3603
Effect of repetitive head trauma on diffusion MRI derived measures of diffusivity and free water1Imaging, Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, United States
Synopsis
In this study, we utilized the diffusion MRI (
Introduction
Studies have shown that both active and retired active professional athletes with repeated head trauma are more likely to suffer from cognitive decline and loss of executive and attention functions when compared to age-matched healthy controls1. Studies with diffusion-weighted magnetic resonance imaging (dMRI) in active fighters have shown increased mean diffusivity (MD) and decreased fractional anisotropy (FA) in the temporal and occipital white matter (WM) tracts and splenium of corpus callosum2–4. Pasternak et al have shown reduced free-water fraction (fiso) in concussed hockey players5. However, it is still unclear whether conventional single tensor dMRI derived metrics and fiso are different between cognitively impaired and nonimpaired active professional fighters. Hence, in this study, we evaluated fiso in cognitively impaired and nonimpaired active professional fighters from the Professional Fighters Brain Health Study (PFHBS)6. In addition, we also investigated whether conventional single tensor diffusion-derived metrics such as FA, MD, axial diffusivity (AD), and radial diffusivity (RD) and recently proposed weighted FA (FAwt)7 are different among cognitively impaired and nonimpaired active professional fighters. Furthermore, we also investigated whether there was any association of neuropsychological scores and exposure to fighting with diffusion-derived metrics using clinical dMRI data.Methods
