3354
Pulmonary venous and coronary artery visualization from isotropic whole-heart kt-accelerated 3D cardiac CINE MRI1Erasmus MC, Rotterdam, Netherlands, 2Research Institute of Radiological Science, Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea, 3Altman CTRI, San Diego, CA, United States
Synopsis
Isotropically-acquired 3D cine cardiac MRI has potential for quantification of cardiac size and function, which has been previously studied. We observed that pulmonary veins and coronary artery origins can be seen with this technique, and sought to further evaluate diagnostic visualization of these vessels. Two observers scored the coronary artery origins and pulmonary veins using a 5-point Likert score. Pulmonary veins were more readily visualized than coronary arteries. Isotropically-acquired 3D cine cardiac MRI enables depiction of vascular anatomy, and potentially may be used for pulmonary venous mapping and depicting coronary anomalies.
Introduction
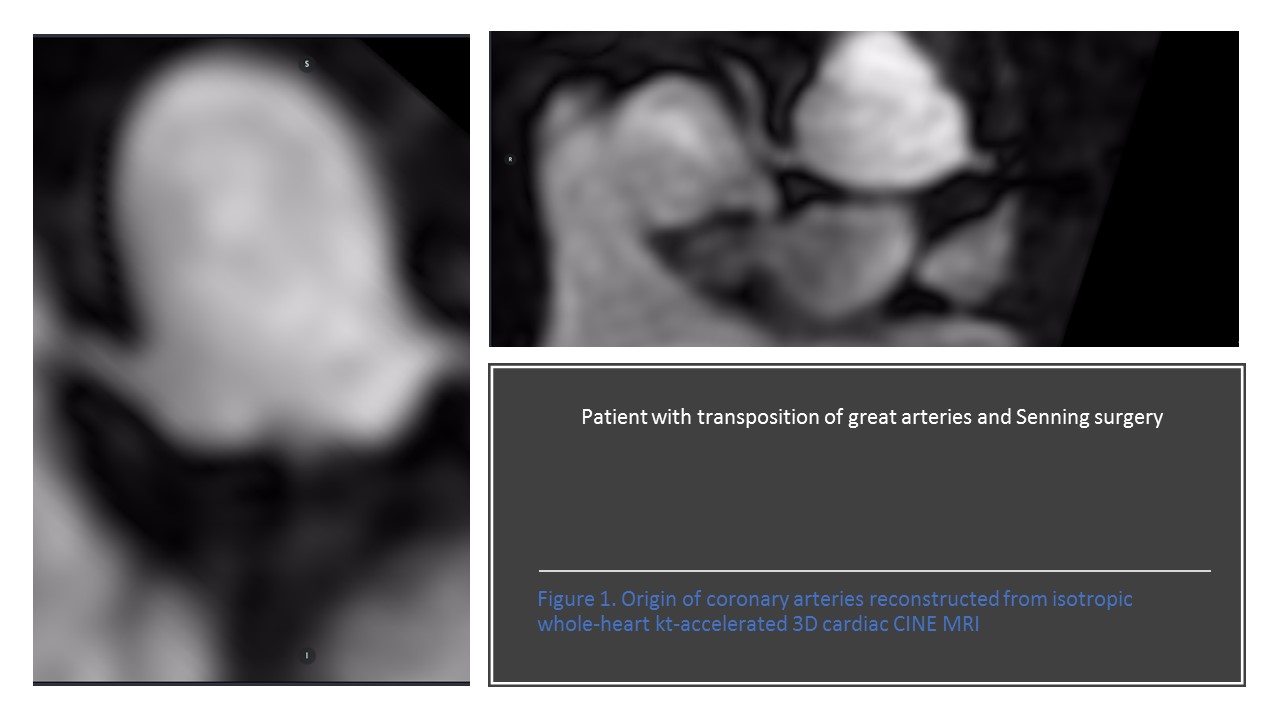
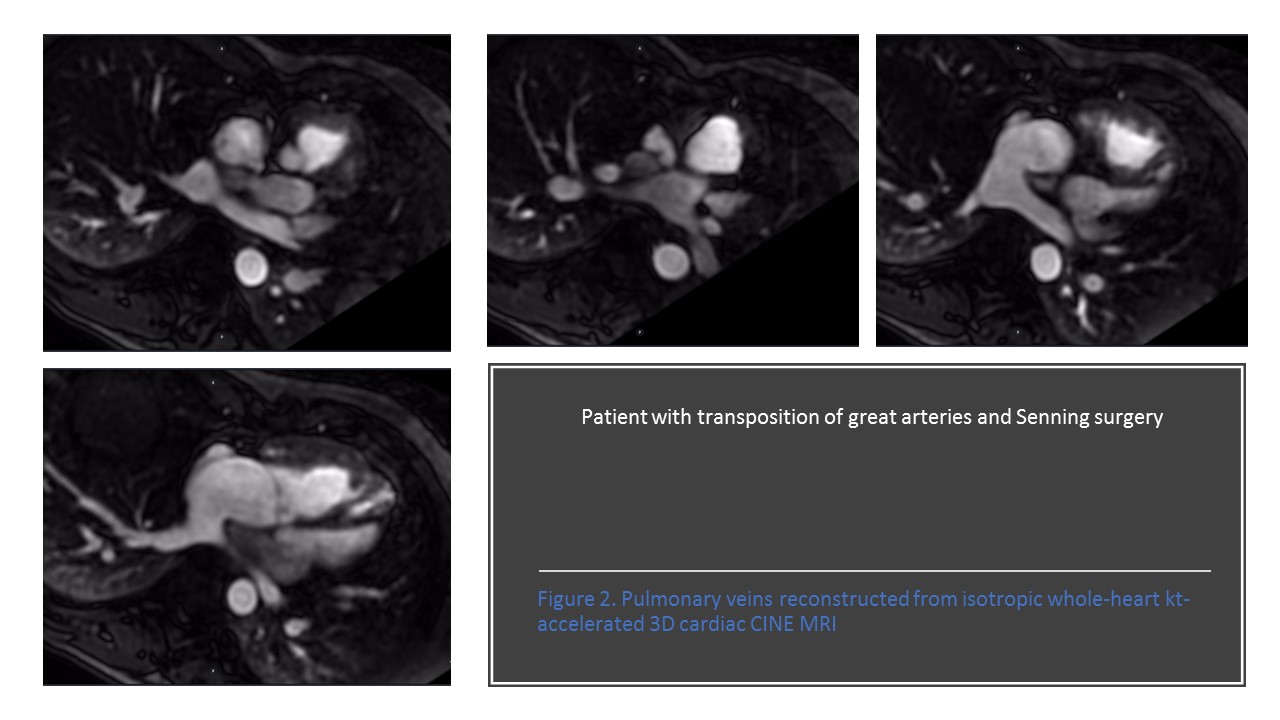
Isotropic whole-heart kt-accelerated 3D cardiac CINE MRI, acquired during one or two breath-holds, can help simplify acquisition of cardiac size and function data (1-3). We observed that pulmonary veins and occasionally coronary artery origins are apparent with this technique, which can be additional indications for MRI, especially for excluding anomalous origin of the coronary arteries. We therefore sought to evaluate the quality of visualization of these vessels with this imaging technique.Methods
With local IRB approval and HIPAA compliance, we retrospectively identified all patients referred for cardiac MRI, including isotropically acquired breath-held kt-accelerated 3D Cine. We identified MRI exams between March and October 2017 performed for 63 patients. Mean heart rate was 68.4 ±12.6. 3D Cine acquisitions were performed on clinical 3T MR scanner (GE Healthcare, Wi) after injection of 0.3 ml/kg gadolinium–based (gadobenate dimeglumine) intravenous contrast, during one (46%) or two breath-holds (54%). Acquisitions were performed during first-pass contrast-enhancement using a timing bolus targeting left ventricular enhancement. When two-breath holds were used, each breath-hold of the multislab acquisition was performed using half the volume of intravenous contrast. The coronary arteries and pulmonary veins were identified on volumetric data and visualized in at least two orthogonal planes and scored by two observers using a 5-point scale (1: not seen, 2: poor delineation due to low signal intensity and/or marked blurring, 3: moderate enhancement and/or blurring, 4: high signal intensity and slight blurring, and 5: high signal and no blurring (4). Further these scores were grouped in acceptable (3,4,5) and unacceptable (1,2). Contrast ratio of enhancement between left atrium and myocardium was also measured. Statistical comparisons were performed with t-tests.Results
