3438
Feasibility of 4D phase-contrast MRI for the assessment of blood flow in the fetal aorta using Doppler ultrasound gating: preliminary results1Department of Diagnostic and Interventional Radiology and Nuclear Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 2Department of Radiology, University Hospital Cologne, Cologne, Germany, 3Lund University, Lund, Sweden, 4University Medical Center Hamburg-Eppendorf, Hamburg, Germany
Synopsis
Fetal magnetic resonance imaging (MRI) is increasingly used as a second-line imaging tool for prenatal evaluation. The recet Doppler ultrasound trigger method enables the use of cardiovascular imaging techniques which may be usefull to improve prenatal cardiovascular imaging. This work investigates the use of 4D phase contrast measurements for the visualisation and quantification of fetal blood flow in the great vessels. In a small study group (n=2) it was shown for the first time that 4D flow measurements are feasible in the fetal vessels which may be beneficial for visualization and quantification of complex congenital cardiovascular malformations.
Introduction
Methods
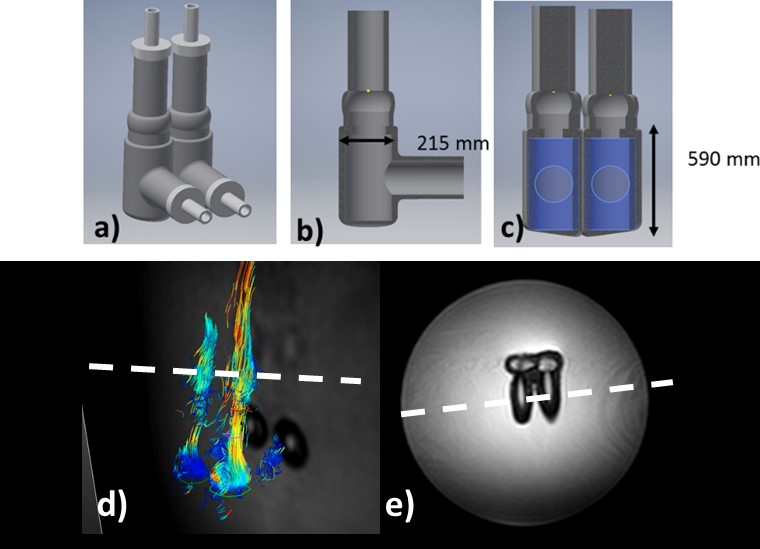
Prior to fetal MRI, the 4D phase contrast sequence was first
evaluated for vessel sizes similar to fetal vessels using a self-manufactured
fetal cardiac phantom based on a simplified biventricular design (Figure 1).
The anatomical dimensions were based on literature values of a 36 week old
fetus with a right and left ventricular diameter of 215 mm and height of 590 mm.
An external pump simulated a constant heart motion and a trigger signal of 130
BPM. The possibility to measure flow within the phantom using the 4D phase
contrast sequence (pixel spacing = 1.04 x 1.04 x 2.50 mm, slice thickness = 5
mm, TR/TE: 3.0/2 msec, FA: 6.5°, SENSE = 2, FoV = 300 x 300 x 50 mm, Phases= 10)
was evaluated using a standard 2D cine phase contrast sequence (pixel spacing =
1.2 x 1.2 mm2, TR/TE: 4.2/2.6 msec, FA: 10°, slice thickness: 8 mm,
VENC: 160 cm/s, phases: 25). All measurements (i.e. phantom and human subject) were
performed on a 1.5T MRI (Achieva, Philips Healthcare, Best, The Netherlands). Following
phantom measurements, the feasibility to acquire a 4D dataset of the fetal
heart and great vessels was evaluated in two fetuses (Gestation week 33 and
35). For required cardiac gating a recently developed MRI compatible Doppler
Ultrasound (DUS) device (northh medical GmbH, Hamburg, Germany) was used. The
device records the fetal heart rate and processes the signal into a gating
signal that is fed into the physiologic unit of the MRI. As fetal motion cannot
be avoided, only 10 heart phases were acquired to minimize imaging time,