Subjects: A total of 252 active professional fighters (18 females (F)) were recruited at our centre. Each subject went through a battery of neuropsychological assessment tests to measure psychomotor speed (PSY) and processing speed (P). The fighters were classified as cognitively impaired if the standardized PSY and P scores were 1.5 standard deviations below the mean8. The rest were classified as nonimpaired fighters. In addition, the single-shot-EPI sequence was used to acquire dMRIs with 71 diffusion directions and b-value of 1000 s/mm2; TR/TE/Resolution=7000ms/91ms/2.5mm3 on all subjects with a 3T Siemens Verio scanner with a 32 channel head coil. Only 70 impaired fighters (3F, age=29.91±6.29 years, years of education (YOE)=13.21±2.17 years) had acceptable dMRI data. 70 nonimpaired fighters (7F, age=29.2±6.5 years, YOE=13.66±1.68 years) were then selected randomly from the cohort of nonimpaired active fighters but matched for all demographics. Data processing: Standard processing steps were used to fit diffusion tensors after eddy current distortion correction in FSL. Voxelwise measures of FA, MD, AD, and RD were extracted for every subject and standard tract-based spatial statistics (TBSS) was conducted to investigate voxelwise differences between the groups. Estimation of fiso and FAwt: Since the algorithm of Pasternak et al9 has been shown to be biased at regions of crossing-fiber regions (CFR)7 and more than 90% of WM tracts have CFRs10, a recently proposed technique for unbiased estimation of fiso and FAwt7 was used and the measures were extracted at each voxel for each subject. FA without fiso bias was also calculated at each voxel. Only 10 randomly selected subjects in each group were used for this analysis. Statistical tests: All statistical tests were conducted using PALM11 and were corrected for the demographics. A regression analysis was then conducted to evaluate the effect of repetitive head trauma on dMRI measures.Results
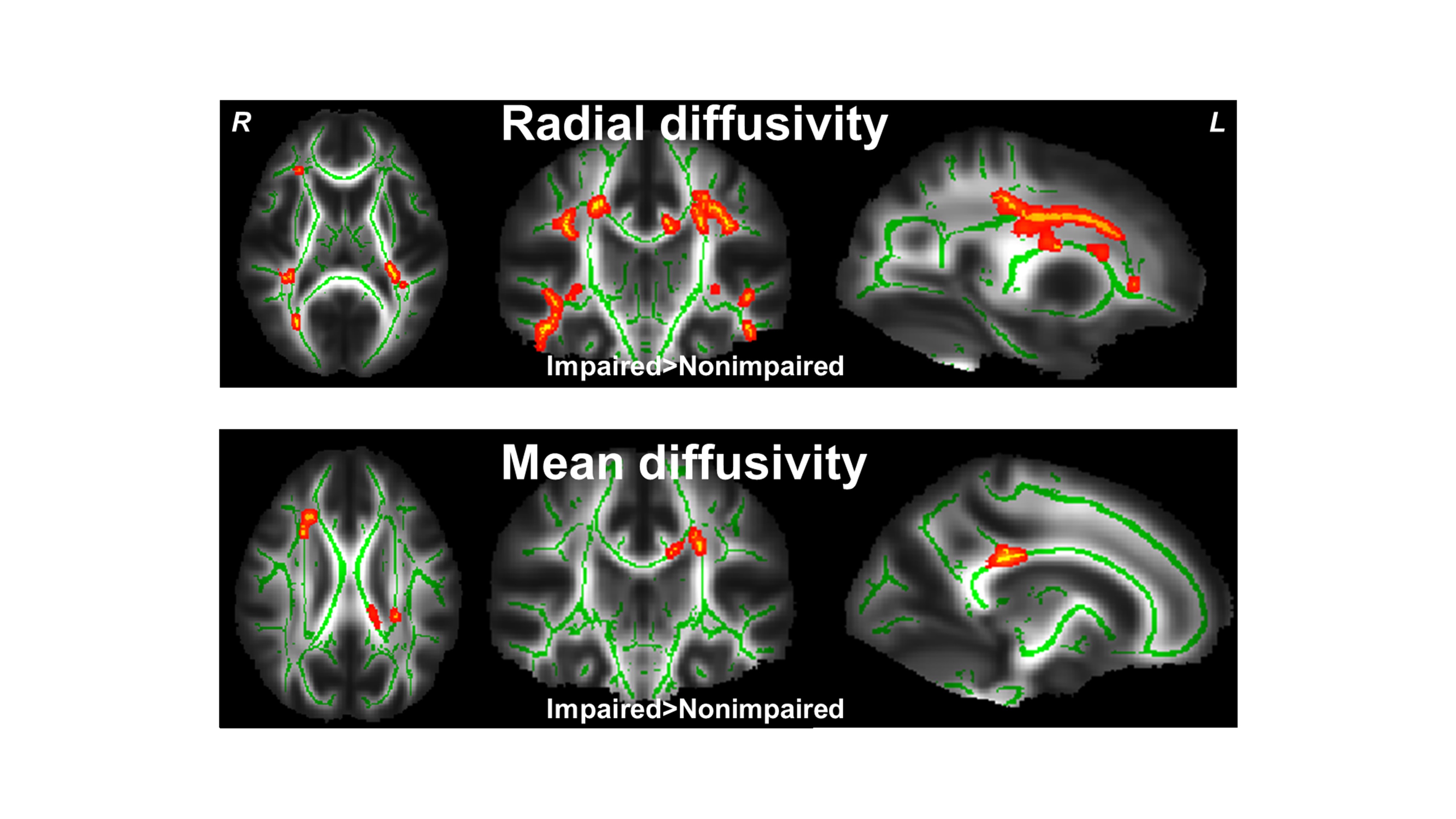
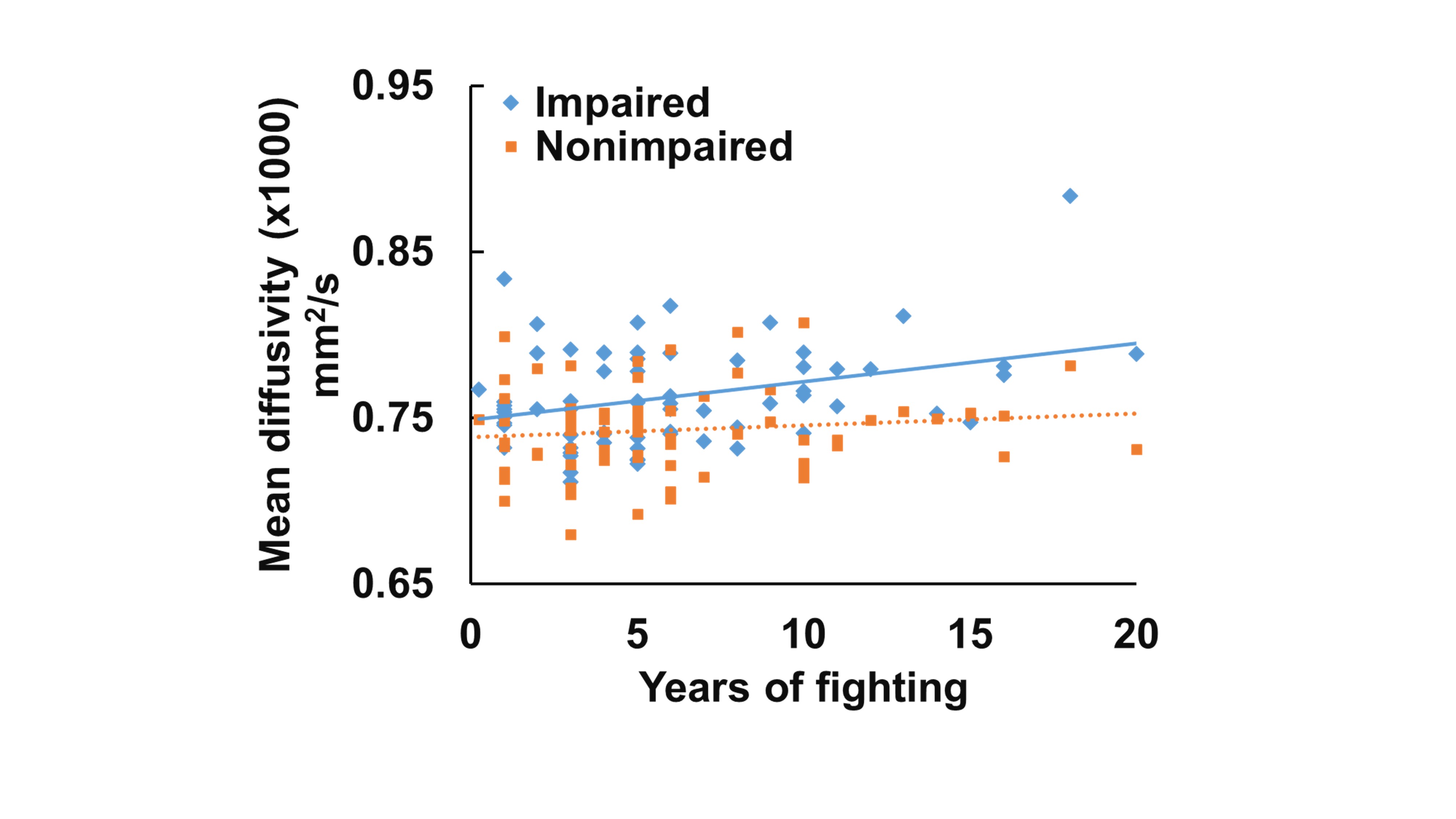
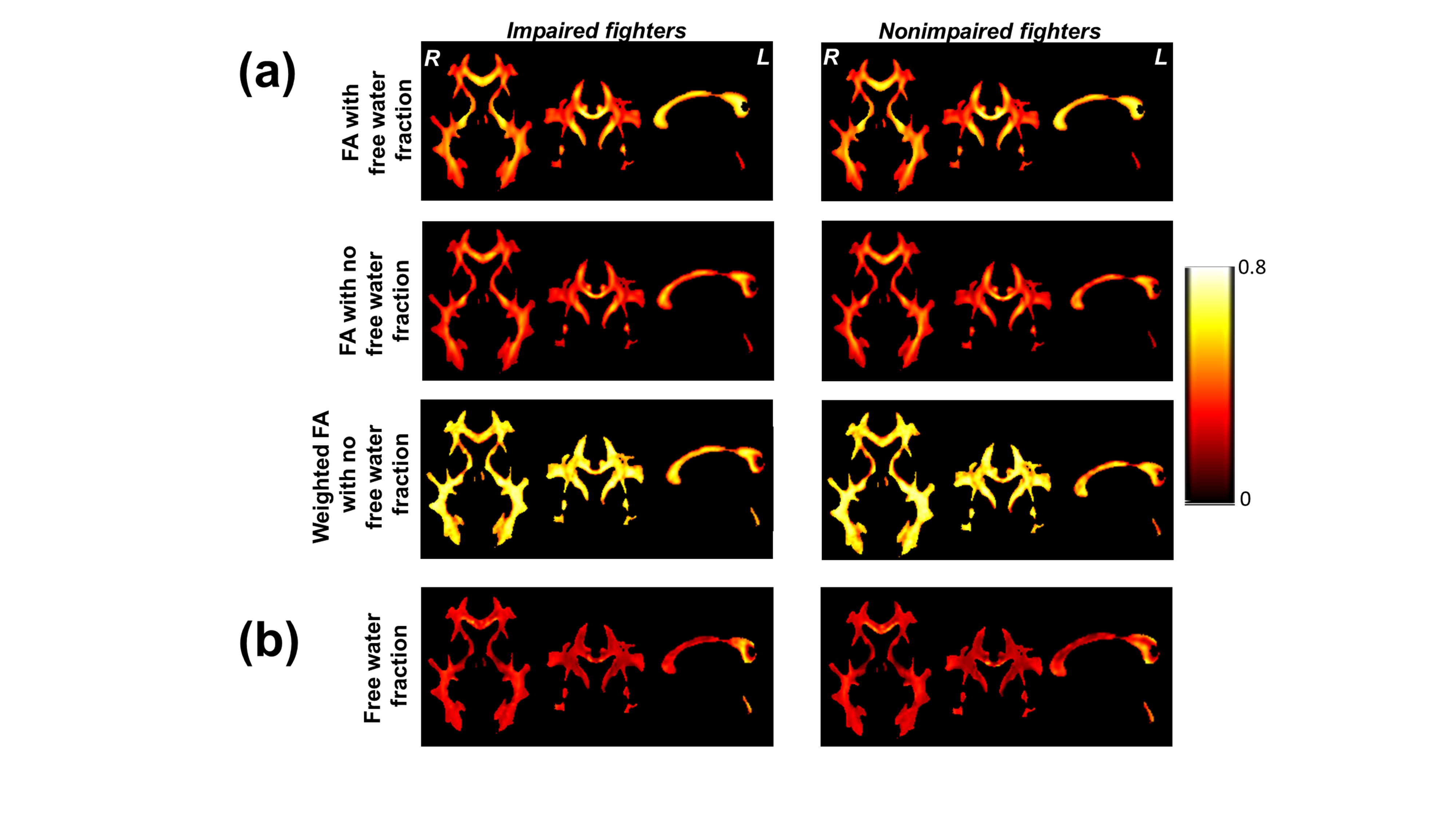
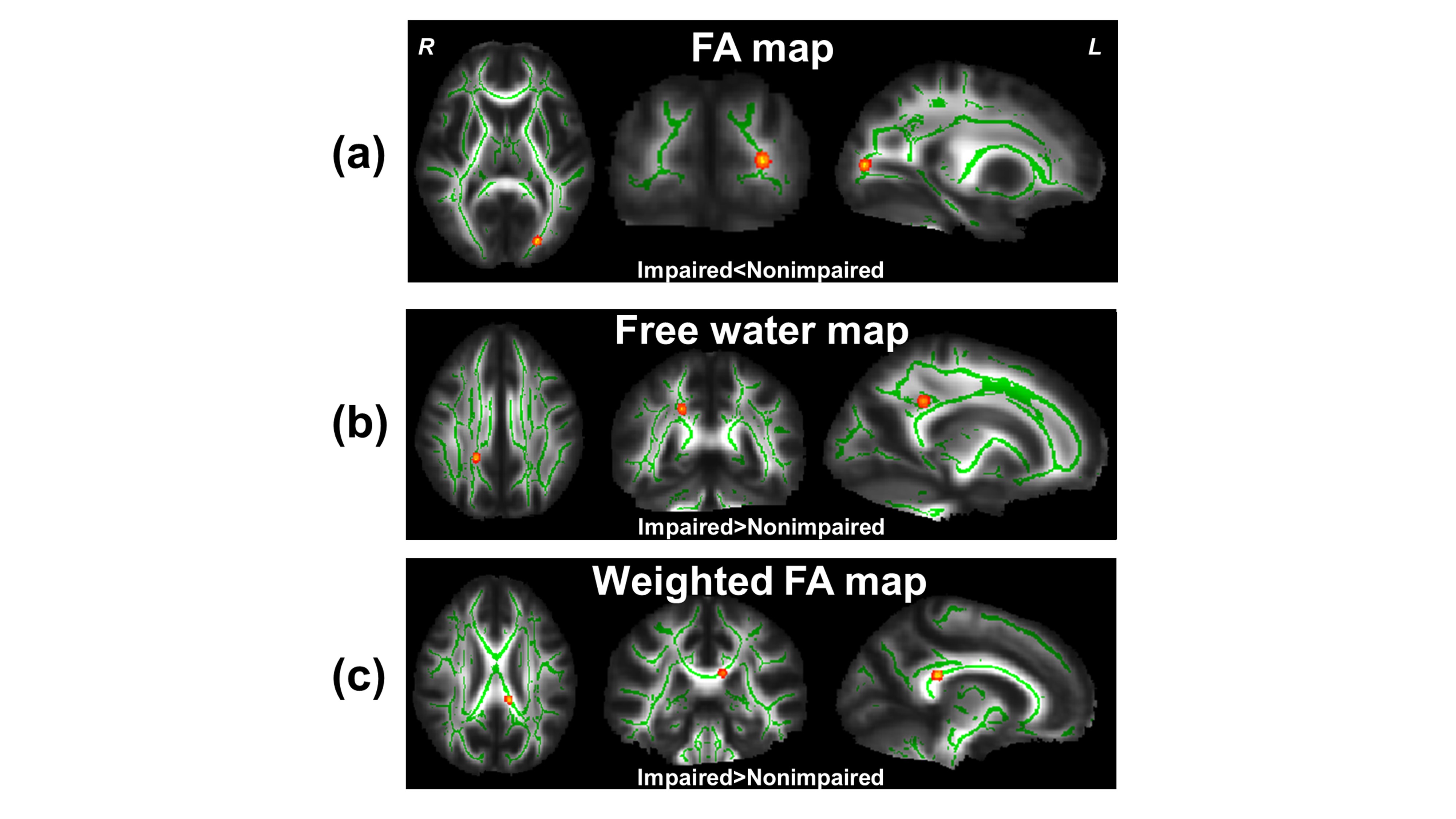
Increased RD and MD were obtained in cognitively impaired active professional fighters as shown in Fig.1. Most of the regions that passed significance testing are located in the CFRs. Significant diffusivity values were extracted for each subject and MD was shown to be positively associated with years of fighting in cognitively impaired active professional fighters. Left and right panel of Fig.3a and Fig.3b shows conventional FA, FA without fiso bias, FAwt, and fiso for cognitively impaired and nonimpaired active fighters respectively. As can be seen, a very uniform fiso and FAwt was obtained throughout the WM tracts for both the groups. Statistical analysis