3468
Quantitative Assessment of Carotid Artery Atherosclerosis by Three-Dimensional Magnetic Resonance Imaging and 2D Ultrasound: A Comparison StudyHuiyu Qiao1, Ying Cai2, Qiang Zhang1, Lingyun Huang3, Manwei Huang4, Chun Yuan1,5, and Xihai Zhao1
1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Department of Radiology, Taizhou People's Hospital, Taizhou, China, 3Clinical Sites Research Program, Philips Research China, Shanghai, China, 4Department of Ultrasound, China Meitan General Hospital, Beijing, China, 5Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
The size of carotid atherosclerotic plaques is associated with ischemic cerebrovascular events. Both 3D MR vessel wall imaging and 2D ultrasound can measure carotid plaques. To improve the work flow of screening for subclinical carotid atherosclerosis, this study sought to compare the quantitative measurements of carotid plaque between 3D MR and 2D ultrasound imaging. Excellent agreement was found between MR and ultrasound imaging in measuring carotid artery maximum wall thickness. Although there was moderate to strong correlation between MR and ultrasound imaging, the plaque area measured by MR imaging was more than two folds than that measured by ultrasound imaging.
Introduction
Increasing evidences have shown that carotid atherosclerotic plaque burden characterized by wall thickness or area is associated with plaque vulnerability1 and subsequent cerebrovascular events, such as ischemic stroke and transient ischemia attack.2,3 Therefore, it is important to accurately assess carotid plaque size prior to occurrence of events. Ultrasound imaging is considered to be the first-line screening tool for carotid plaques. However, it has poor inter-operator reproducibility due to variations in experience and scanning plane. Despite the capability of accurately characterizing plaque morphology,4 magnetic resonance (MR) vessel wall imaging is not an ideal modality for screening due to high cost. To improve the work flow of screening for subclinical carotid atherosclerosis, this study sought to compare the quantitative measurements of carotid plaque between MR and ultrasound imaging.Methods
Study sample: Forty-four arteries with atherosclerotic plaque from 31 asymptomatic subjects (mean age, 73.0 ± 6.2 years; 21 males) who underwent MR and ultrasound imaging for carotid arteries were included in this study. MR Imaging: Carotid arteries were imaged on 3.0T MR scanner (Achieva TX, Philips Healthcare) with custom-designed 36-channel cerebrovascular coil. A 3D T2-VISTA sequence was acquired coronally with the following parameters: TSE, TR/TE 2500/275 ms; field of view 250×160×45 mm3, and spatial resolution 0.8×0.8×0.8 mm3. Ulrasound Imaging: B-mode and color Doppler ultrasound imaging were performed for all carotid arteries on a Philips iU22 ultrasound system with the L9-3 linear array transducer. The carotid plaque thickness and area were measured from the longitudinal and cross-sectional views of the plaques. Image Analysis: All MR images were reviewed by two radiologists with >3 years’ experience in cardiovascular MR imaging using a custom designed software. Each artery was divided into common carotid artery (CCA) and internal carotid artery (ICA) segments. The boundaries of lumen and outer wall were outlined semi-automatically and adjusted on the cross-sectional view of each carotid segment which is perpendicular to the centerline of carotid artery. Boundaries and auto-calculated wall thickness (WT) information of each slice were recorded in eXtensible Markup Language (XML) files. All the files were loaded into MATLAB. The plaque area was measured at the slice with the maximum WT (Max WT) across all slices of each carotid segment. Plaque area was defined as the area of the region (the red area