3463
3D dual-contrast vessel wall imaging of the aortic arch1Cedars-Sinai Medical Center, Los Angeles, CA, United States, 2University of California, Los Angeles, CA, United States, 3Xuanwu Hospital, Beijing, China, 4Guangzhou Medical University, Guangzhou, China, 5Siemens Healthineers, Los Angeles, CA, United States
Synopsis
Atherosclerotic disease of the aortic arch has been considered a potential cause of cryptogenic stroke. Vessel wall MR imaging can directly probe atherosclerotic lesions to provide
Introduction
Atherosclerotic disease of the aortic arch has been considered a potential cause of cryptogenic stroke1. Vessel wall MR imaging can directly probe atherosclerotic lesions to provide the assessment of plaque burden and instability. However, its clinical adoption for the aortic arch is hindered primarily by long imaging time that is associated with the needs for large spatial coverage, high spatial resolution, compensation of motion, and multiple image contrasts. Several 3D aortic wall MR techniques have been developed to enable more efficient acquisition, compared to 2D imaging methods, but are still limited in meeting all above clinical needs2,3. In this work, we proposed a fast 3D dual-contrast vessel wall MR technique that is potentially useful for detecting intraplaque hemorrhage and calcification as well as measuring plaque burden at the aortic arch.Methods
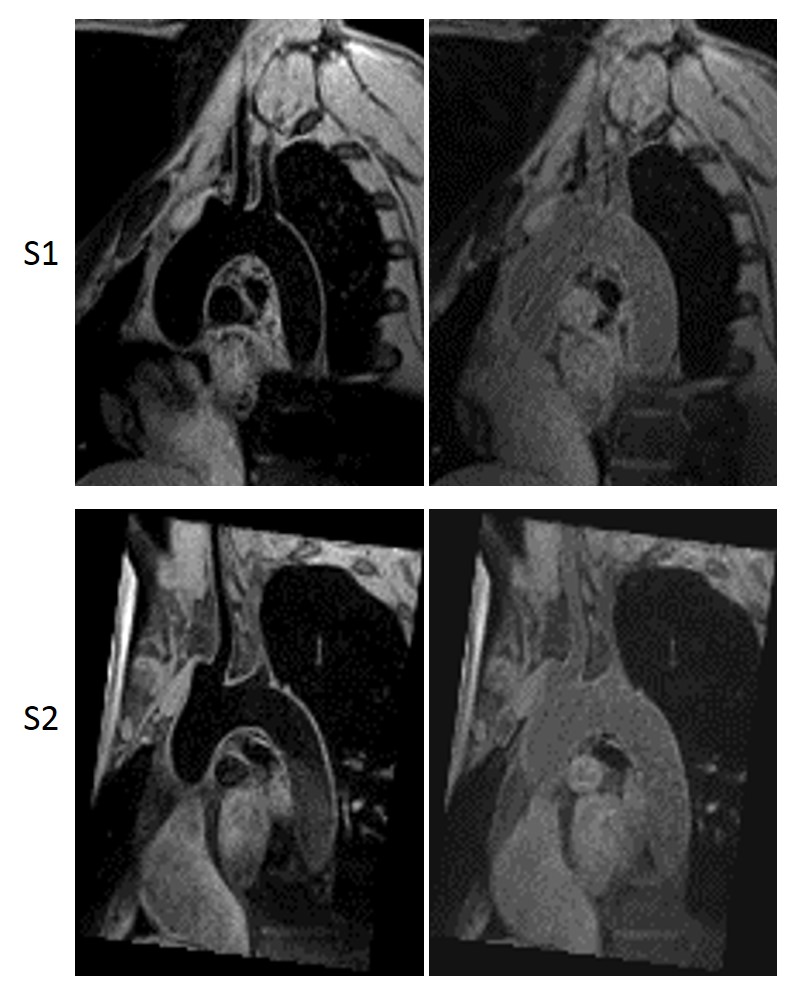
The technique acquires T1-weighted dark-blood and gray-blood data in consecutive heartbeats. At the beginning (i.e. R wave) of the first heartbeat, the blood in the left ventricle is inverted with a localized inversion preparation. During the subsequent approach to the nulling point, the blood spins are distributed in the ascending aorta (AAo), aortic arch (AAr), and proximal descending aorta (DAo). Dark blood images are then acquired at the aortic arch quiescent phase as determined from cine imaging. Gray-blood images are acquired at the same phase during the second heartbeat. To improve navigator efficiency, two independent respiratory navigators are used for the interleaved acquisition4.
