3361
Quantification heterogeneous wall displacement and circumferential strain in the thoracic and abdominal aorta by spiral cine DENSE MRI1Radiology and Imaging Sciences, Emory University, Atlanta, GA, United States, 2Research and Development, Siemens Healthineers, Atlanta, GA, United States
Synopsis
We used spiral cine DENSE (Displacement Encoding with Stimulated Echoes) MRI in the aortic wall to examine the heterogeneity of displacement and strain at three axial locations along the aorta. The major findings of this study were that spiral cine DENSE MRI is a viable technique for assessing patient-specific aortic wall kinematics in-vivo, that regional displacement and circumferential strain are heterogeneous and vary depending on aortic location, and neither mean nor maximum displacement co-localized with sections of peak circumferential strain.
Inroduction
Local mechanics of the vascular wall plays a key role in maintaining vascular health and governing aortic remodeling in response to acute and chronic events (1). Assessing patient-specific aortic wall mechanics in vivo requires a reliable method to quantify heterogeneous regional aortic kinematics non-invasively. The majority of current imaging studies limit kinematic evaluation to simulated displacements and homogenized values of circumferential strain based on diameter change during the cardiac cycle. A few prior studies using ultrasound or MRI have suggested circumferential heterogeneities in aortic motion, but none have mapped the regional aortic wall kinematics to evaluate the spatial relationship between mean or maximum displacement and maximum strain, both of which are metrics which may play an important mechanobiological role in regional susceptibility and rupture-risk of aortic aneurysms and dissections (2,3). We used recent advancements in aortic cine DENSE (Displacement Encoding with Stimulated Echoes) MRI to heterogeneity of displacement and strain at three axial locations along the aorta. We hypothesized that peak strain and displacement would be circumferentially heterogeneous and peak displacement and peak strain would not be co-localized.Methods
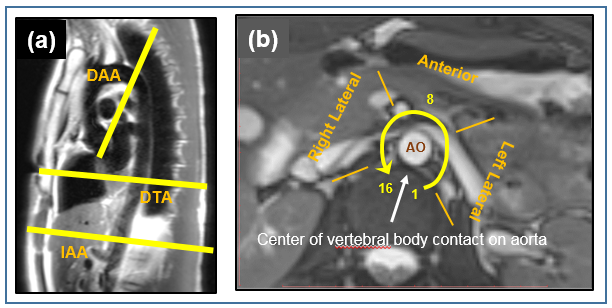
Transverse, ECG-gated, 2D, spiral cine DENSE images were acquired on a 3T Siemens MRI (Trio or Prisma) in 15 healthy volunteers (ages 19-65) at three aortic locations: infrarenal abdominal aorta (IAA), descending thoracic aorta (DTA), and distal aortic arch (DAA), Figure 1a. Displacement data were acquired over the cardiac cycle in the phase-encoding and readout directions (resolution=1.3 x 1.3 x 8 mm, TE=1.2 ms, TR=16 ms, w=0.17-0.25 cycles/mm). Using in-house Matlab code, the aortic wall was manually segmented, wall motion was tracked, and Green strain was calculated using an interpolation function over quadrilateral elements. Time and displacement smoothing, overlapping sectorization, and reference point averaging were employed to reduce noise while preserving regional heterogeneities in displacement and strain. Patient-specific displacement was quantified at each voxel in the segmentation, and mean circumferential strain was calculated for each of 16 sectors around the wall. Co-localization of mean and peak wall displacement and peak strain was assessed by sector and by section (groupings of 4 sectors each into posterior, left lateral, anterior, and right lateral walls in the IAA and DTA (Figure 1b).Results
Peak systolic displacement and circumferential strain around the aortic wall was heterogeneous at all three axial locations, Figure 2. In the IAA, mean displacement was consistently anterior (opposite the spine), and peak displacement occurred either anteriorly or right anterolaterally. However, peak circumferential strain occurred in the lateral walls in 5 of 6 volunteers. In no patients did the mean or peak displacement occur in the same sector as maximum strain (mean diff. ±4.0 and ±4.3 sectors, respectively). In the DTA, both mean and peak displacement were consistently anterior toward the left ventricle; however, peak strain was consistently in the lateral walls, and there was no co-localization of mean or peak displacement and strain by either sector or section (mean diff. ±4.0 sectors for both). In the DAA, mean displacement was directed toward the greater curvature in 4/6 and lateral wall in 2/6 volunteers, but peak displacement was variable. Peak strain occurred in the medial wall (next to the vertebra) in the 4 oldest patients (age>50) and in the greater curvature in the 2 youngest patients (age<40). Strain did not co-localize to mean or peak displacement in any sector (mean diff. ±4.7 and ±4.5 sectors, respectively) and only co-localized by section in 1/6 volunteers.Discussion
The major findings of this study were: 1) spiral cine DENSE MRI is a viable technique for assessing patient-specific aortic wall kinematics in-vivo, and 2) regional displacement and circumferential strain are heterogeneous and vary depending on aortic location. Neither mean nor maximum displacement co-localized with peak circumferential strain (0/16 by sector and only 2/16 by section), emphasizing the need to consider these motion and strain independently and to assess their values regionally. Quantification of these heterogeneities may directly provide novel metrics for assessing patient-specific vulnerability to the development or progression of aortic aneurysms and dissections, and indirectly provide the essential spatiotemporal data needed to improve understanding of the regional mechanobiological stimuli that govern aortic remodeling and the assignment of regionally heterogeneous material properties in patient-specific aortic computational models.Conclusion
Regional aortic wall displacement and strain can be quantified in vivo using spiral cine DENSE MRI, and both displacement and strain are patient-specific and circumferentially heterogeneous. Neither mean nor peak displacement is co-localized with peak circumferential strain.Acknowledgements
No acknowledgement found.References
1. Fillinger MF, Marra SP, Raghavan ML, Kennedy FE. Prediction of rupture risk in abdominal aortic aneurysm during observation: wall stress versus diameter. J Vasc Surg. 2003 Apr;37(4):724-32.
2. Haraldsson H, Hope M, Acevedo-Bolton G, Tseng E, Zhong X, Epstein FH, Ge L, Saloner D. Feasibility of asymmetric stretch assessment in the ascending aortic wall with DENSE cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2014 Jan 9;16:6
3. Califano JP, Reinhart-King CA. Exogenous and endogenous force regulation of endothelial cell behavior. J Biomech. 2010 Jan 5;43(1):79-86. 4.
Figures