3352
Accelerated Non-Rigid Respiratory Motion Corrected Simultaneous Bright- and Black-Blood 3D Whole-Heart Coronary MR Angiography1School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
A novel 3D whole-heart sequence for simultaneous bright- and black-blood coronary angiography (named BOOST) was recently introduced. BOOST alternates the acquisition of two differently magnetization-prepared bright-blood volumes for coronary lumen visualization and from which respiratory motion information can be independently extracted. These datasets are subsequently combined in a PSIR-like reconstruction to obtain a complementary co-registered black-blood volume for thrombus/haemorrhage visualization. BOOST acquisitions, however, require prolonged acquisition times. Here, we accelerate BOOST acquisition by exploiting a variable density Cartesian trajectory that generates incoherent undersampling artefacts. Furthermore, non-rigid respiratory motion correction incorporated in the undersampled reconstruction is exploited for improved sharpness.
Introduction
MRI is a promising and non-invasive technique for the visualization of coronary lumen, thrombus, and intraplaque haemorrhage. Typically, non-contrast enhanced bright-blood coronary MRA (CMRA) and black-blood T1-weighted acquisitions are performed sequentially for the visualization of the coronary lumen and thrombus/haemorrhage, respectively1. Such approaches, however, suffer from limited volumetric coverage and, additionally, the extraction of respiratory motion parameters from the black-blood image poses challenges. Furthermore, the presence of motion between these sequential acquisitions can compromise the process of image fusion between the bright-blood coronary lumen and the black-blood coronary thrombus/haemorrhage datasets. To overcome these drawbacks, a 3D whole-heart bright- and black-blood phase sensitive