3452
Effect of gravity on inferior vena cava and abdominal aortic flow: evaluation using multi-posture MRI1Kanazawa University Graduate School of Medical Sciences, Kanazawa, Japan
Synopsis
Inferior vena cava flow (IVCF) and abdominal aortic flow (AAF) are seems to be affected by gravity, ie., it depends on the body posture. We validated the effect of gravity on IVCF and AAF in supine and upright positions using an original multi-posture MRI. IVCF/AAF mean velocity, IVCF/AAF maximum velocity, mean IVCF/AAF, maximum IVCF/AAF in the upright position were significantly lower than those in the supine position. The cross-sectional area of IVC was significantly lower than those in the supine position, but that of AA was not significantly changed. Both IVCF and AAF decrease in the upright position.
Purpose
Inferior vena cava flow (IVCF) and abdominal aortic flow (AAF) are essential factors of the systemic circulation.1 Although postural changes might alter IVCF and AAF by the gravity effect, the exact details are unknown. This study aimed to evaluate the differences of IVCF and AAF in the supine and upright positions of healthy volunteers, using an original magnetic resonance imaging (MRI) system that can obtain images in any posture (multi-posture MRI).2 Materials and Methods
We
obtained caval velocity-mapped images with ECG-triggered cine phase-contrast
technique using multi-posture MRI (N = 12) in the supine and upright positions,
and determined mean IVCF and AAF velocities in the region of interest in each
cardiac phase. In addition, we obtained flow curves in the cardiac cycle from
the IVCF and AAF velocity multiplied by each cross-sectional area. We assessed
the mean IVC velocity (IVC-Vmean), the maximum IVC velocity (IVC-Vmax), the
mean IVCF (IVCFmean), the maximum IVCF (IVCFmax), and the cross-sectional area
of the inferior vena cava (IVC-CA) in the supine and upright positions. We also
assessed the mean AA velocity (AA-Vmean), the maximum AA velocity (AA-Vmax),
the mean AAF (AAFmean), the maximum AAF (AAFmax), and the cross-sectional area
of the abdominal aorta (AA-CA) in the supine and upright positions. Further, we
assessed heart rates in the supine and upright positions.Materials and Methods
Results and Discussion
The
IVC-Vmean in the upright position (1.62 ± 1.03 cm/s) was significantly lower
than that in the supine position (9.55 ± 5.03 cm/s; P = 0.002)(Fig. 2a), the IVC-Vmax in the upright position (2.1 ±
0.93 cm/s) was significantly lower than that in the supine position (14.6 ±
5.66 cm/s; P = 0.002)(Fig. 2b), the
IVCFmean in the upright position (165 ± 109 mL/min) was significantly lower
than that in the supine position (1403 ± 534 mL/min; P = 0.002)(Fig. 2c), the IVCFmax in the upright position (23.4 ±
10.2 mL/min) was significantly lower than that in the supine position (249 ±
94.1 mL/min; P = 0.002)(Fig. 2d), and
the mean IVC-CA in the upright position (211 ± 115 mm2) was significantly lower
than that in the supine position (342 ± 203 mm2; P = 0.008)(Fig. 2e).
The
AA-Vmean in the upright position (2.10 ± 0.79cm/s) was significantly lower than
that in the supine position (6.71 ± 2.30 cm/s; P = 0.002)(Fig. 3a), the AA-Vmax in the upright position (5.22 ±
2.39 cm/s) was significantly lower than that in the supine position (17.9 ±
6.52 cm/s; P = 0.002)(Fig.3b), the
AAFmean in the upright position (241 ± 113 mL/min) was significantly lower than
that in the supine position (699 ± 306 mL/min; P = 0.002)(Fig. 3c), and the AAFmax in the upright position (572 ±
303 mL/min) was significantly lower than that in the supine position (1823 ±
630 mL/min; P = 0.003)(Fig. 3d).
However, no significant difference was observed between the upright position
and the supine position in terms of the mean AA-CA (184 ± 50.1 mm2 and 175 ±
43.6 mm2, respectively; P = 0.583)(Fig.
