3444
Evaluation of aortic viscous energy loss, kinetic energy and association with pumping function in congenital patients with transposition of great arteries using time-varying aortic geometry: Volumetric 4D Flow MRI Analysis1Pediatric Cardiology, Leiden University Madical Ceneter, Leiden, Netherlands, 2Radiology, Leiden Univeristy Medical Center, Leiden, Netherlands
Synopsis
Aortic hemodynamic energetics including kinetic energy (KE) and non-turbulent viscous energy loss (EL) and the association with cardiac function were evaluated in 8 TGA patients after arterial switch operation (ASO) and in 8 healthy individuals by 4D flow MRI. EL was significantly increased in TGA compared to healthy volunteers and aortic regions of highest levels indicate influence of complex ASO-related aortic geometry on blood flow efficiency. Significant positive correlation between aortic EL and cardiac index was found. Understanding the impact of ASO on aortic blood flow efficiency might enable insights on ways to improve operative procedure for TGA in future.
INTRODUCTION:
Patients with transposition of great arteries (TGA), currently undergo arterial switch operation (ASO) at neonatal age. The ASO with Lecompte procedure restores cardiovascular physiology at the expense of alteration of arterial geometry with the pulmonary arteries embracing the ascending aorta from anterior and a steeper angulation of the aortic arch [1, 2]. This complex geometrical setup results in altered aortic hemodynamics with aortic root dilatation as the main complication [3]. An emerging tool to evaluate blood flow efficiency is the quantification of hemodynamic energetics including kinetic energy (KE) and non-turbulent viscous energy loss (EL: amount of kinetic energy lost due to viscosity-induced forces) [4]. Using 4D Flow MRI, the aims of this study were to evaluate efficiency of blood flow energetics and the association with cardiac pumping function in TGA patients in comparison with healthy volunteers.