in Figure 1) from Max WT to a threshold of WT, such as 1.5 mm, 1.6 mm, 1.7 mm, 1.8 mm, 1.9 mm and 2.0 mm. All ultrasound images were reviewed to measure plaque thickness and area manually by a sonographer with 25 years’ experience in carotid imaging. Statistical Analysis: The Max WT and plaque area were compared between 3D MR and ultrasound imaging using paired t test. Spearman correlation was conducted to evaluate the agreement of plaque measurements between 3D MR and ultrasound imaging. Bland-Altman analysis was performed to determine the differences in measuring the Max WT between MR and ultrasound imaging.Results
The Max WT of plaque measured by MR imaging was significantly greater than that measured by ultrasound (3.2 ± 1.1 mm vs. 2.6 ± 0.7 mm, p<0.001). Significant correlation was found between Max WT measured by MR and ultrasound (r=0.7, p<0.001, Figure 2). The mean area of all 44 plaques measured by ultrasound was 16.8 ± 13.3 mm2. In contrast, the plaque areas measured by MR imaging were significantly larger than those measured by ultrasound using WT threshold from 1.5 mm to 2.0 mm (all p <0.001, Table 1). The correlation coefficients of between plaque area measured by MR and ultrasound increased from 0.486 to 0.658 with the WT threshold from 1.5mm to 2.0mm (all p ≤0.001, Table 1).Discussion and Conclusion
Excellent agreement was found between 3D MR and ultrasound imaging in measuring maximum wall thickness of carotid plaques. Although there was moderate to strong correlation between MR and ultrasound imaging, the plaque area measured by MR imaging was more than two folds than that measured by ultrasound imaging. The differences in plaque size measurement between MR and ultrasound imaging might be due to the methodology of assessment. On 3D MR imaging, the wall thickness and plaque area were derived from the whole layers of vessel wall from intima to adventitia. In contrast, ultrasound imaging can only confidently delineate intima and media of arteries. In addition, the plaque size measured by 2D ultrasound is heavily dependent on the orientation of the scan by sonographer. Recently, 3D ultrasound imaging has been utilized to assess carotid plaques which may enable more accurate quantitative assessment.5,6Acknowledgements
No acknowledgement found.References
- Zhao X, Underhill HR, Zhao Q, et al. Discriminating carotid atherosclerotic lesion severity by luminal stenosis and plaque burden: a comparison utilizing high-resolution magnetic resonance imaging at 3.0 Tesla. Stroke. 2011;42:347-353.
- Parmar JP, Rogers WJ, Mugler JR, et al. Magnetic resonance imaging of carotid atherosclerotic plaque in clinically suspected acute transient ischemic attack and acute ischemic stroke. Circulation. 2010;122:2031-2038.
- Gupta A, Baradaran H, Schweitzer AD, et al. Carotid plaque MRI and stroke risk: a systematic review and meta-analysis. Stroke. 2013;44:3071-3077.
-
Saam T, Ferguson MS, Yarnykh VL, et al.
Quantitative evaluation of carotid plaque composition by in vivo MRI. Arterioscler
Thromb Vasc Biol. 2005;25:234-239.
- Chiu B, Egger M, Spence JD, et al. Quantification of carotid vessel wall and plaque thickness change using 3D ultrasound images. Med Phys. 2008;35:3691-3710.
- Yamaguchi M, Sasaki M, Ohba H, et al. Quantitative assessment of changes in carotid plaques during cilostazol administration using three-dimensional ultrasonography and non-gated magnetic resonance plaque imaging. Neuroradiology. 2012;54:939-945.
Figures
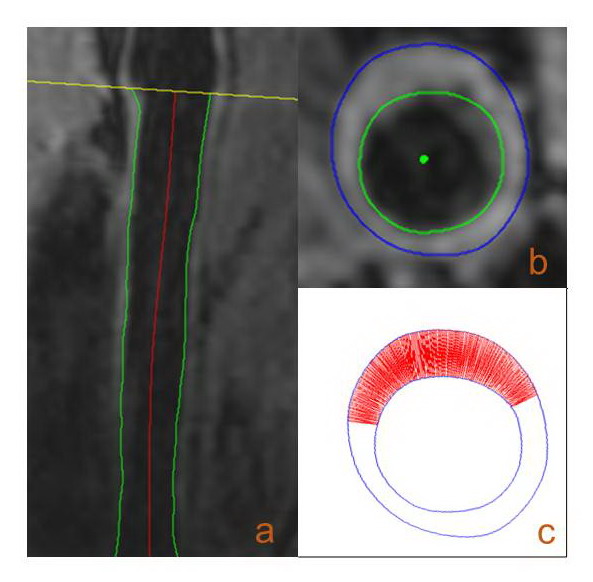
Figure 1. Methodology
for measuring plaque area on MR images. The common carotid artery was shown in
a, and b is the cross-sectional slice with maximum wall thickness. The red area
in c represents plaque area defined as the region from maximum wall thickness
to threshold wall thickness.