resulting in a temporal resolution of ca. 40 ms and scan time of 2.30min. Morphologic
images of the aorta and fetal heart for planning and orientation were acquired
using a retrospectively gated cine balanced steady-state free precession
sequences (pixel spacing = 1.0 x 1.0 mm2, slice thickness = 5 mm, TR/TE:
5.0/1.6 msec, FA: 60°, SENSE = 2, matrix = 288 x 288, Phases= 20). For
verification the 2D cine phase contrast angiography sequence was also acquired
perpendicular to the descending aorta. Visualizations and analysis was
performed using a freely available software Segment and FourFlow (Medviso AB,
Lund, Sweden). Flow values of total flow and mean flow velocity were calculated
and compared.Results
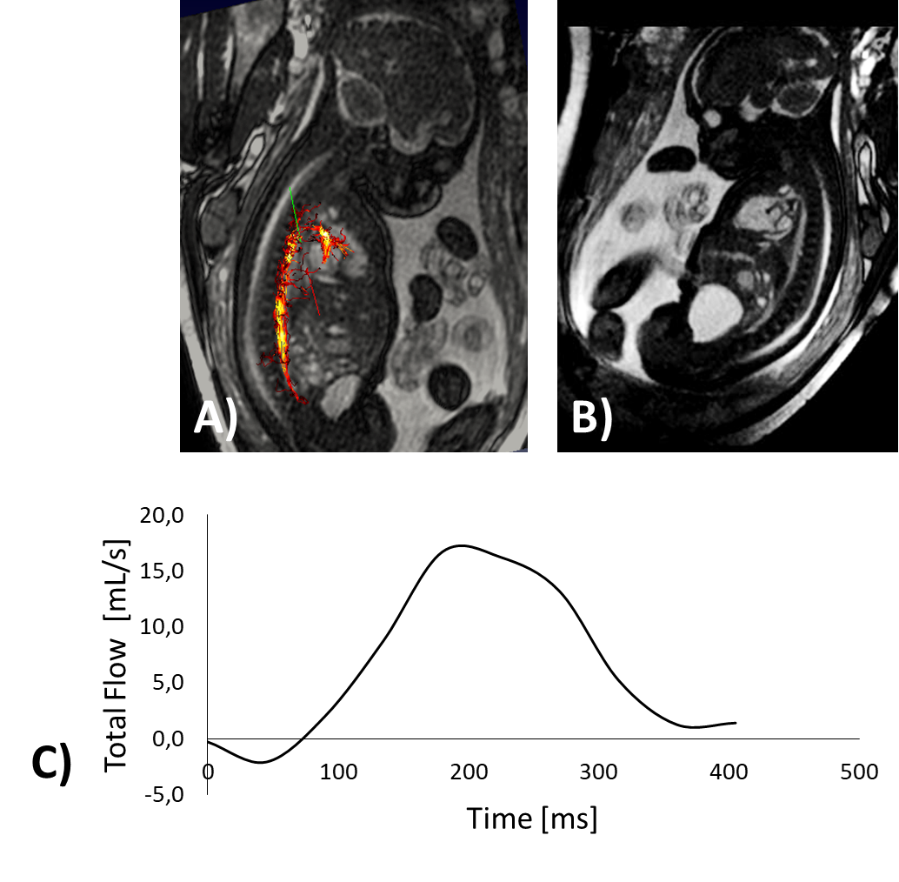
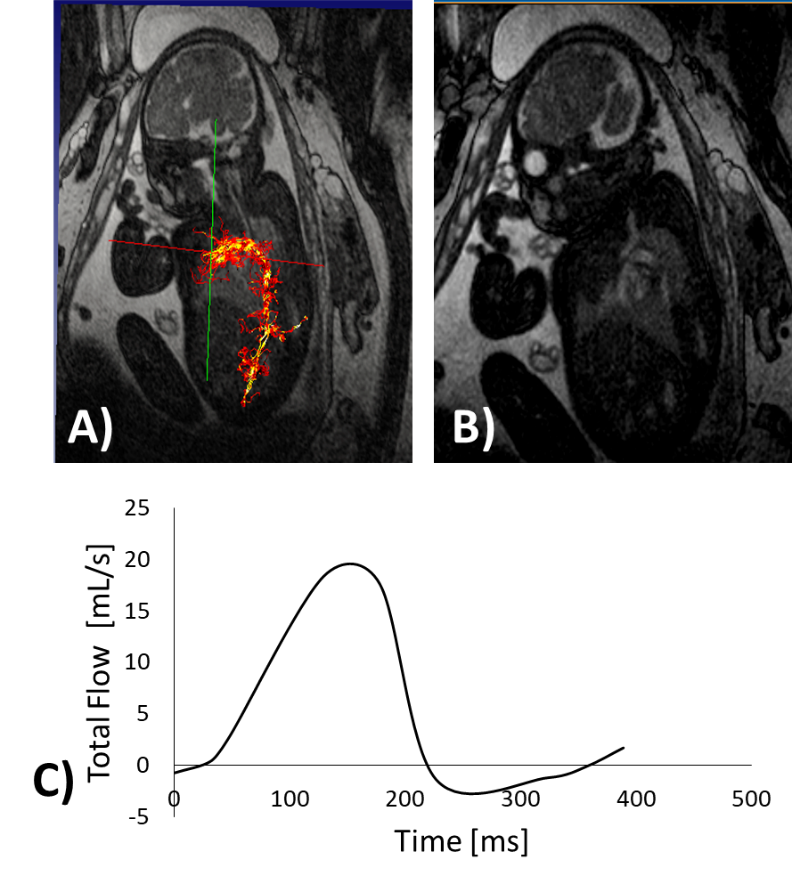
For the phantom measurements mean calculated flow and mean stroke volume were 6.1 ± 0.1 mL/s and 5.3 ± 0.5 mL, respectively. In Comparison, calculated mean flow and stroke volumen from 4D quantification were 6 ± 1 mL/s and 5 ± 0.3 mL. The DUS device could be reliably used for fetal cardiac gating and thus provided stable trigger signals throughout each scan. Due to the late gestational week (35 week) the first fetus showed less motion during the examination than the second one, in which the 4D sequence had to be repeated due to severe motion. Blood flow quantification was possible for each fetus and the blood flow in the descending aorta, aortic arch and ductus arteriosus could be visualized (Figure 2, Figure 3). Mean calculated stroke volumes of the two fetuses from the 3D velocity encoding were 2.8 / 2.7 mL with peak velocities of 115 / 66 cm/s, respectively. In comparison, stroke volumes and peak velocities calculated with standard 2D phase contrast sequence were 3.0 / 3.4 mL and 90 / 115 cm/s, respectively.Discussion
Quantitative measurements were well comparable between 4D and 2D phase contrast acquisitions for both the fetal phantom and for the human subjects. Fetal movement is a challenge due to long acquisition times and needs to be addressed in future studies.Conclusion
This preliminary study showed the possibility of visualization and quantitative measurements of blood flow in-utero within the great fetal vessels with 4D phase contrast imaging utilizing the Doppler ultrasound gating method. The technique may be beneficial for visualization and quantification of complex congenital cardiovascular malformations.Acknowledgements
No acknowledgement found.References
1. Wielandner A et al, Semin Fetal Neonatal Med 2013;18:286–97
2. Yamamura J et al,J Magn Reson Imaging 2012;35:1071–6.
3. Jarvis, K et al. JCMR, 18(1), 59.
Figures