3449
Vortex Flow in Left Ventricle Interrupts Efficient Ejection: Demonstration by Vortex Flow Map of Cardiac Cine Magnetic Resonance ImagingMasateru Kawakubo1, Kenji Fukushima2, Risako Nakao3, Eri Watanabe3, Yamato Shimomiya4, Yasuhiro Goto5, Hitoshi Tadenuma5, Masami Yoneyama6, and Michinobu Nagao2
1Department of Health Sciences, Faculty of Medical Sciences, Kyushu University, Fukuoka, Japan, 2Department of Diagnostic Imaging & Nuclear Medicine, Tokyo Women’s Medical University, Tokyo, Japan, 3Department of Cardiology, The Heart Institute of Japan, Tokyo Women’s Medical University, Tokyo, Japan, 4Clinical Application Development Marketing Division, Ziosoft Inc., Tokyo, Japan, 5Department of Radiological Service, Tokyo Women’s Medical University, Tokyo, Japan, 6Philips Electronics Japan, Ltd., Tokyo, Japan
Synopsis
Quantitative characterization of vortex flow might be a novel objective tool for evaluating left ventricular (LV) function. We developed the novel technique of vortex flow map (VFM). The VFM based on MR feature tracking can calculate the temporal displacement of the pixels on standard cine MRI. In this study, we analyzed the association with the VFM in LV and ejection fraction. As a result, it is indicated that the strong 3-dimensional vortex flow appears and impairs efficient LV ejection in severe heart failure. And the VFM is a useful tool for the evaluation of the efficiency of LV ejection.
Purpose
Vortex formation within the left ventricular (LV) blood flow contribute to efficient blood pumping function. Quantitative characterization of vortex flow might be a novel objective tool for evaluating LV function1. Recently, further development of the phase contrast (PC) magnetic resonance imaging (MRI) technique allows evaluation of 3-dimensional (3D) blood flow; this is often referred to as “4D-Flow MRI” and provides information on 3D blood flow, with full volumetric coverage of any cardiovascular region of interest2, 3. However, there are some limitation for using 4D-Flow MRI in clinical examination such as long data acquisition time, special MR sequence as the 3D PC, and complex post image procession. Therefore, the easier analytical method is needed to quantify the vortex blood flow. Recently, we developed the novel technique named vortex flow map (VFM). The VFM based on MR feature tracking can calculate the temporal displacement of the pixels in the region of interest (ROI) determined on standard cine MRI4. In this study, we analyzed the association with geometrical vortex flow in LV and ejection fraction (EF) using the VFM.Methods
Fifty-eight patients with non-ischemic cardiomyopathy who underwent cardiac MR examination were retrospectively enrolled (48±18 years old, 41 male). All cine images were obtained by steady state free precessions sequence with short-axis (SA), four-chamber (4CH), and two-chamber (2CH) orientations. The patients were divided into 2 groups as the patients with LVEF <25 % and the patients with LVEF ≧25 %. The quantification of vortex flow is based on MR feature tracking technique. Firstly, the regions of LV are manually determined in SA, 4CH, and 2Ch orientations at the end-diastolic phase. The pixels in ROI are automatically tracked for a cardiac cycle with MR feature tracking (Fig. 1a). Secondly, the vector of displacement of all pixels is decomposed into circumferential and radial components (Fig. 1b). Finally, magnitude vector flow (MVF) is calculated as the maximum percentage of the absolutely displacement for a cardiac cycle. The indices of circumferential MVF (MVFCC) and radial MVF (MVFRad) were defined. In the statistically analysis, the MVFs were compared between the 2 patient groups by Mann-Whitney U test. The MVFs were multiply compared between SA, 4CH, and 2CH orientations by Steel-Dwass test.Results
As shown in Figure 2, the MVFCC in the patients with LVEF <25 % were significantly greater than those with LVEF ≧25 % in the SA and 4CH orientations (SA: 7.4±5.3 vs. 4.5±5.3, P <0.05, 4CH: 10.9±13.4 vs. 4.2±3.4, P <0.05). The MVFCC with 2CH orientation was significantly greater than in other orientations in the patients with LVEF ≧25 % (SA: 4.5±5.3, 4CH; 4.2±3.4, and 2CH: 7.9±3.9, P <0.05) (Fig. 3).Discussion
Strong circumferential vector flow in the SA and 4CH orientation in the patients with severe LV dysfunction (LVEF < 25 %). Our result indicates that large 3D circumferential vortex flow appears and impairs efficient LV ejection. Figure 4 represents the vortex flow in the patient with and without LV dysfunction. The strong vortex flows were observed in the patients with LV dysfunction. In only 2CH orientation, the MVFCC is equivalent between the two groups. On the other hand, our result demonstrated significantly large MVFCC with the 2CH orientation than with the SA and 4CH orientations in the patients with LVEF ≧25 %. These results agree with previous report that the strong longitudinal vortex flow in the patients with preserved LV function5. Therefore, the MVF with MR VFM can be useful clinical index for evaluating vortex blood flow.Conclusion
There are two findings in this study. One is strong 3D vortex flow appears and impairs efficient LV ejection in severe heart failure. The other is the VFM can be a useful tool for the evaluation of LV function and the efficiency of LV ejection.Acknowledgements
No acknowledgement found.References
- Kheradvar A, Pedrizzetti G. Vortex formation in the heart. In: Vortex formation in the cardiovascular system. London: Springer; 2012: 45–53.