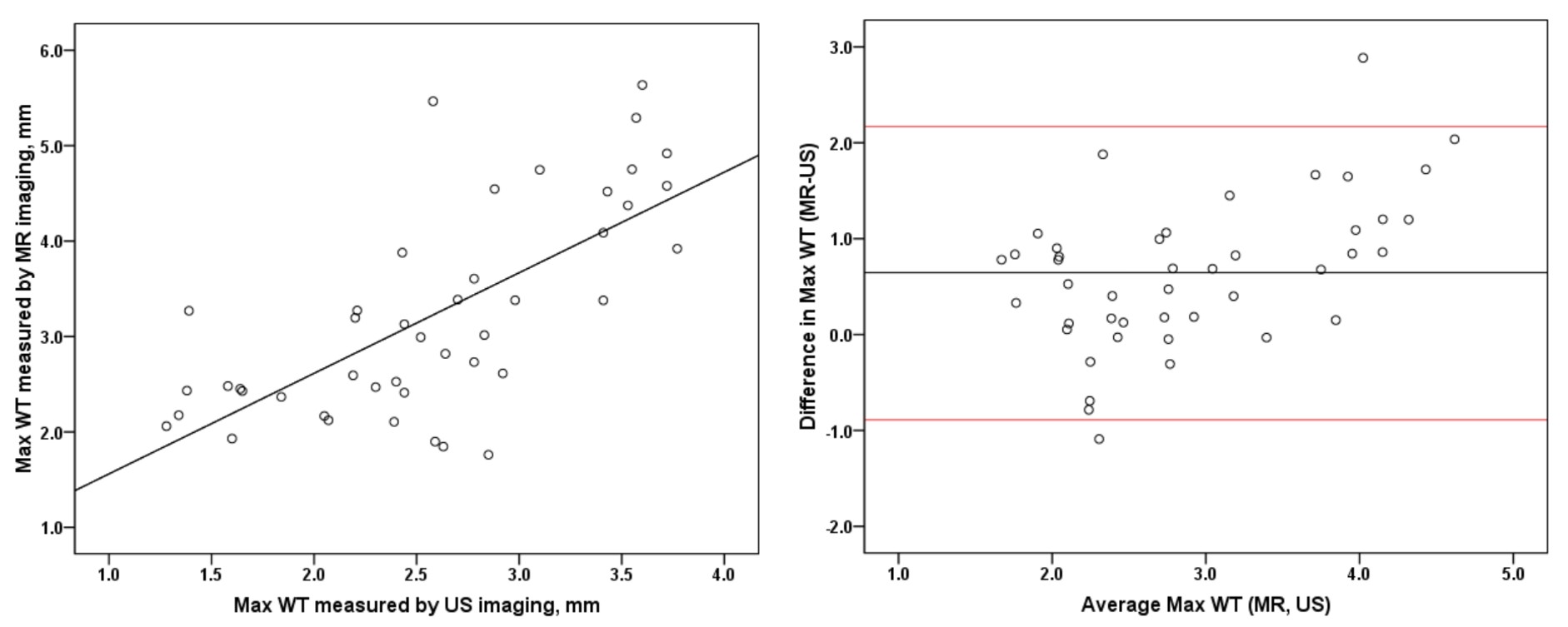
Figure 2. Correlation
of Max WT measurement between MR and ultrasound imaging.
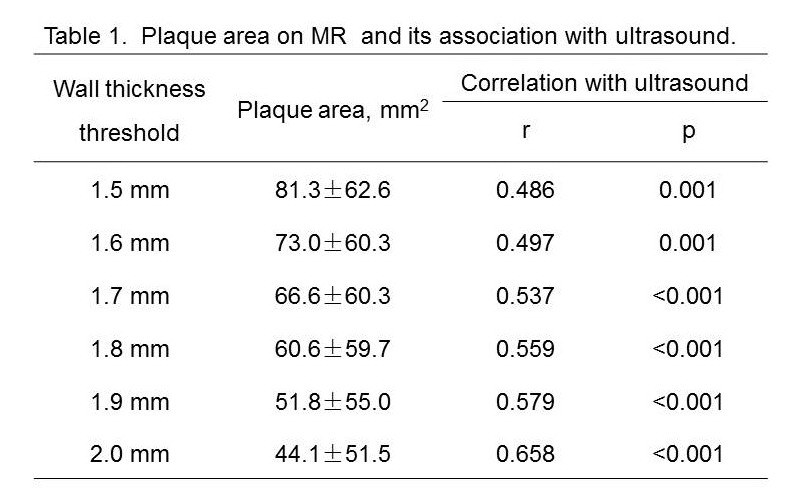
Table 1. Plaque area on MR and its association with ultrasound.