MATERIAL AND METHODS:
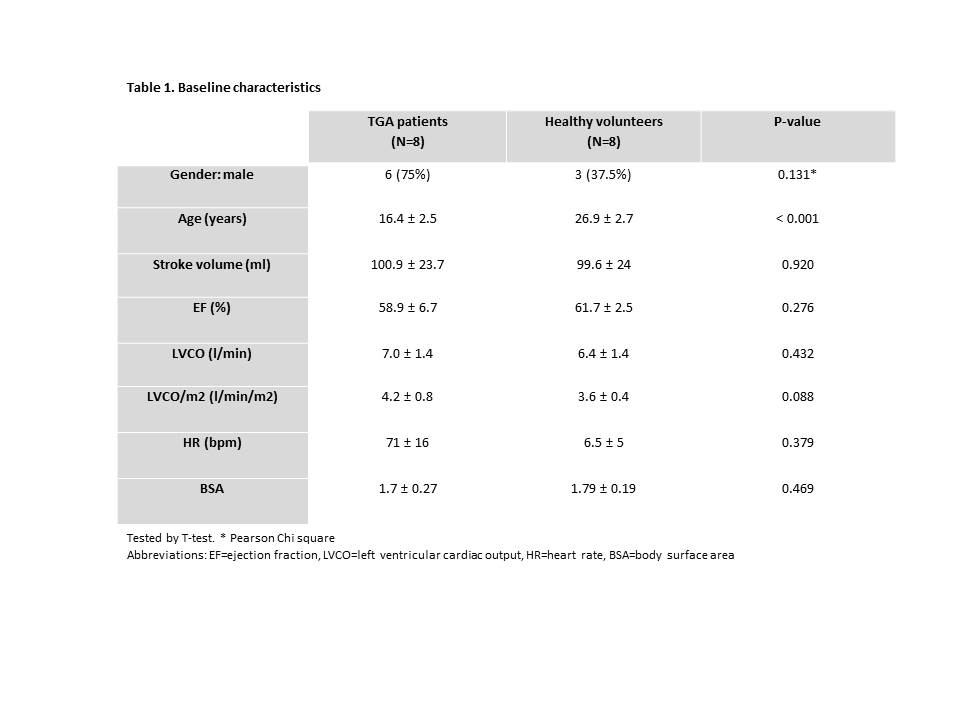
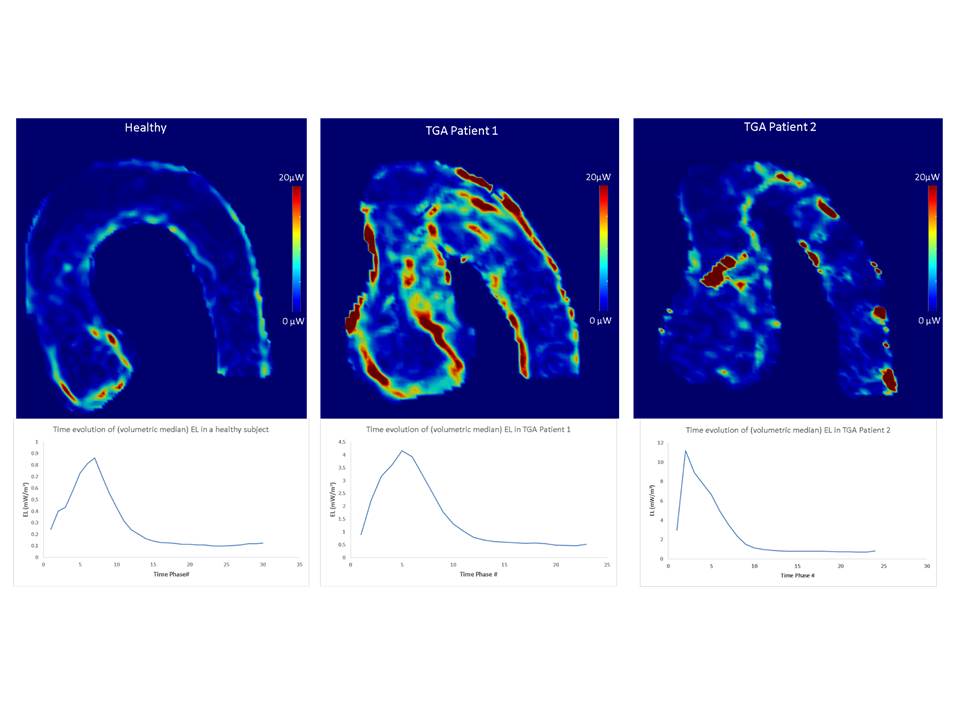
Aortic 4D flow MRI and cardiovascular MRI were performed on a 3.0 Tesla MRI scanner (Philips Healthcare) in 8 TGA (age=16.4±2.5 yrs) patients after ASO and 8 healthy volunteers (age=26.9±2.7 yrs). 4D flow MRI scan parameters were: retrospective ECG and respiratory navigator gating, spatial resolution=2.5x2.5x2.5mm3, temporal resolution=33.8-36.8ms, VENC=200-300cm/s, repetition time 4.2-4.6ms, echo time 2.4-2.7ms, flip angle 10°. In order to produce time-varying aortic geometry segmentation from 4D Flow MRI, we used a co-registration framework between cine-anatomical images (steady-state free-precession acquisition using free breathing and respiratory navigator gating) and 4D Flow MRI data to perform the segmentation. Using in-house developed software MASS, time-resolved volumetric aortic segmentation was manually performed on cine-anatomic images spanning from the aortic valve to the thoracic aorta at the level of the aortic valve. To correct potential misalignment between cine-anatomic images and 4D Flow MRI, we performed automatic rigid registration (translation+rotation) by mutual information between cine-anatomic images and 4D Flow MRI data. Registered time-resolved segmented aortic contours were then transferred to 4D Flow MRI data to provide 4D Flow MRI aortic segmentation. This time-resolved volumetric segmentation was then used to compute KE and EL using in-house Matlab based software: at each time instant t, and voxel i, voxel-wise