revealed a cluster in the splenium of corpus callosum where impaired fighters had reduced FA as compared to nonimpaired fighters (Fig.4a). In addition, a cluster in corticospinal tract was obtained where fiso in impaired fighters was significantly greater than nonimpaired active fighters (Fig.4b). Impaired fighters also revealed a cluster in the genu of corpus callosum where FAwt in impaired fighters was greater than nonimpaired active professional fighters.Discussion and Conclusion
In this study, we showed that conventional single tensor dMRI derived metrics are significantly greater and are associated with years of fighting. We also showed for the first time that unbiased fiso and FAwt was greater in cognitively impaired active professional fighters. These findings suggest selective damage of WM tracts in CFR of impaired active fighters and the advanced dMRI measures may provide more sensitive imaging biomarkers in patients exposed to repetitive head trauma.Acknowledgements
The study issupported by the National Institutes of Health (grant number 1R01EB014284 and P20GM109025).References
1 McKee AC, Stern RA, Nowinski CJ, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain 2013; 136: 43–64.
2 Montenigro PH, Bernick C, Cantu RC. Clinical features of repetitive traumatic brain injury and chronic traumatic encephalopathy. Brain Pathol 2015; 25: 304–17.
3 Hulkower MB, Poliak DB, Rosenbaum SB, Zimmerman ME, Lipton ML. A decade of DTI in traumatic brain injury: 10 years and 100 articles later. AJNR Am J Neuroradiol 2013; 34: 2064–74.