- Stankovic Z, Allen BD, Garcia J, et al. 4D-flow imaging with MRI. Cardiovasc Diagn Ther: 2014: 4: 173-192.
- Elbaz MS, Calkoen EE, Westenberg JJ, et al. Vortex flow during early and late left ventricular filling in normal subjects: quantitative characterization using retrospectively-gated 4D flow cardiovascular magnetic resonance and three-dimensional vortex core analysis. J Cardiovasc Magn Reson: 2014: 16:78.
- Kawakubo M, Nagao M, Kumazawa S, et al. Evaluation of ventricular dysfunction using semi-automatic longitudinal strain analysis of four-chamber cine MR imaging. Int J Cardiovasc Imaging 2016; 32 (2): 283-9.
- Suwa K, Saitoh T, Takehara Y, et al. Intra-left ventricular flow dynamics in patients with preserved and impaired left ventricular function: Analysis with 3D cine phase contrast MRI (4D-Flow). J Magn Reson Imaging 2016; 44 (6): 1493-1503.
Figures
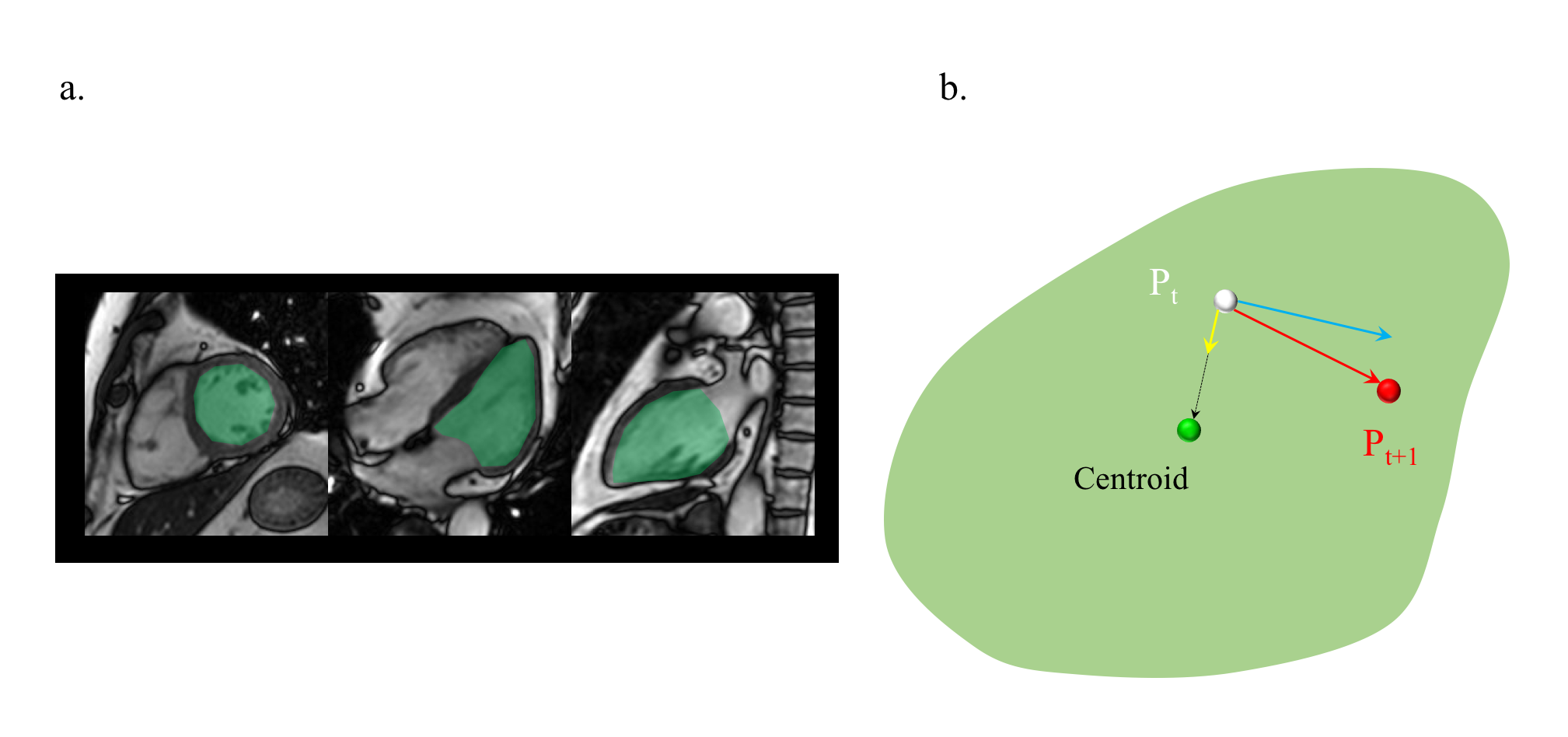
a: The LV areas are manually determined in SA, 2CH, and 4CH
orientations (green area).
b: Vector of the displacement
of all pixels in the area (red arrow) are decomposed into circumferential
component (blue arrow) and radial component (yellow arrow). Green point is
indicated the centroid of LV area.
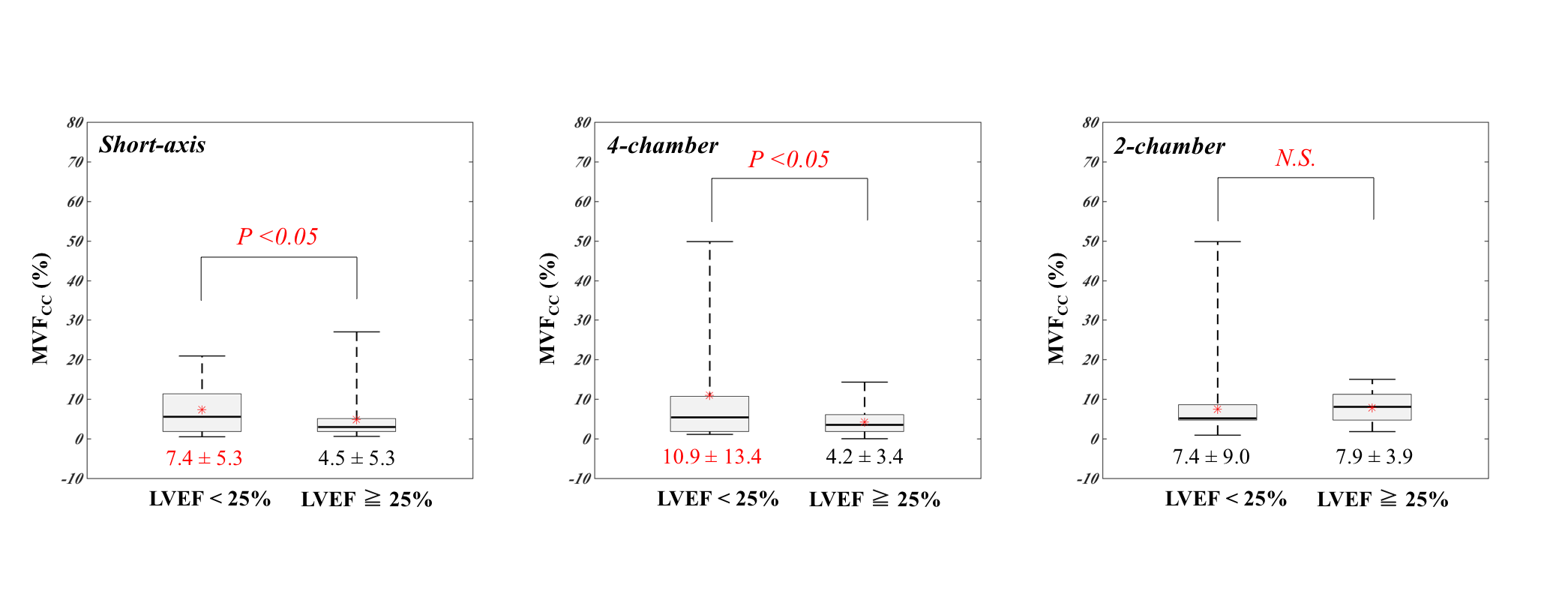
Comparison of the circumferential
MVF in the SA, 4CH, and 2CH orientations are shown. Significantly large MVFs
are observed in the SA and 4CH orientations. In 2CH orientation, the MVFCC
is equivalent between the two groups.
