3353
Contrast-enhanced magnetic resonance angiography (MRA) in pre-surgical planning of deep inferior epigastric artery perforator flaps: comparison with surgical outcomes1Department of Diagnostic and Interventional Imaging, KK Women's and Children's Hospital, Singapore, Singapore, 2Department of Plastic, Reconstructive and Aesthetic Surgery, KK Women's and Children's Hospital, Singapore, Singapore
Synopsis
Deep inferior epigastric perforator (DIEP) flap reconstruction is an excellent choice because only the subcutaneous fat is used. DIEP flap reconstruction requires selection of a suitable perforator vessel, which can be highly variable in size and location. Pre-operative imaging can identify these vessels. Doppler sonography is the standard imaging modality, but has mixed results. CT angiography is accurate, but involves ionising radiation. MR angiography is less commonly used, but obviates any radiation exposure. This study shows that MR angiography is an accurate imaging modality to detect the size and location of suitable perforator vessels. Pre-operative knowledge of these vessels allows for optimal surgical planning, reduced area of surgical dissection and shortened dissection times.
Introduction
There are multiple reconstruction options available to women after mastectomy. Deep inferior epigastric perforator (DIEP) flap reconstruction is an excellent choice for autologous breast reconstruction because only subcutaneous abdominal fat is used. The rectus muscle remains intact, resulting in less donor site complications.A breast cancer patient may undergo multiple radiologicial examinations involving ionising radiation. Computed tomography (CT) angiography is a highly accurate modality for detection of the perforators, but will increase the amount of radiation the patient receives. MR angiography of the anterior abdominal wall perforators is an alternative to CT angiography and will obviate any radiation exposure. This study was performed to evaluate the ability of MR angiography to localise the anterior abdominal wall perforator vessels, with surgical outcomes as an end point.Methods
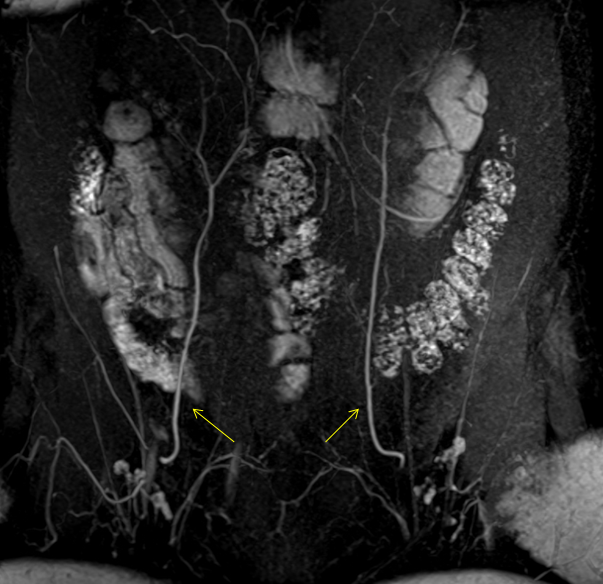
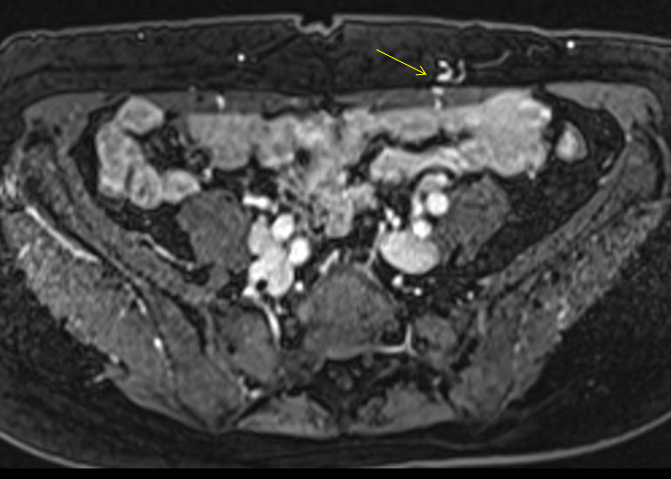
In our institution, all patients who desire breast reconstruction surgery with an autologous abdominal-based flap will undergo either a CT angiography or a MR angiography study. Patients who underwent MR angiography were included in this study. This is a retrospective review of the data from all the MR angiographic studies performed at our institution during a period between June 2011 and December 2015. A total of 28 patients underwent MR angiography which was performed on either a 1.5 MRI scanner (Signa HDXT, GE) or a 3 T MRI scanner (Magnetom Skyra, Siemens Healthcare). Three-dimensional (3D) gadolinium-enhanced fat-suppressed T1-weighted gradient-echo sequence were performed in the axial and coronal planes. All patients received a standard dose of gadoterate meglumine (Dotarem; Guerbet LLC). Up to 3 perforator vessels were localised on each side of the umbilicus for potential harvesting. The size (diameter) and distance of each perforator from the umbilicus along the axial and cranio-caudal axes were documented. The size of the vessels were defined as large if its diameter measured > 1.5 mm, moderate if its diameter was between 0.8-1.5 mm and small if it measured < 0.8 mm in diameter.
