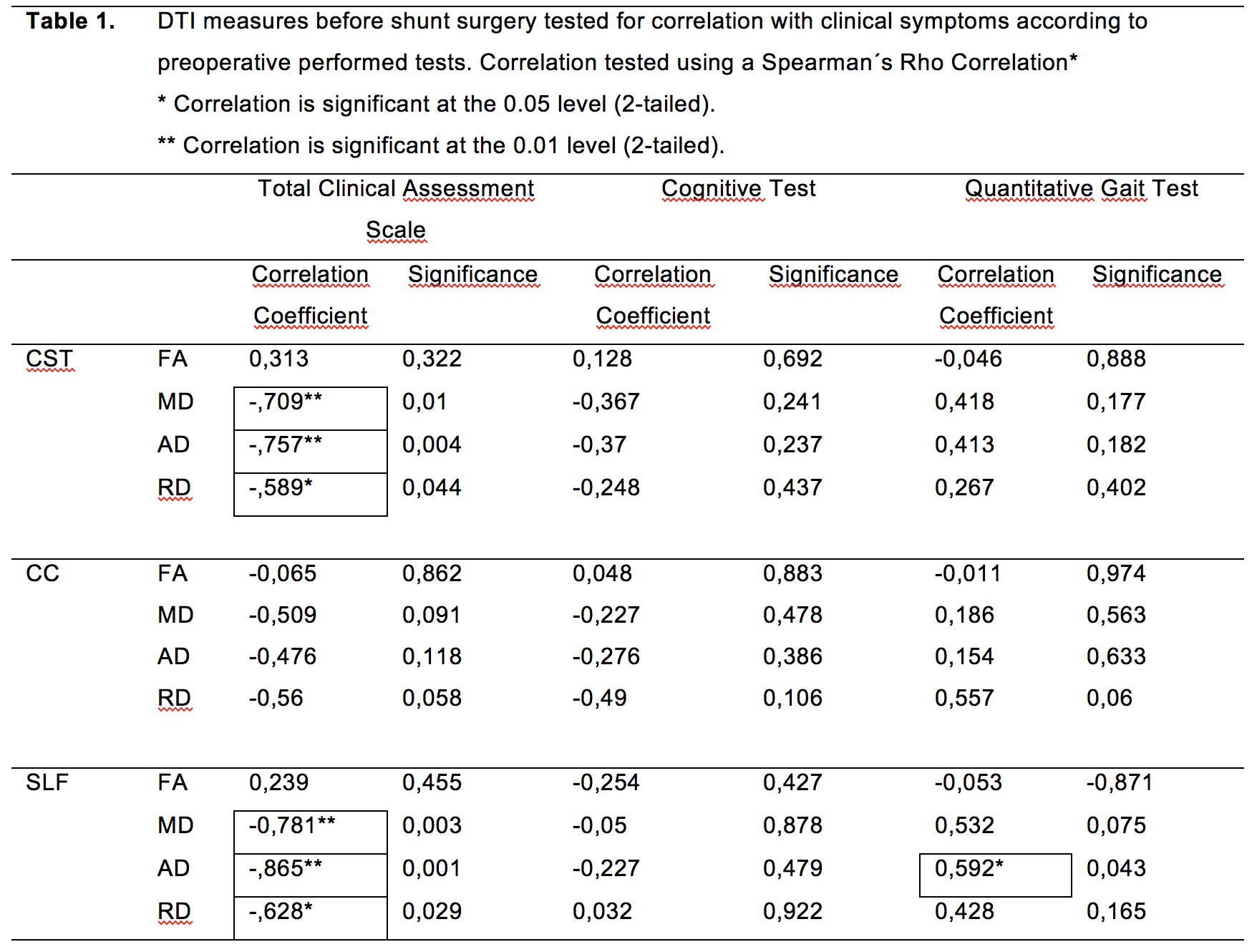
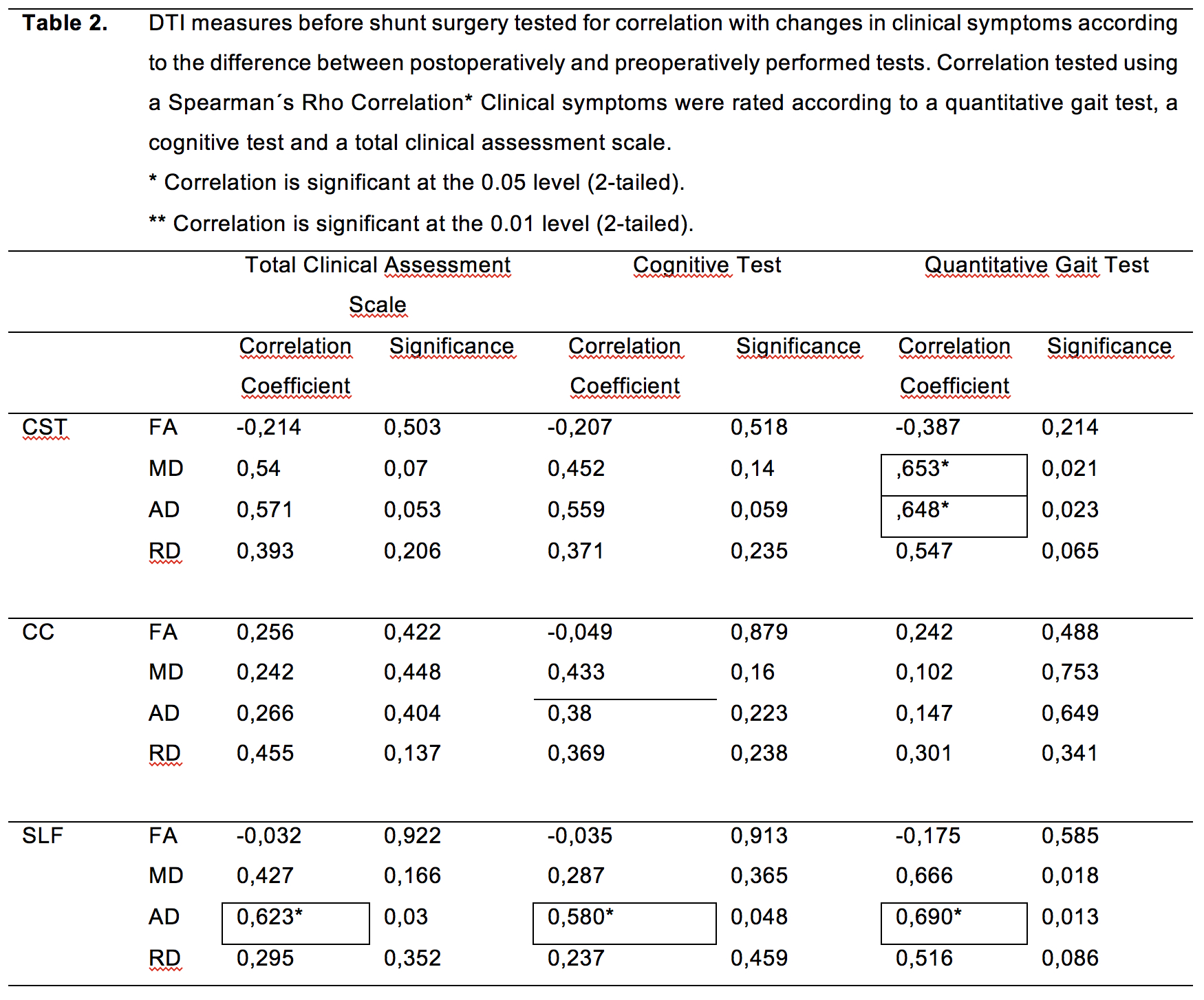
Diffusion measures differed significantly between healthy controls and patients for FA in CC (p<0,01), for MD in CC (p<0,05) and SLF (p<0,05), for AD in CST (p<0,01), and SLF (p<0,01), and for RD in CC (p<0,01) (fig 2). Correlations were found between the preoperative DTI measures MD, AD, and RD in CST and SLF, and preoperative tests of total clinical assessment (Table 1). Also, the AD in SLF correlated with preoperative cognitive tests (Table 1). Correlations were also found between preoperative MD and AD in CST and RD in SLF, and clinical changes in quantitative gait test after shunt surgery, and between AD in SLF, and all of the performed clinical tests after shunt surgery (Table 2). The presence of white matter lesions did not differ significantly between patients and healthy controls.Discussion
Since FA can increase and decrease in iNPH, it might be difficult to interpret results from FA only. Findings from MD agreed with previous observations.2,3 The smallest standard errors were found for AD and the findings regarding AD were in agreement with previous observations.4 The RD values initiated a non-significant trend. Different portions of CC contain different types of fibers depending on the coupled cortical areas. The superior part of CC showed visually large anatomical effects from the disease, while genu and splenium were different affected, which may have affected the CC analysis. In CST, higher values of AD may be secondary to compression of the tracts in the vicinity of the dilated ventricles. Results from previous studies were thereby replicated.4 SLF is compressed by enlarged ventricles, due to its anatomical location.Conclusion