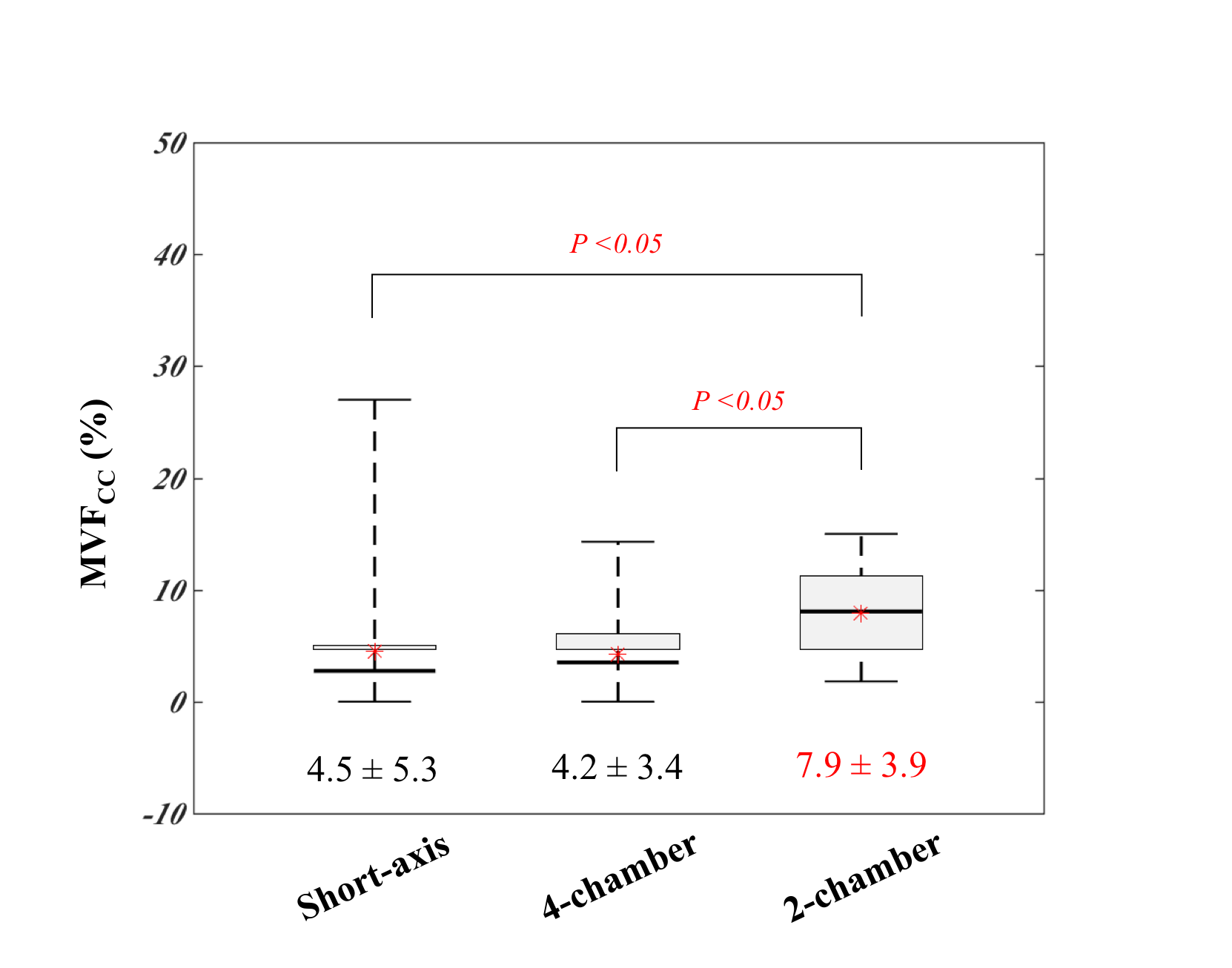
Multiply comparison of the circumferential
MVF in the patients with LV ≧25% between the SA, 4CH, and 2CH orientations are
shown. The MVFCC was significantly greater in 2CH orientation than those in SA and
4CH orientations.