inversion recovery (PSIR) sequence, named BOOST2, was recently introduced. BOOST enables the acquisition of two differently weighted bright-blood datasets for the visualization of the coronary lumen and for the estimation of motion parameters. With this approach, a complementary and fully co-registered black-blood volume for thrombus/haemorrhage characterization is obtained from the PSIR reconstruction. The acquisition of two high-resolution 3D bright-blood datasets, however, requires prolonged acquisition times (~20min). In this study, we sought to accelerate BOOST data acquisition by exploiting an undersampled 3D variable density Cartesian trajectory with spiral profile order3 (VD-CASPR). Furthermore, this accelerated BOOST framework is here integrated with non-rigid respiratory motion correction4 to obtain sharper bright-blood coronary lumen depiction and to reduce phase errors in the complementary black-blood PSIR reconstruction.Methods
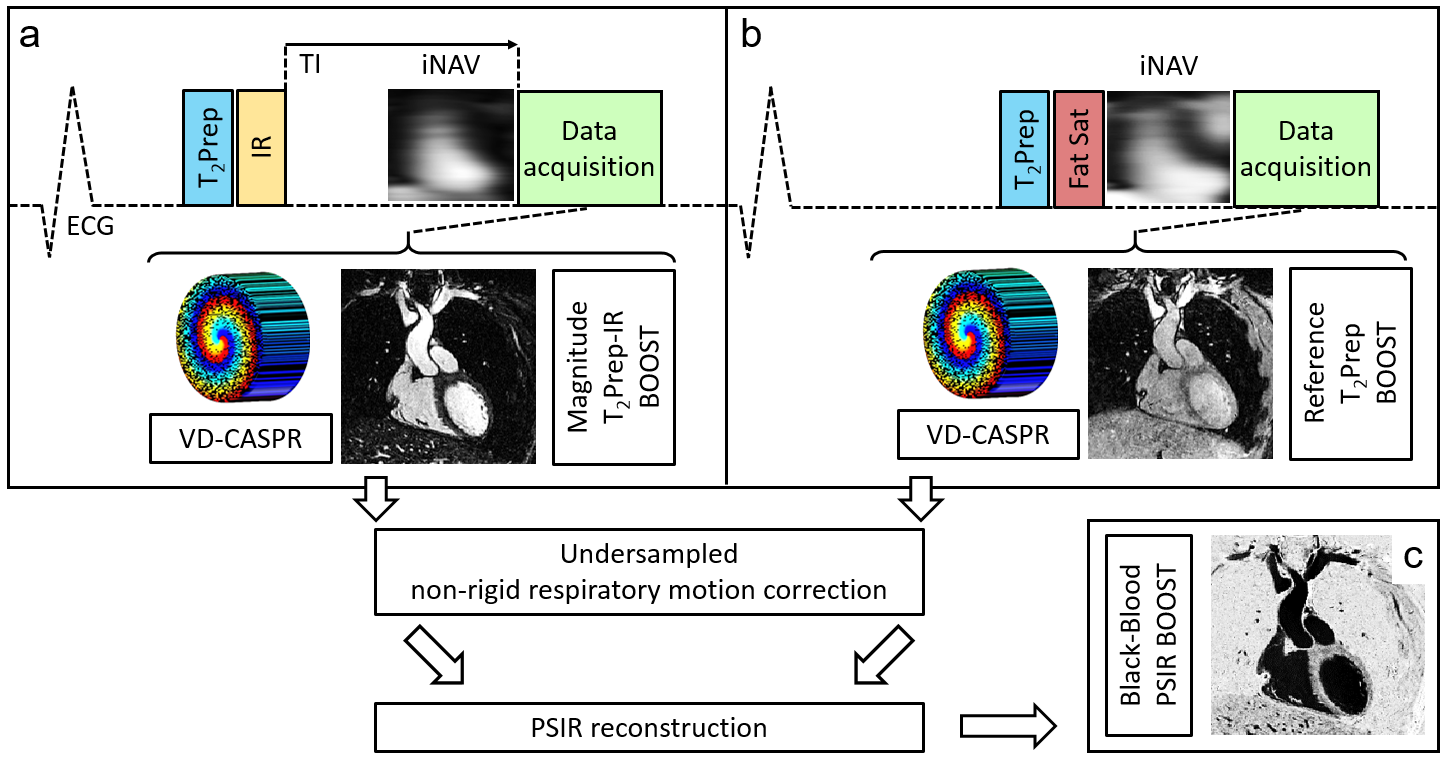
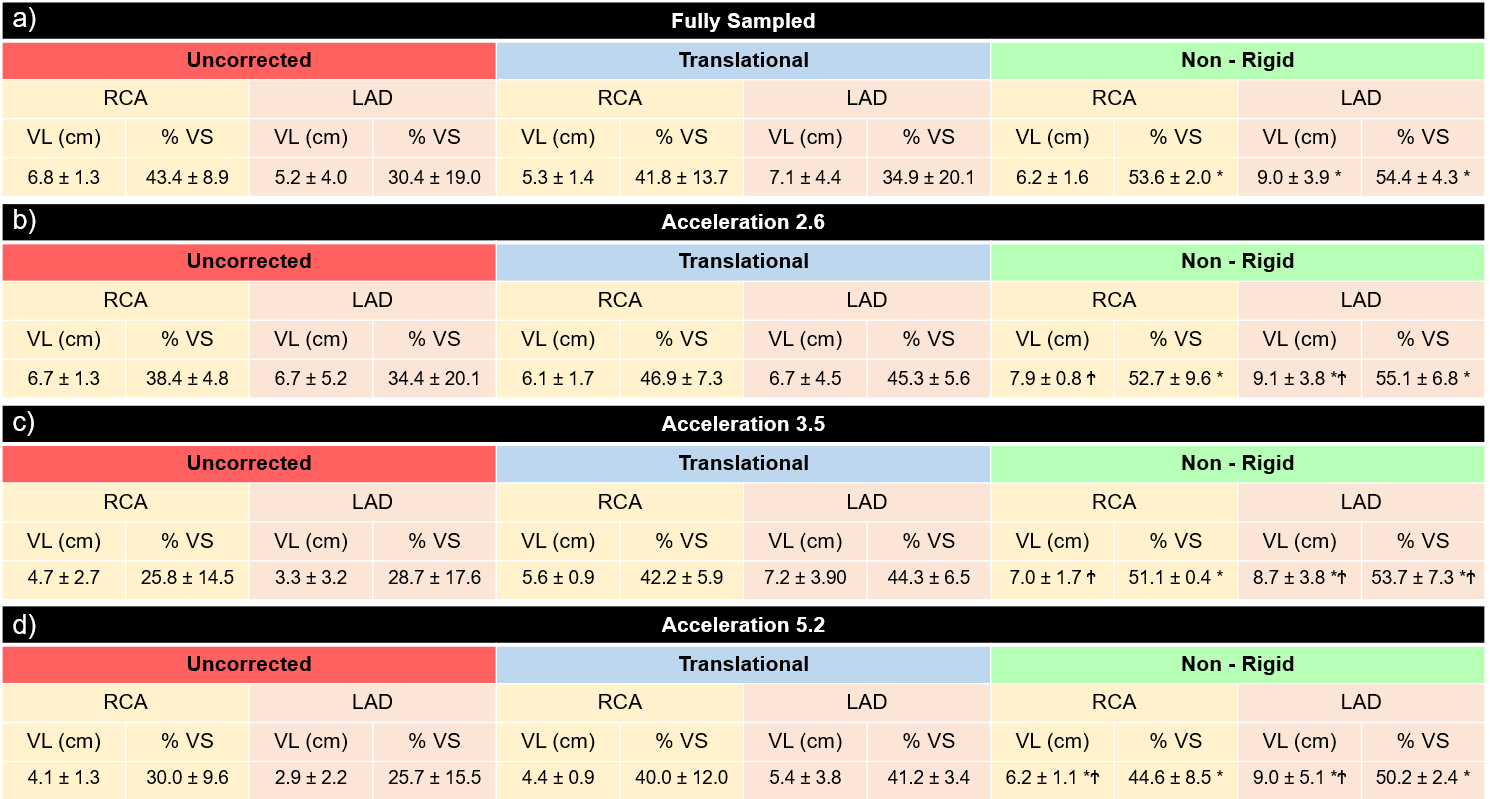
Framework: A 3D undersampled VD-CASPR sampling was integrated into the BOOST sequence2 as illustrated in Fig1. VD-CASPR samples the ky-kz phase-encoding plane with spiral interleaves on a Cartesian grid with variable density sampling along each spiral arm, leading to incoherent undersampling artefacts when high acceleration is exploited. Moreover, the use of VD-CASPR allows for high quality respiratory-resolved reconstructions from highly undersampled data, which is crucial for accurate estimation of 3D non-rigid motion fields via image-based registration. The BOOST sequence alternates the acquisition of a T2-prepared Inversion Recovery module in odd heartbeats (T2Prep-IR BOOST dataset), whereas T2-preparation solely is applied in even heartbeats (T2Prep BOOST dataset). The acquisition of a low-resolution 2D image-based navigator (iNAV)5 