DTI and tractography has emerged as tools for analyses of neurodegenerative diseases and microstructural processes of the brain, and thereby enhanced our understanding of neurodegeneration.5 Since correlations were found with between preoperative DTI results and preoperative clinical symptoms, as well as between preoperative DTI results and changes in clinical findings after shunt surgery, DTI may reflect important aspects of the pathophysiology in iNPH. Our findings suggest that DTI may become a supportive tool for the prediction of clinical outcomes from shunt surgery in patients with iNPH, but more standardized methods would be needed.Acknowledgements
References
1. Fazekas F, Chawluk JB, Alavi A, et al. MR signal abnormalities at 1.5 T in Alzheimer's dementia and normal aging. Am J Roentgenol. 1987;149(2):351-356.
2. Hattingen E, Jurcoane A, Melber J, et al. Diffusion Tensor Imaging in Patients With Adult Chronic Idiopathic Hydrocephalus. Neurosurg 2010;66(5):917-924.
3. Scheel M, Diekhoff T, Sprung C, et al. Diffusion tensor imaging in hydrocephalus--findings before and after shunt surgery. Acta Neurchir 2012;154(9):1699-1706.
4. Kamiya K, Masaaki H, Ryusuke I, et al. Diffusion imaging of reversible and irreversible microstructural changes within the corticospinal tract in idiopathic normal pressure hydrocephalus. NeuroImage Clin. 2017;14:663-671.
5.Cohen Y, Anaby D, and Morozov D. Diffusion MRI of the spinal cord: from structural studies to pathology. NMR Biomed. 2017;30:e3592.
Figures