Seven healthy volunteers (2F/5M, aged 22-61 y) were scanned on a 3T system (MAGNETOM Verio, Siemens) equipped with a 32-channel cardiac coil. Major imaging parameters for 3D dual-contrast imaging were: FLASH readout, candy-cane orientation, FOV 216×152×54 mm3, isotropic spatial resolution 1.23 mm, flip angle 10o, parallel imaging GRAPPA 2, 34 or 52 segments/heartbeat, navigator acceptance window ±3.5 mm. Six of the 7 volunteers also underwent 2D single slice T1-weighted TSE imaging for comparison. A 3-mm-thick cross-sectional slice reformatted from the 3D scan was imaged with spatial resolution and thickness matched and without parallel imaging. The contrast-to-noise ratio (CNR) between the vessel wall and lumen was measured for AAo, AAr, and DAo, respectively, on 3D images. On paired aortic wall images obtained from 2D and 3D scans, the lumen and wall area and their signal intensity were quantified. Wall-lumen contrast ratio was calculated as the difference between wall signal and lumen signal divided by lumen signal.
Results
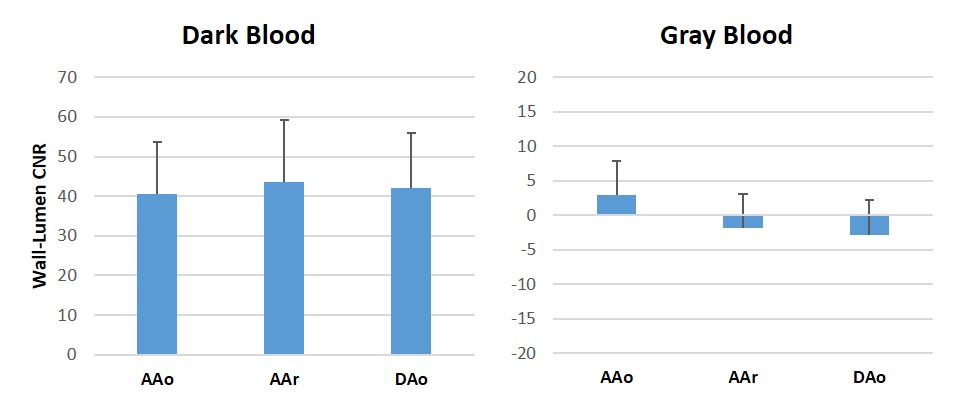
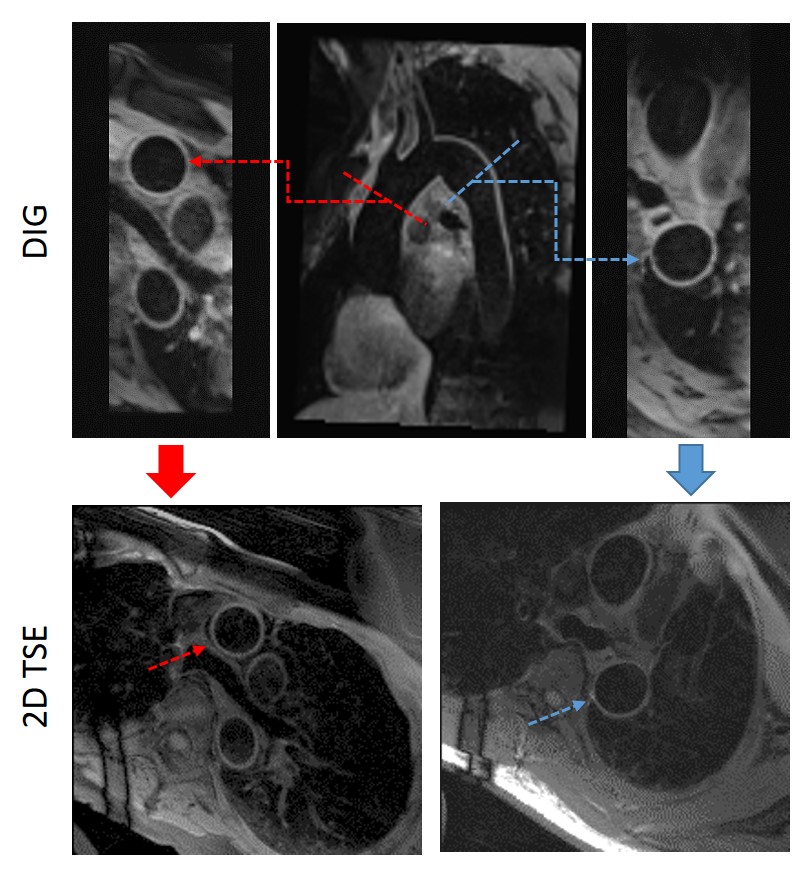
Spatially co-registered dual-contrast images were successfully acquired in all 7 subjects with the 3D dual-contrast imaging technique. Scan time ranged from 4:36 to 7:59 min, depending on breathing patterns. On dark-blood images, blood signals were adequately suppressed in AAo, AAr, and proximal DAo (Figure 1), resulting in wall-lumen CNR of 40.65±13.12, 43.55±15.67, and 42.05±13.93, respectively (Figure 2). Neutral contrast between the vessel wall and lumen was obtained on gray-blood images, resulting in wall-lumen CNR of 2.88±4.41, -1.90±8.65, -2.84±11.73 at the three segments (Figure 2). 