3440
Dual-venc and single-venc 4D Flow MRI in cerebral aneurysms in comparison to image-based CFD modeling1Weldon School of Biomedical Engineering, Purdue University, West Lafayette, IN, United States, 2Radiology, Neurological Surgery and Neurology, Northwestern University, Chicago, IL, United States, 3Radiology, Northwestern University, Chicago, IL, United States, 4Biomedical Engineering, Northwestern University, Evanston, IL, United States
Synopsis
Blood flow in two cerebral aneurysms was measured with 4D Flow MRI and simulated with image-based Computational Fluid Dynamics (CFD). A dual-venc 4D Flow MRI sequence with a shared reference scan was used in addition to a standard, single-venc 4D Flow acquisition in order to improve the dynamic range of measured velocities. Comparison of the MRI-measured and CFD-simulated flow fields showed that the 4D Flow and CFD methods can complement each other by eliminating modeling errors and augmenting imaging resolution. The dual-venc 4D Flow MRI provided valuable information on recirculating flow patterns that was not available from the single-venc data.
Introduction:
4D Flow MRI is capable of measuring time-resolved, 3D velocity fields in cerebral arteries. Hemodynamic forces have been shown to affect the stability and progression of cerebral aneurysms1. The assessment of relevant flow metrics from 4D Flow MRI may be inaccurate due to limited spatiotemporal resolution and the dynamic range of velocities in cerebral aneurysms. An interleaved, dual-venc 4D Flow MRI sequence with a shared reference scan allows the acquisition of 4D Flow MRI data with high dynamic range and without velocity aliasing2. Alternatively, these flow parameters may be acquired from image-based Computational Fluid Dynamics (CFD) models. While providing higher resolution, CFD relies on modeling assumptions, which may compromise the reliability of the results. In this study, we compared dual-venc 4D Flow with high-resolution CFD results in two cerebral aneurysms in order to cross-validate both approaches and determine the advantages of dual-venc 4D Flow relative to a single-venc acquisition.Methods:
Dual-venc 4D Flow MRI and a time of flight angiogram (TOF) were acquired on a 3T MRI scanner (MAGNETOM Skyra, Siemens, Germany) in two patients with cerebral aneurysms. The first patient (female, 65 yrs old) presented with a saccular anterior communicating artery (ACA, 7.2 x 8.5 mm saccular) aneurysm and the second patient (female, 60 yrs old) with a left saccular internal carotid aneurysm (ICA, 10 mm). The TOF data was segmented to form 3D surfaces corresponding to the luminal boundaries. Flow-related image artifacts were corrected by comparing TOF data to the magnitude and phase images of the 4D Flow MRI as shown in Figure 1. Numerical simulations were conducted with the solver FLUENT, using inlet velocities prescribed from the 4D Flow data. The error in velocity magnitude between CFD and 4D Flow MRI was determined by finding the percentage error taking CFD as the standard for each case. The average error with respect to all points in the region was calculated.Results:
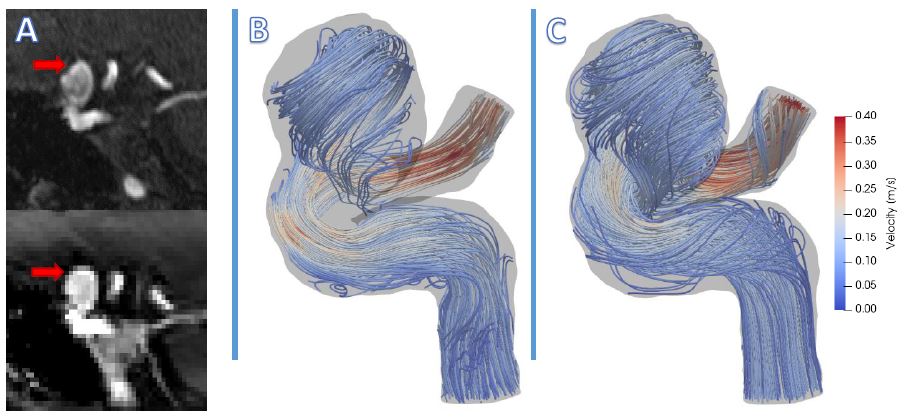