KEi,t =1/2×rho×vi2 was computed (rho as the blood density=1.06 g/mL, v the voxel-wise velocity magnitude). Voxel-wise ELi,t = μ Pi Li, was computed , μ=0.004 Pa.s as the dynamic viscosity, Pi as the voxel-wise viscous dissipation rate per unit volume in the Navier-Stokes energy equations [4], voxel volume Li . Volumetric KE (Joule (J)) and EL (Watt (W)) were then computed as the median of all voxel-wise KEi and ELi values within the segmented volume at time t, respectively. Repeating this over all acquired time phases provide time evolution curves of KE and EL over the cardiac cycle. To account for difference in aortic size between subjects, computed parameters were normalized by instantaneous aortic volumes resulting in evolution curves of KE (J/m3) and EL (W/m3) (Figure 1). From these volume-normalized time curves, the systolic time-peak KE (KEsys-peak) and EL (ELsys-peak) were computed and compared between TGA patients and healthy volunteers (using t-test). Regional EL Maps were also computed to identify aortic regions of highest EL levels visually. To evaluate cardiac pumping function, cardiac output and cardiac index (cardiac output normalized for body surface area) were computed from the short-axis cine images of the left ventricle. Association between KE and EL with cardiac index were tested using Pearson’s correlation (P<0.05=significant).
RESULTS:
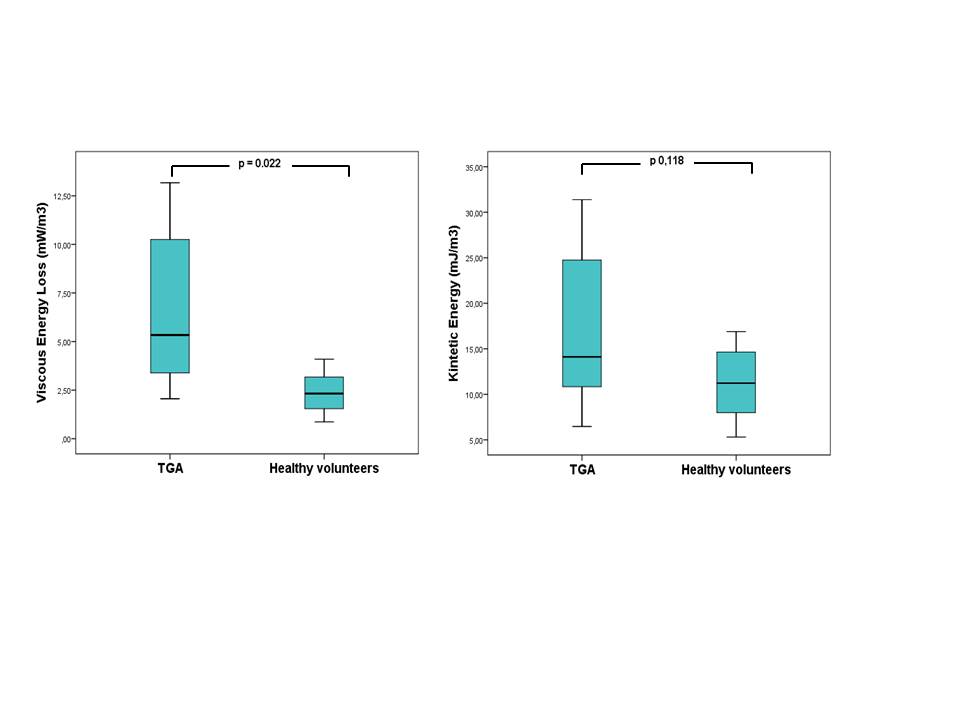
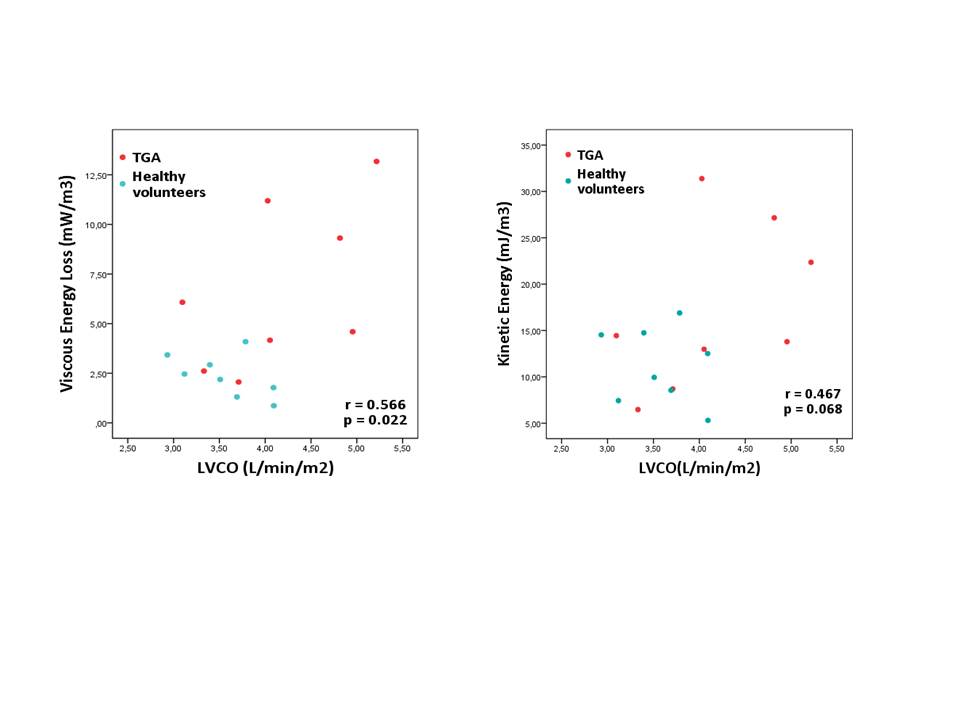
Baseline characteristics of the groups were similar except for the age (Table 1). TGA patients showed significantly higher volume-normalized median EL (ELsys-peak=6.65±4.11 vs 2.38±1.08mW/m3, p=0.02). Example time-evolution curves of volume-normalized El are provided in Figure 1. The volume-normalized median KE of the