3476
Feasibility of coronary artery wall imaging using 3D turbo spin-echo (black blood -T1-VISTA) in children with Kawasaki disease1Department of Radiology, Chiba University Hospital, Chiba, Japan, 2Division of Health Sciences, Graduate School of Medial Science, Kanazawa University, Kanazawa, Japan, 3Diagnostic Radiology and Radiation Oncology, Graduate School of Medicine, Chiba University, Chiba, Japan, 4Department of Pediatrics, Chiba University Hospital, Chiba, Japan
Synopsis
We evaluate feasibility of three-dimensional turbo spin echo imaging (BB-T1-VISTA) as coronary artery wall imaging for Kawasaki disease. BB-T1-VISTA could visualize the proximal regions of the coronary artery appropriately. BB-T1-VISTA with axial orientation produced the highest reproducibility to magnetic resonance coronary angiography (MRCA). Although BB-T1-VISTA showed significantly smaller diameter than MRCA, the limits of agreement were small in the proximal regions with normal diameter. By contrast, the larger aneurysms were, the larger bias became between MRCA and BB-T1-VISTA. BB-T1-VISTA has a potential to evaluate wide range of the coronary artery at once and was feasible in regions with small diameter.
Introduction
Magnetic resonance coronary angiography (MRCA) with low invasiveness is used for evaluating coronary arterial lesions of Kawasaki disease (KD). MRCA is equivalent to coronary angiography for coronary artery aneurysm identification in patients with KD [1]. However, MRCA cannot detect thrombus and intimal proliferation sufficiently [2], so that black blood (BB) imaging is desirable [2]. There was a report using the two-dimensional dual inversion recovery techniques for KD [3]. However, this paper lacks feasibility analyses and two-dimensional imaging is clinically struggling to set imaging section because the childhood coronary artery is small. By contrast, the three-dimensional imaging can easily obtain a cross section by post-processing. Three-dimensional turbo spin echo imaging (BB-T1-VISTA) has been widely used as vessel wall imaging in the carotid artery. To evaluate feasibility of BB-T1-VISTA for children with KD, we developed cardiac gating and real-time navigator echo technique.Materials and methods
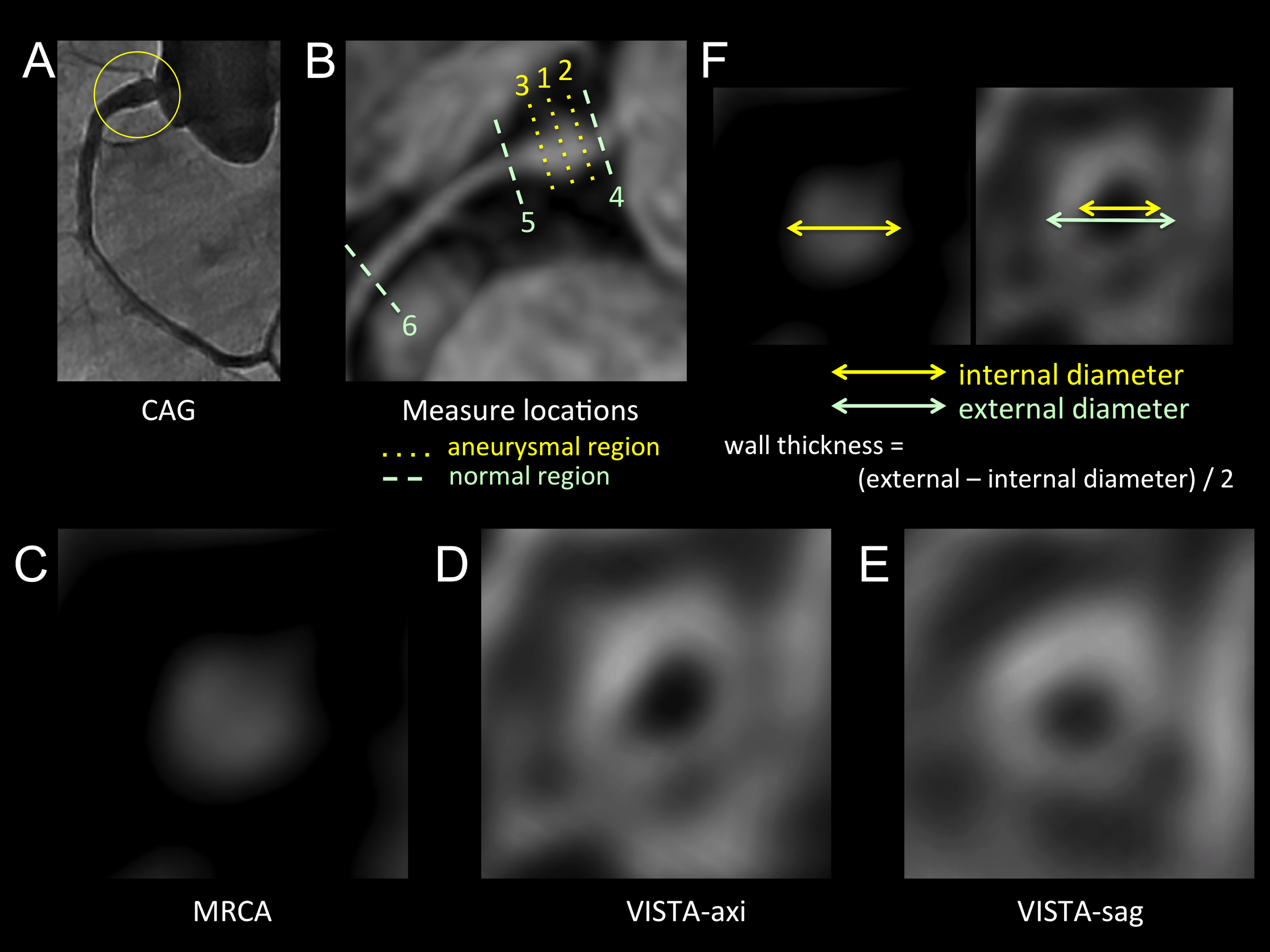
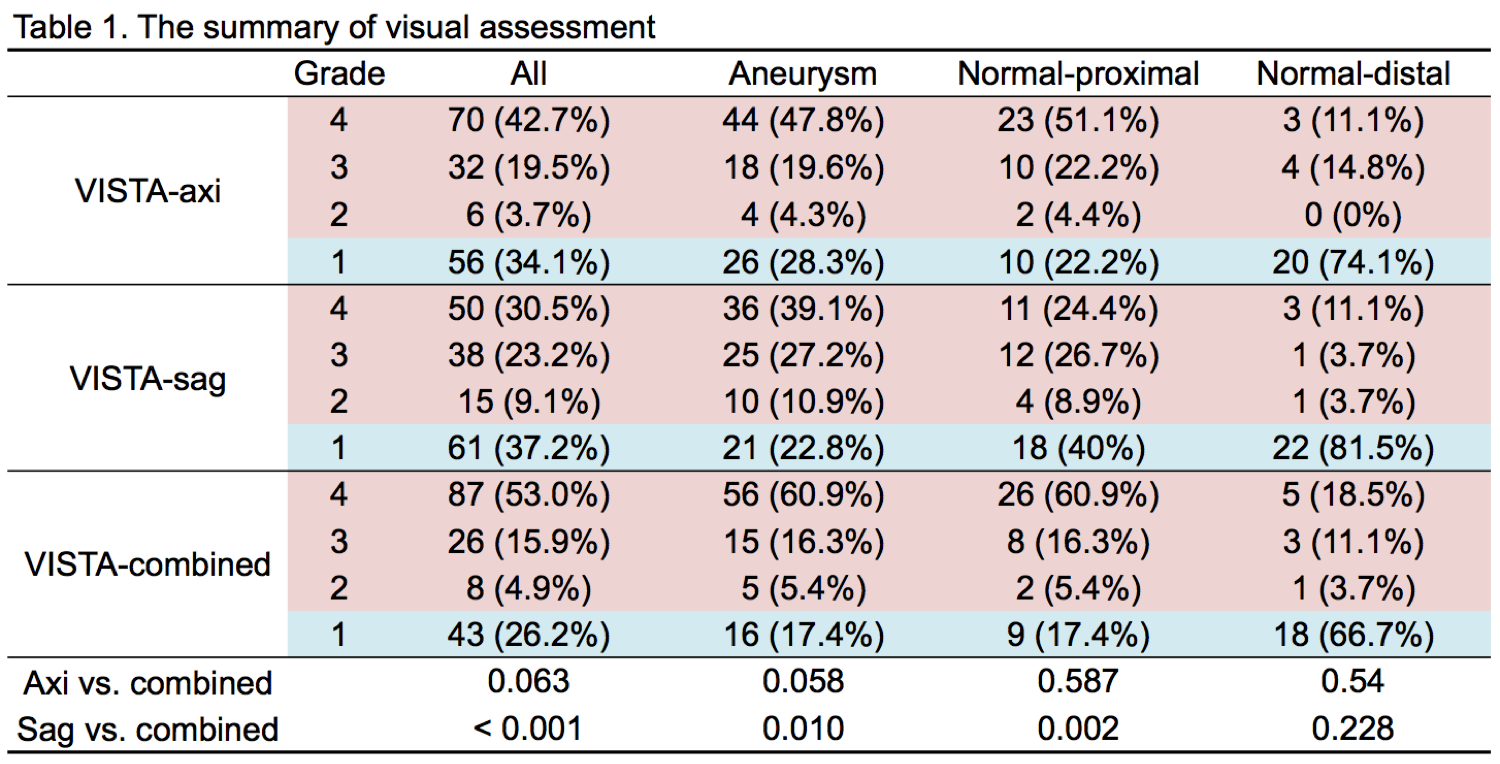
Patients’ families gave informed consent, and the study was approved by the local ethics committee. Subjects: Nine pediatric patients (3 boys) in age from 1 year to 10 years (mean ± SD, 5.6 ± 3.3 years) were enrolled in this study. Data acquisition: All MR imaging studies were performed on 1.5-tesla MR imaging units (Intera Achieva Release 3.2, Philips Medical Systems) by using a two-element flex-medium coils (Flex-M) or a five-element synergy cardiac coils. A high-resolution 2D cine scan with axial slice orientation was used to identify precisely the individual period of minimal cardiac motion. Subsequently, MRCA with axial slice orientation, BB-T1-VISTA with axial slice orientation (VISTA-axi), and BB-T1-VISTA with sagittal slice orientation (VISTA-sag) were acquired for a whole heart. The BB-T1-VISTA was obtained with the following parameters: repetition time, 1beat (522-800 ms); echo time, 24-44 ms; refocusing flip angle: 50°, turbo factor, 9-15; field-of-view, 210-290 mm; slice thickness, 1.1-1.6 mm; flow compensation: sensitized; and scan time: 10-18 minutes. The heart rate range was 72-108 beats per minute (BPM) (mean ± SD, 91.3 ± 10.9 BPM). No thrombosis was pointed out in coronary artery angiography or transthoracic echocardiography. Postprocessing: According to coronary artery segments of American heart association (AHA) classification, #1-3 of the right coronary artery, #5-8 and #11-15 of the left coronary artery were assessed. #3, #8 and #15 were classified into the distal region, and others were classified in to the proximal region. Cross-sectional images were created on MRCA, VISTA-axi, and VISTA-sag, respectively (Fig. 1). Evaluation: The image quality of cross-sectional images was visually graded with 4-scale grades (4, excellent; 3, good; 2, adequate; 1, poor). Internal diameter and wall thickness were measured in the cases with grade 2 to 4 (Fig. 1). VISTA-axi and VISTA-sag were combined using the visual grades (VISTA-combined). On each location, we selected measurements from either VISTA-axi or VISTA-sag with better visual grade. Analysis: To evaluate reproducibility of internal diameter, interclass correlation coefficient (ICC) and Bland-Altman plot were used. Fixed and proportional biases were defined as significance on a paired t-test and linear regression with a P-value less than 0.05, respectively. To evaluate relationship between internal diameter and wall thickness, scatter plot and correlation test were used.