The average score for left main coronary artery was 3.6 ± 1.0, for right coronary artery 3.5 ± 1.03, for right pulmonary veins 4.7 ± 0.5 and for left pulmonary veins 4.6 ± 0.5. Qualitative scores for the pulmonary veins were significantly higher than the coronary arteries (p<0.05, t-test). There was not significant difference in scores between one-breath-hold acquisitions compared with two-breath-hold acquisitions. Contrast enhancement ratio was 2.5 ± 0.9 for one-breath hold and ??? for two-breath hold. There was not a significant difference between the two techniques.Discussion
Isotropic kt-accelerated 3D cine cardiac MRI offers the possibility of measuring cardiac size and function with only one or two breath-holds in a multislab acquisition. Further, it may also be used for pulmonary vein visualization and proximal coronary arteries. So, it has potential to be used for pulmonary vein mapping before ablation or depiction of coronary anomalies, which is an important added value in imaging of congenital heart patients.Conclusions
In this study, we show that kt-accelerated 3D Cine imaging is a feasible technique for visualization of the pulmonary veins and occasionally can visualize the coronary origins.Acknowledgements
GE Research GrantReferences
1. Greil GF, Germann S, Kozerke S, et al. Assessment of left ventricular volumes and mass with fast 3D cine steady-state free precession k-t space broad-use linear acquisition speed-up technique (k-t BLAST). J Magn Reson Imaging. 2008;27(3):510-515. doi:10.1002/jmri.21200.
2. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE: Dynamic MRI With High Frame Rate Exploiting Spatiotemporal Correlations. Magn Reson Med. 2003;50(5):1031-1042. doi:10.1002/mrm.10611.
3. Okuda S, Yamada Y, Tanimoto A, et al. Three-dimensional cardiac cine imaging using the kat ARC acceleration: Initial experience in clinical adult patients at 3T. Magn Reson Imaging. 2015;33(7):911-917. doi:10.1016/j.mri.2015.04.004.
4. Hope TA, Petkovska I, Saranathan M, Hargreaves BA, Vasanawala SS. Combined parenchymal and vascular imaging: High spatiotemporal resolution arterial evaluation of hepatocellular carcinoma. J. Magn Reson Imaging 2016 ;43 :859-865
Figures