The 4D Flow and CFD results obtained for the ICA aneurysm
are shown in Figure 1. The panel (A) shows a concave shape of the aneurysmal
dome on the TOF image due to signal saturation as well as the correct, convex
dome appearing on the 4D Flow magnitude image. The flow streamlines obtained
with the dual-venc 4D Flow (B) are compared to those obtained with CFD (C). The
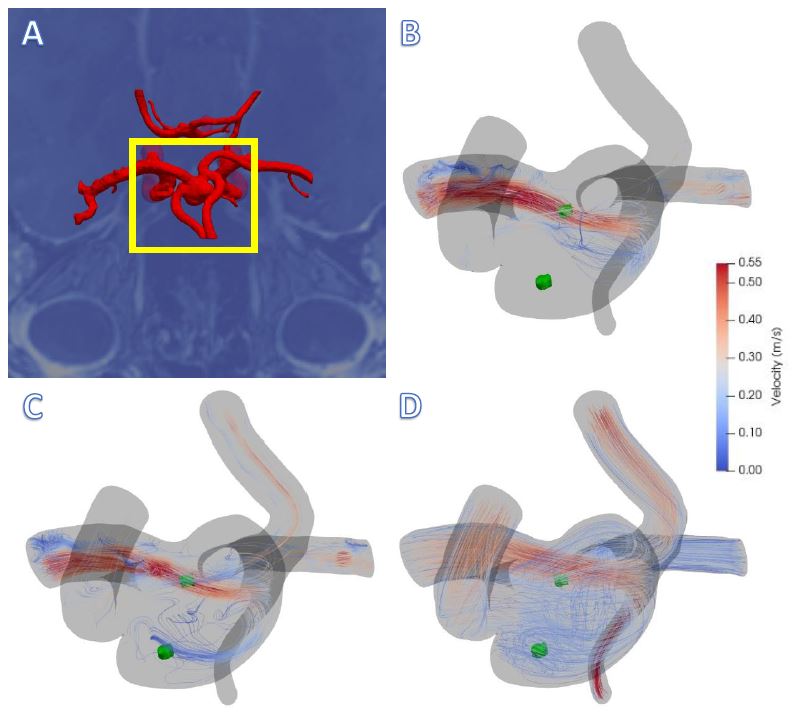
image-based model of the ACA aneurysm is shown in Figure 2(A). The flow
streamlines obtained with the single-venc (B) and dual-venc 4D Flow (C) are
compared to the CFD streamlines (D). The results show the limitation of the
single-venc 4D Flow in detecting slow, recirculating patterns in the aneurysmal
sac. The dual-venc acquisition provides more details on the complex flow
patterns, while still lacking the resolution of the CFD. Error analysis of data
for the ICA aneurysm showed a 33.90% and 11.03% difference between the
dual-venc and CFD velocities in the flow recirculation and jet regions,
respectively. For the ACA aneurysm, the velocity discrepancies between the
dual-venc and CFD were 22.42% and
37.81%, while single-venc to CFD differences at the same locations were 24.93%
and 39.16%.
Discussion:
The 4D Flow data was invaluable for correcting the segmentation errors resulting from the TOF signal loss in slow velocity zones. In addition, the 4D Flow data was crucial for prescribing patient-specific inlet flow conditions for the ACom aneurysm, where the flow rates in the supplying ACAs were markedly different. The numerical results provided information on small flow structures that were not detected with 4D Flow. A comparison of the single-venc and dual-venc 4D Flow results for the ACom aneurysm clearly demonstrate the advantages of the dual-venc acquisition in detecting these slow, recirculating flow patterns. The flow field obtained with the dual-venc captures the vortex and show the flow in the distal region of the aneurysm. The limited improvement in the percent error calculated between the CFD and single- and dual-venc 4D Flow data can be explained by averaging of the velocities interpolated on lower-resolution grid. The future work will be on quantitative comparison of velocity components and wall shear stresses obtained with each method.Conclusions:
Comparison of the flow fields simulated with CFD and measured with the single- and dual-venc 4D Flow MRI showed the advantage of the dual-venc acquisition in resolving recirculating flows in cerebral aneurysms. The study emphasized the importance of 4D Flow measurements for verification of patient-specific CFD models as well as the value of CFD for detecting small flow structures that affect hemodynamic forces acting on vessel walls.Acknowledgements
No acknowledgement found.References
[1] Boussel L, Rayz V, McCulloch C, et al. Aneurysm growth occurs at region of low wall shear stress: patient-specific correlation of hemodynamics and growth in a longitudinal study. Stroke. 2008;39(11):2997-3002.
[2] Schnell S, Ansari S A, et al.
Accelerated dual-venc 4D flow MRI for neurovascular applications. J Magn Reson
Imaging. 2017;46(1):102-114.
Figures