Results
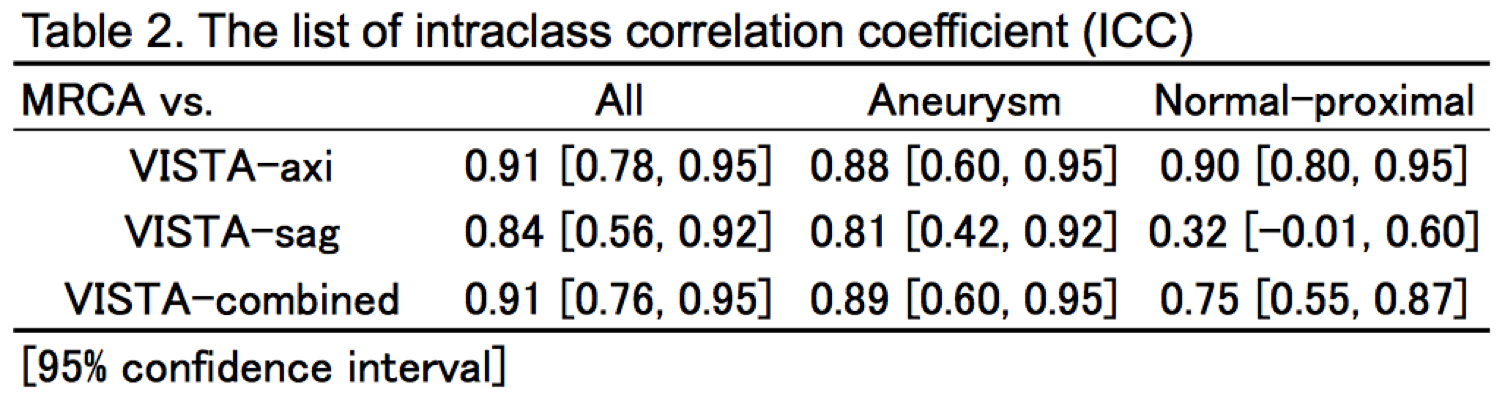
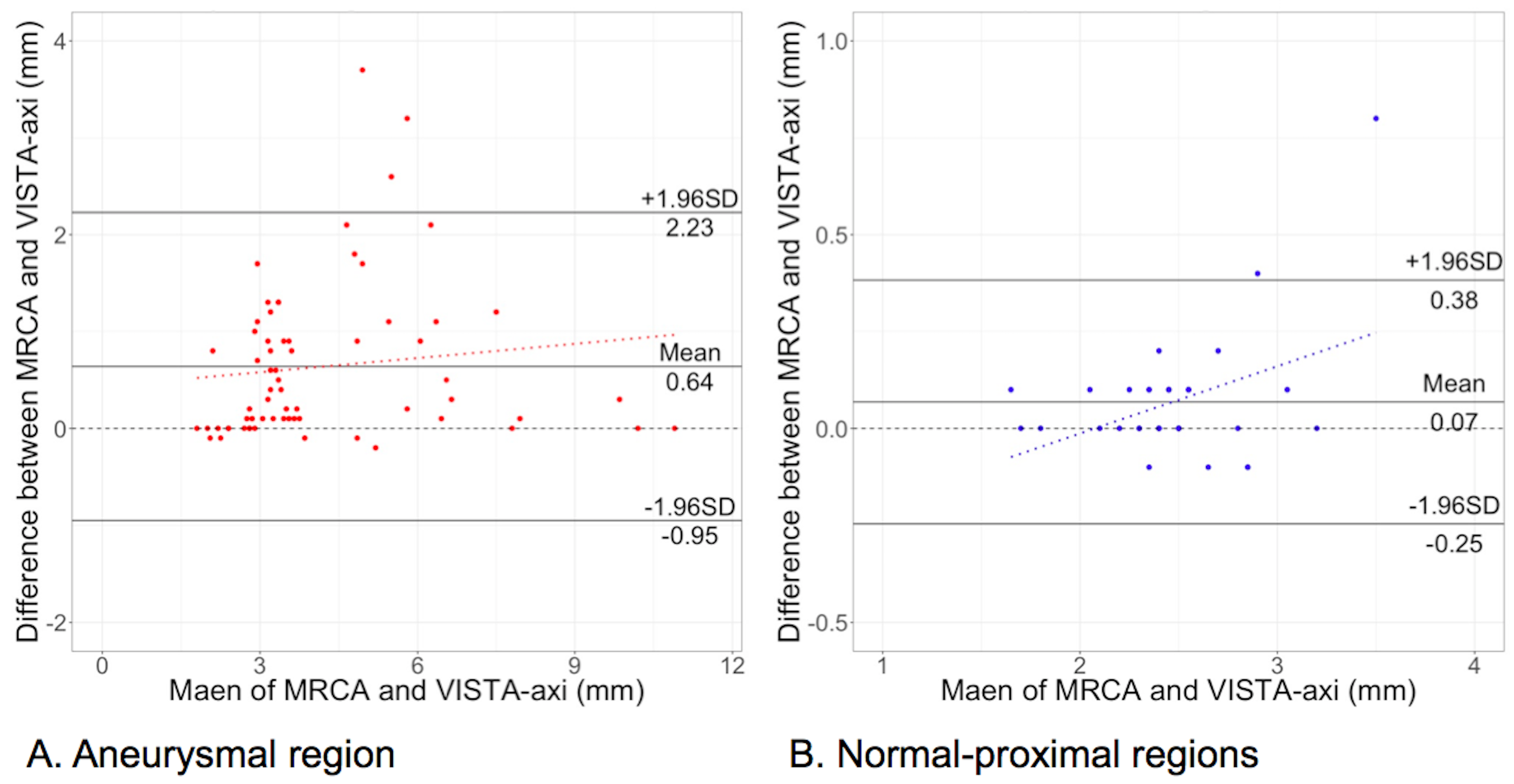
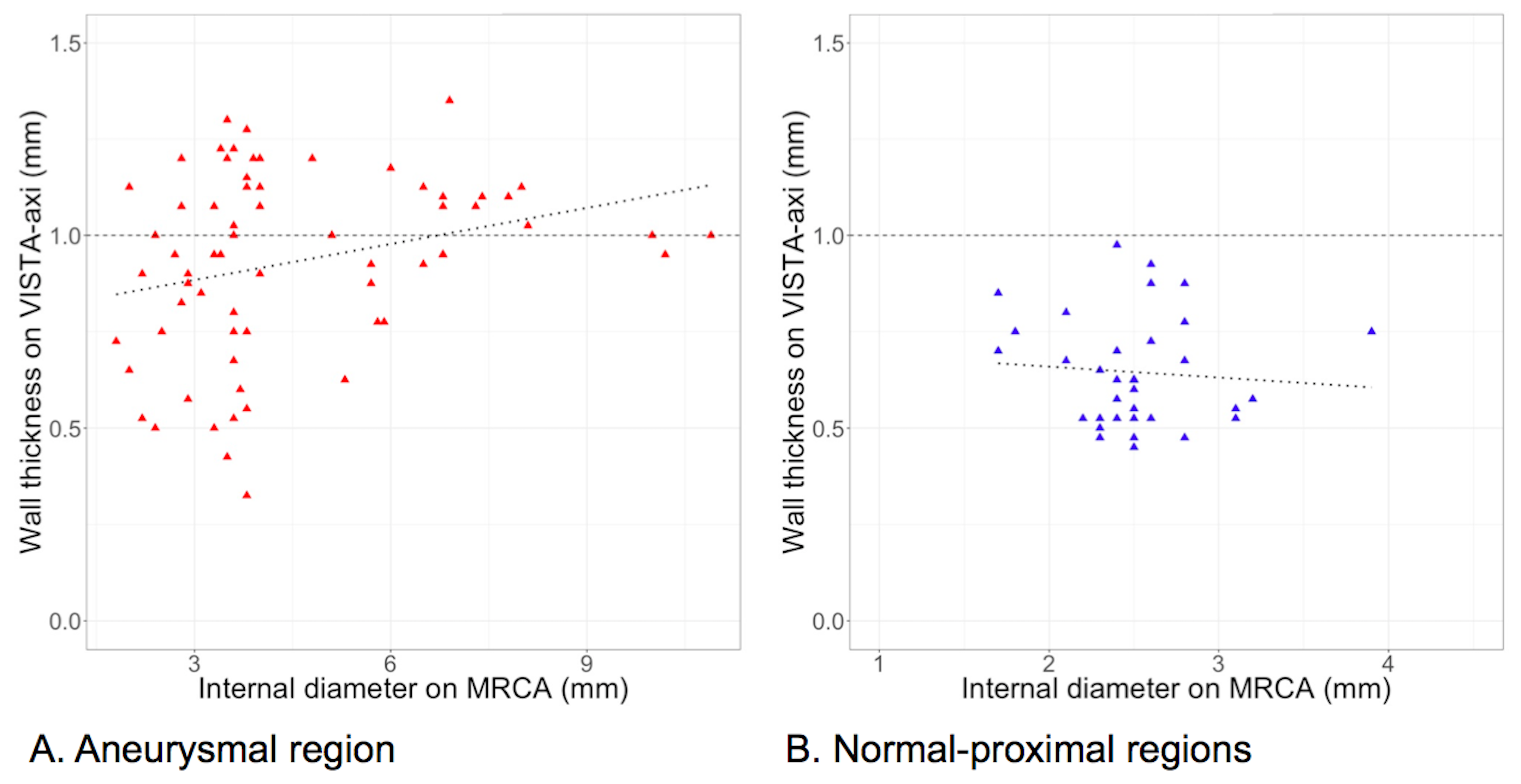
We evaluated 164 locations (aneurysmal regions, 92; normal-proximal, 45; normal-distal, 27) of the coronary artery. The aneurysms were located in only the proximal region. MRCA had excellent reproducibility to coronary angiography or echocardiography (ICC = 0.98), so that MRCA was used as the standard measurement of internal diameter in this study. The results of the visual assessment were summarized in Table 1. VISTA mostly missed visualization in the distal region. Thereby, the distal regions were removed from the following analyses. ICCs of internal diameter were listed in Table 2. VISTA-axi showed higher reproducibility performance than VISTA-sag in both aneurysmal and normal-proximal regions. Additionally, VISTA-combined could not overcome VISTA-axi, so that Bland-Altman and scatter plots were created using VISTA-axi alone (Fig 2 and 3).Discussion and conclusions