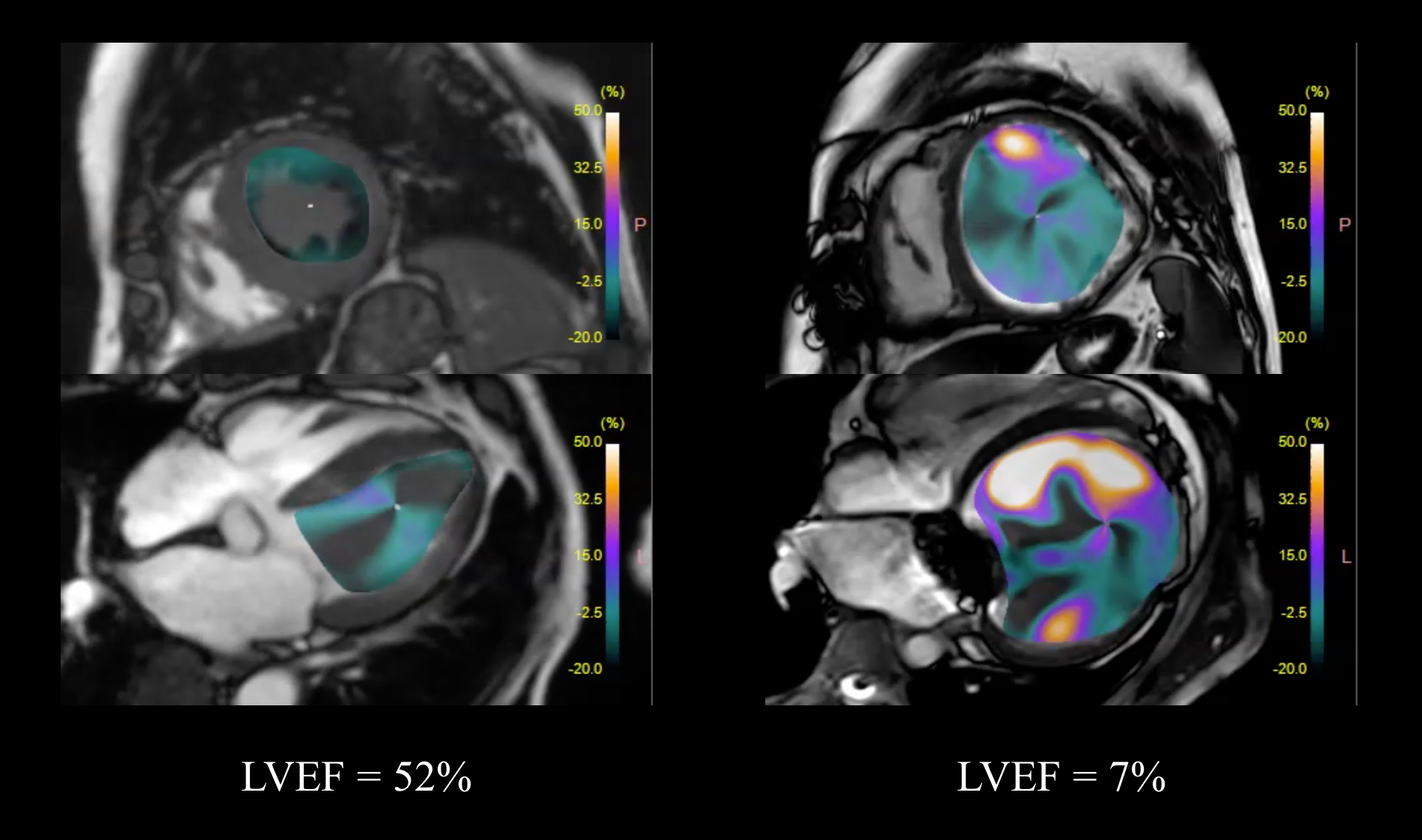
Representative
cases of the vortex flow in the patient with and without LV dysfunction are
shown. The strong vortex flows were observed in the patients with LV
dysfunction (right: LVEF = 7%).