3456
Regional distribution of Local 3D Pulse Wave Velocity with and without Aortic Arch Replacement in Pediatric Patients with Single VentricleAmol S. Pednekar1, Matthew Goette1, Prakash Masand1, and Cory Noel2
1Radiology, Texas Children's Hospital, Houston, TX, United States, 2Cardiology, Texas Children's Hospital, Houston, TX, United States
Synopsis
PC-CMR permits precise discrete 3D aortic pulse wave velocity (PWV) measurements as a surrogate for changes in vascular stiffness and ventricular-vascular interaction. In this preliminary study, global PWVs are 50% higher in 3 single ventricle (SV) patients with reconstructed arch (RA) than 3 patients with native arch (NA). Furthermore, the regional distribution of PWVs in SV-RA indicates rapid deceleration (50-70%) from proximal to distal aorta that is absent in SV-NA. The abnormal shape, large caliber change, and prosthetic material of reconstructed aortas may be additional explanatory variables. Regional distribution of local PWVs could potentially predict development of abnormal ventricular-vascular interaction.
PURPOSE
Simultaneous 3D measurement of aortic wall morphology and 3D flow vector in synchronization with cardiac cycle using phase contrast MR allows precise measurement of systolic pulse wave velocity (PWV) without assumptions of the tortuosity of the aorta. The discrete 3D aortic PWV measurements can serve as a surrogate for changes in vascular stiffness and ventricular-vascular interaction. The purpose of this preliminary study was to investigate the differences in global aortic PWV and regional distribution of local PWVs in single ventricle congenital heart disease patients with and without arch reconstruction.BACKGROUND
The aorta plays an obvious and vital role in the cardiovascular system. Important physical properties of the aorta include shape, stiffness, and distensibility, which all play a role in optimal ventricular-vascular interaction. There is great interest in understanding these aortic properties in patients with the single ventricle-type congenital heart disease due to the abnormality of the aortic root and arch and the potential role that aortic arch reconstruction plays in ventricular dysfunction [1]. One measure of arterial stiffness is the pulse wave velocity (PWV), which is also a predictor of cardiovascular mortality. The abnormal shape and caliber change of the reconstructed aorta post palliation surgery along with prosthetic material used in reconstructed aorta may contribute for the changes in regional distribution of PWV in single ventricle patients and could potentially predict development of abnormal ventricular-vascular interaction.METHODS