3e). The heart rate in the upright position (85 ± 7.4 times/s) was
significantly higher than that in the supine position (73 ± 6.9 times/sec; P = 0.002) (Fig. 4). The findings of
this study indicate that gravity reduces IVCF and AAF, despite autoregulation.Results and Discussion
Conclusion
Both
IVCF and AAF decrease in the upright position. Multi-posture MRI makes it
possible to evaluate the effect of gravity on systemic circulation.Conclusion
Acknowledgements
No acknowledgement found.References
1. W. F. Ganong. Review of Medical Physiology 22nd edition. NY, McGraw-Hill Companies; 2005
2. Ohno N, Miyati T, Hiramatsu Y, Yamasaki M. Quantitation of Venous Blood Flow in Gravity MRI: A Phantom Study. Med Imag & Info Sci 2017;in press
Figures

Fig. 1
Caval velocity-mapped images were obtained with ECG-triggered cine phase-contrast technique in the supine position and upright position using multi-posture MRI.
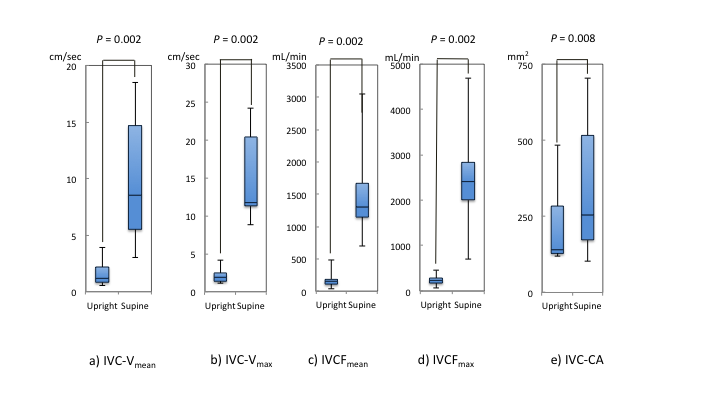
Fig. 2
a) The IVC-Vmean in the upright position was significantly lower than that in the supine position (P = 0.002). b) The IVC-Vmax in the upright position was significantly lower than that in the supine position (P = 0.002). c) The IVCFmean in the upright position was significantly lower than that in the supine position (P = 0.002). d) The IVCFmax in the upright position was significantly lower than that in the supine position (P = 0.002). e) The mean IVC-CA in the upright position was significantly lower than that in the supine position (P = 0.008).
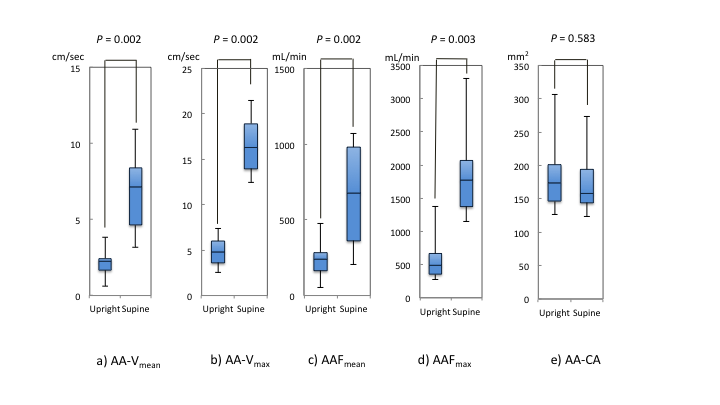
Fig. 3
a) The AA-Vmean in the upright position was significantly lower than that in the supine position (P = 0.002). b) The AA-Vmax in the upright position was significantly lower than that in the supine position (P = 0.002). c) The AAFmean in the upright position was significantly lower than that in the supine position (P = 0.002). d) The AAFmax in the upright position was significantly lower than that in the supine position (P = 0.003). e) No significant difference was observed between the upright position and the supine position in terms of the mean AA-CA (P = 0.583).
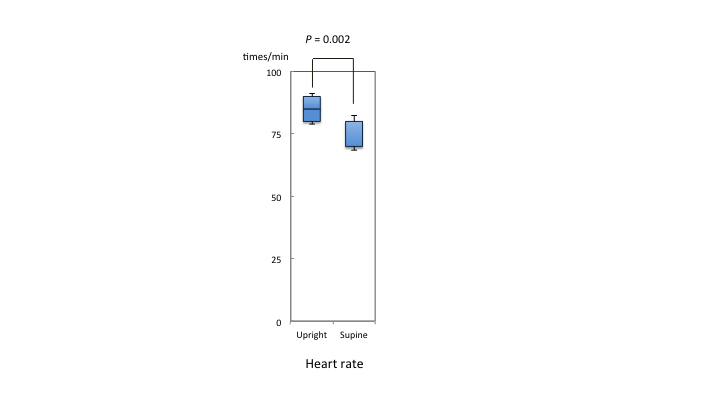
Fig. 4
The heart rate in the upright position was significantly higher than that in the supine position (P = 0.002).