Results
2 patients were scanned on the 1.5 T scanner and 26 patients were scanned on the 3.0 T scanner. Out of the 28 patients who underwent MR angiography, 5 patients declined to undergo surgery. 23 patients subsequently underwent autologous abdominal-based breast reconstruction surgery and comprised our study population. Of the 23 patients, MR angiography detected 14 (61%) patients with optimally located large and moderate sized perforators. These patients were identified as suitable candidates for DIEP flap reconstruction. The location of these perforators were marked with ink on the anterior abdominal surface prior to surgery based on the MR angiographic findings and confirmed with the use of ultrasound Doppler. DIEP flap reconstruction surgery was successfully performed. 3 patients (13%) had small sized perforators based on MR angiography. These could be found on ultrasound Doppler examination, but the decision was made to perform muscle-sparing transverse rectus abdominis myocutaneous (ms-TRAM) flap reconstruction instead due to the small size of the perforators. 6 patients (26%) underwent free TRAM flap reconstruction. MR angiography showed that for 2 patients, even though there were good size perforators, they were in a suboptimal location. In 4 patients, there were no significant perforators. Of these, one patient underwent bilateral free TRAM flap reconstruction.
Discussion and Conclusion
Pre-operative knowledge of the size and location of the variable perforators in DIEP flap reconstruction allows the surgeon to avoid extensive dissection and focus on the area where the perforator is expected to pierce the rectus fascia. This allows for optimal pre-surgical planning, a smaller dissection area and shortened dissection times.Our study has shown that MR angiography is able to select patients for the different types of autologous breast reconstruction surgery. Identification of large and moderate perforator vessels enabled successful DIEP flap reconstruction surgery in 61% of our patients. MR aniography detected 39% patients with small or unsuitable perforators. These patients underwent non-DIEP abdominal reconstruction surgery depending on the MR angiography findings. MR angiography is therefore a useful imaging modality in the pre-operative evaluation of perforator size and location in patients undergoing autologous abdominal breast reconstruction surgery.
Acknowledgements
NilReferences
1. Knox AD, Ho AL, Leung L et al. Comparison of outcomes following the autologous breast reconstruction using the DIEP and pedicled TRAM flaps: a 12-year clinical retrospective study and literature review. Plast Reconstr Surg 2016; 138(1):16-28
2. Karunanithy N, Rose V, Lim AK et al. CT angiography of inferior epigastric and gluteal perforating arteries before free flap breast reconstruction. Radiographics 2011; 31(5):1307-19
3. Chernyak V, Rozenbit AM, Greenspun DT et al. Breast reconstruction with deep inferior epigastric artery perforator flao: 3.0-T Gadolinium-enhanced MR imaging for preoperative localization of abdominal wall perforators. Radiology 2009; 250(2):417-24
4. Schaverien M, Ludman CN, Neil-Dwyer JG et al. Contrast enhanced magnetic resonance angiography for preoperative imaging in DIEP flap breast reconstruction. Plast reconstr surg. 2011; 128(1):56-62
Figures