Three patients with single right ventricle (SRV) with native arch (ascending aortic diameter z-scores of 2.6 – 2.9) and three single ventricle patients (2 SRV, 1 left RV with ascending aortic diameter z-scores of 4.7 – 5.2) with reconstructed arch (age range, 11-18 years) were assessed for PWV. Cardiac phase resolved phase-contrast (PC) sequence with velocity encoding in three orthogonal directions (RL, FH, AP with uniform Venc) with 3D slab excitation, retrospective cardiac gating, and RF navigator gate and track technique was used. This prospective study has been approved by IRB and consent forms were obtained before all studies. All MR studies were performed on a Philips Ingenia 1.5T scanner. The 4D PC cine sequence covered the aorta from root to descending aorta with TR/TE/FA, 4.8ms/2.8ms/12o; acquired voxel size, 2x2x2 mm3; cardiac phases, 15-20 (40-50ms temporal resolution), SENSE acceleration factors, 2AP x 2RL. CMR experienced cardiologist measured the local PWVs in following sections: 1. ascending aorta (AAo) to distal transverse arch (DTA), 2. DTA to isthmus (Isth), 3. Isth to descending aorta (DAo), and 4. global PWV from AAo to DAo. The automatic 3D segmentation of the aorta and PWV calculations using 3D centerline of the segmented aorta were performed using CAAS MR 4D Flow, Pie Medical Imaging (Fig 1).RESULTS
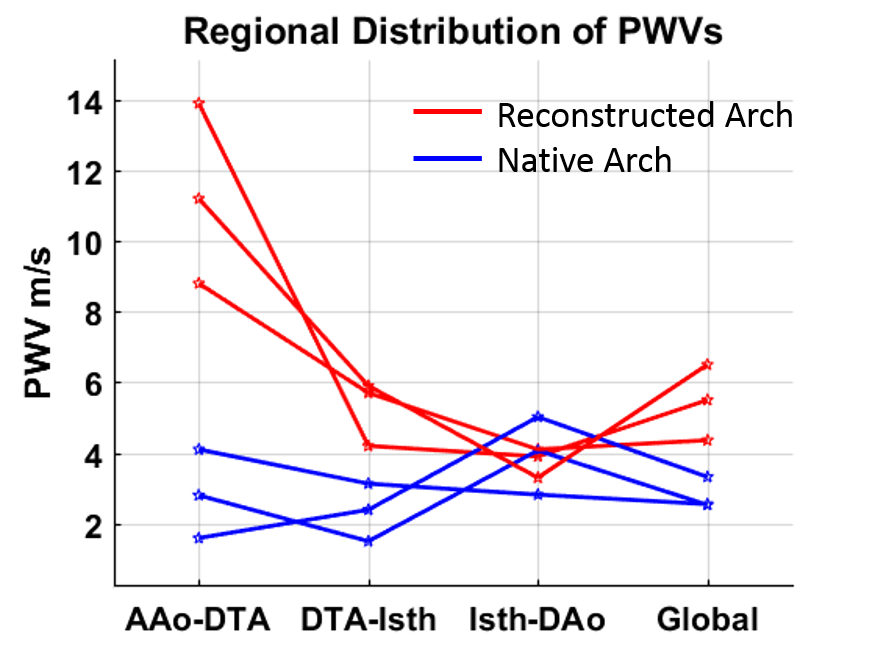
The single ventricle subjects with reconstructed arch have higher global PWV (4.36 to 6.5 m/s) compared to patients with native arch (2.53 to 3.32 m/s) (Fig 2). The local PWV in AAo-DTA section for patients with reconstructed arch (8.8-13.9 m/s) were more than double the corresponding PWVs in patients with native arch (1.59-4.1 m/s). The difference in PWVs in DTA-Isth section was also much higher than differences in global PWV, (4.2-5.9 m/s) with reconstructed arch vs. (1.5-3.13 m/s) with native arch. The PWVs in the Isth-DAo section were comparable with reconstructed arch (3.3-4.1 m/s) and native arch (2.82-5.02 m/s).CONCLUSION
The regional distribution of aortic pulse wave velocity in single ventricle patients indicates rapid deceleration (50-70%) from proximal to distal aorta. The abnormal shape, large caliber change, and prosthetic material of the reconstructed aortas may be additional explanatory variables for the differences in regional distribution of local PWVs. Regional distribution of local PWVs could potentially predict development of abnormal ventricular-vascular interaction.Acknowledgements
No acknowledgement found.References
[1] The PWV increase in SRV indicates the adverse aortic condition and function.Figures
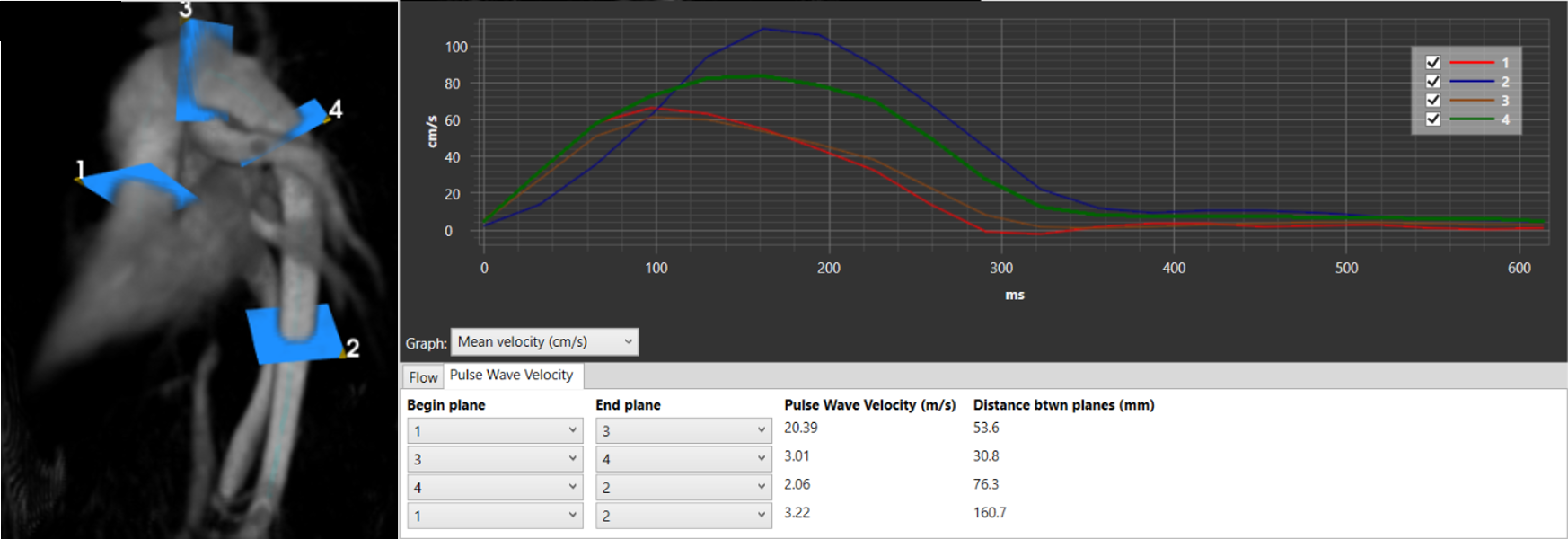
Representative image
of the local and global pulse wave velocity measurements in single ventricle
patient with reconstructed arch.
Local aortic pulse
wave velocities in sections: 1. ascending aorta (AAo) to distal transverse arch
(DTA), 2. DTA to isthmus (Isth), 3. Isth to descending aorta (DAo), and 4. global
PWV from AAo to DAo.