2D TSE was successful in 5 subjects. The dark-blood images from 3D imaging were generally better than 2D TSE images in terms of wall delineation quality (Figure 3). The 3D and 2D scans provided comparable lumen (4.73±1.00 cm2 vs. 4.74±1.04 cm2) and wall area (1.66±0.19 cm2 vs. 1.62±0.13 cm2). Wall-lumen contrast ratio was significantly higher with 3D imaging (6.97±1.57 vs. 3.23±1.84, p<0.001).Conclusion
The developed 3D dual-contrast vessel wall imaging technique provides high-quality dark-blood and gray-blood vessel wall images for the aortic arch within clinically acceptable scan times. Dark-blood images are shown to be capable of quantifying vessel wall morphology. Gray-blood images, as shown in literature5, are expected to facilitate identification of superficial calcification in atherosclerotic plaques, but await validation in the patient population.Acknowledgements
No acknowledgement found.References
1. Amarenco P, Duyckaerts C, Tzourio C, et al. The prevalence of ulcerated plaques in the aortic-arch in patients with stroke. New Engl J Med. 1992;326:221-225.
2. Zhou C, Qiao H, He L, et al. Characterization of atherosclerotic disease in thoracic aorta: a 3D multicontrast vessel wall imaging study. Eur J Radiol 2016;85:2030-2035.
3. Mihai G, Varghese J, Lu B, et al. Reproducibility of thoracic and abdominal aortic wall measurements with three-dimensional, variable flip angle MRI. J Magn Reson Imaging 2015;41:202-212.
4. Xie G, Bi X, Liu J, et al. Three-dimensional coronary dark-blood interleaved with gray-blood (cDIG) magnetic resonance imaging at 3 Tesla. Magn Reson Med 2016;75:997-1007.
5. Koktzoglou. Gray blood magnetic resonance for carotid wall imaging and visualization of deep-seated and superficial vascular calcification. Magn Reson Med 2013;70:75-85.
Figures