BB-T1-VISTA could visualize the proximal region, while visualization for the distal regions was poor. The acquisition directions influenced the results of visual assessments. Flow direction and flow speed should be related to the results. The axial acquisition had higher performance than sagittal acquisition. The combination could not improve reproducibility performance. Therefore, VISTA-axi might have more versatility. Although internal diameter looked smaller in VISTA-axi than in MRCA, the limits of agreement were small in the normal-proximal region. In the normal-proximal region, wall thickness was not correlated with internal diameter on MRCA. These results suggested that thrombosis and wall thickness assessments by VISTA-axi might be reliable in the normal-proximal region. In the aneurysmal region, the larger the aneurysmal diameter was, the larger the bias between MRCA and VISTA-axi became. Careful evaluation for thrombosis and wall thickness should be needed for especially in large aneurysms.Acknowledgements
No acknowledgement found.References
- Mavrogeni S, Papadopoulos G, Douskou M, et al. Magnetic resonance angiography is equivalent to X-ray coronary angiography for the evaluation of coronary arteries in Kawasaki disease. J Am Coll Cardiol. 2004;43:649-52.
- Suzuki A, Takemura A, Inaba R, et al. Magnetic resonance coronary angiography to evaluate coronary arterial lesions in patients with Kawasaki disease. Cardiol Young. 2006;16:563-71.
- Greil GF, Seeger A, Miller S, et al. Coronary magnetic resonance angiography and vessel wall imaging in children with Kawasaki disease. Pediatr Radiol. 2007;37:666-73.
Figures