4 Wintermark M, Sanelli PC, Anzai Y, Tsiouris AJ, Whitlow CT. Imaging evidence and recommendations for traumatic brain injury: advanced neuro- and neurovascular imaging techniques. AJNR Am J Neuroradiol 2015; 36: E1–11.
5 Pasternak O, Koerte IK, Bouix S, et al. Hockey Concussion Education Project, Part 2. Microstructural white matter alterations in acutely concussed ice hockey players: a longitudinal free-water MRI study. J Neurosurg 2014; 120: 873–81.
6 Bernick C, Banks S, Phillips M, et al. Professional fighters brain health study: Rationale and methods. Am J Epidemiol 2013; 178: 280–6.
7 Mishra V, Guo X, Delgado MR, Huang H. Toward tract-specific fractional anisotropy (TSFA) at crossing-fiber regions with clinical diffusion MRI. Magn Reson Med 2014; 0: 1–12.
8 Schinka JA, Loewenstein DA, Raj A, et al. Defining mild cognitive impairment: impact of varying decision criteria on neuropsychological diagnostic frequencies and correlates. Am. J. Geriatr. Psychiatry. 2010; 18: 684–91.
9 Pasternak O, Sochen N, Gur Y, Intrator N, Assaf Y. Free water elimination and mapping from diffusion MRI. Magn Reson Med 2009; 62: 717–30.
10 Jeurissen B, Leemans A, Tournier J-D, Jones DK, Sijbers J. Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum Brain Mapp 2013; 34: 2747–66.
11 Winkler AM, Ridgway GR, Douaud G, Nichols TE, Smith SM. Faster permutation inference in brain imaging. Neuroimage 2016; 141: 502–16.
Figures