patients was not significantly different compared to the healthy volunteers (KEsys-peak=17.16±8.87 vs 11.24±4.06 mJ/m3, p=0.118) (Figure 2). A significant correlation between cardiac index and normalized EL was found for the entire population (i.e. pooled TGA patients and healthy volunteers) (Figure 3). The regions of highest EL for TGA patients were at the inner curvature of the dilated proximal ascending aorta and inner curvature of proximal descending aorta, just beyond the aortic arch (FIgure1).
DISCUSSION AND CONCLUSION:
EL is increased in the aorta of TGA patients after ASO correction as compared to healthy volunteers. A significant positive correlation is found between aortic EL and cardiac index, which might impact cardiac function in the long term. Regions of highest EL levels in TGA patients indicate influence of complex aortic geometry on blood flow efficiency. Understanding the impact of ASO on aortic blood flow efficiency might enable insights on ways to improve or guide operative procedure for TGA in the future.Acknowledgements
No acknowledgement found.References
1. Dodge-Khatami A, Mavroudis C, Mavroudis CD, Jacobs JP. Past, present, and future of the arterial switch operation: historical review. Cardiol Young. 2012 Dec;22(6):724-31.
2. Van der Bom T, Van der Palen RL, Bouma BJ, et al. Persistent neo-aortic growth during adulthood in patients after an arterial switch operation. Heart. 2014 Sep;100(17):1360-5.
3. Geiger J, Hirtler D, Bürk J, et al. Postoperative pulmonary and aortic 3D haemodynamics in patients after repair of transposition of the great arteries. Eur Radiol (2014) 24:200–208.
4. Barker AJ, Van Ooij P, Bandi K, et al. Viscous Energy Loss in the Presence of Abnormal Aortic Flow. Magn Reson Med. 2014 Sep; 72(3): 620–628.
Figures