precedes data acquisition in each heartbeat. Data acquisition was performed in 6 healthy subjects on a 1.5T system (Siemens Magnetom Aera) using the proposed prototype accelerated BOOST framework integrated with VD-CASPR sampling. Three different acceleration factors (2.6x, 3.5x, and 5.2x, corresponding to acquisition times of ~9min, ~7min, and ~5min, respectively) were investigated. A fully sampled BOOST acquisition (with eliptical shape3, ~20min) was performed for each subject for comparison. Imaging parameters included: bSSFP sequence, resolution=1x1x2mm, FOV=320x320x90-100mm, coronal orientation, TE/TR=1.56/3.6ms, flip-angle=90deg, TI=110ms, T2Prep duration=40ms. Image reconstruction: The T2Prep-IR BOOST and the T2Prep BOOST datasets were reconstructed independently. iNAVs were used to estimate 2D superior-inferior (SI) and right-left (RL) beat-to-beat translational motion and to bin data along the SI direction (4-6 bins). After intra-bin translational motion correction, bins were reconstructed using soft-gated Iterative-SENSE and bin-to-bin 3D non-rigid motion was estimated via image registration4. Non-rigid motion was incorporated in the undersampled reconstruction to obtain images at end-expiration. Undersampled non-rigid motion corrected co-registered T2Prep-IR BOOST and T2Prep-BOOST were combined as described in6 to generate the complementary black-blood PSIR BOOST dataset. Data analysis: Coronary percentage vessel sharpness (%VS) and visible vessel length (VL) were computed along the right (RCA) and left anterior descending (LAD) coronary artery7 for all the tested acceleration factors in the undersampled non-rigid motion corrected T2Prep-IR BOOST datasets and compared to the fully sampled reference dataset. Endpoints were quantified for uncorrected and translational corrected datasets for comparison and for all the acceleration factors.Results
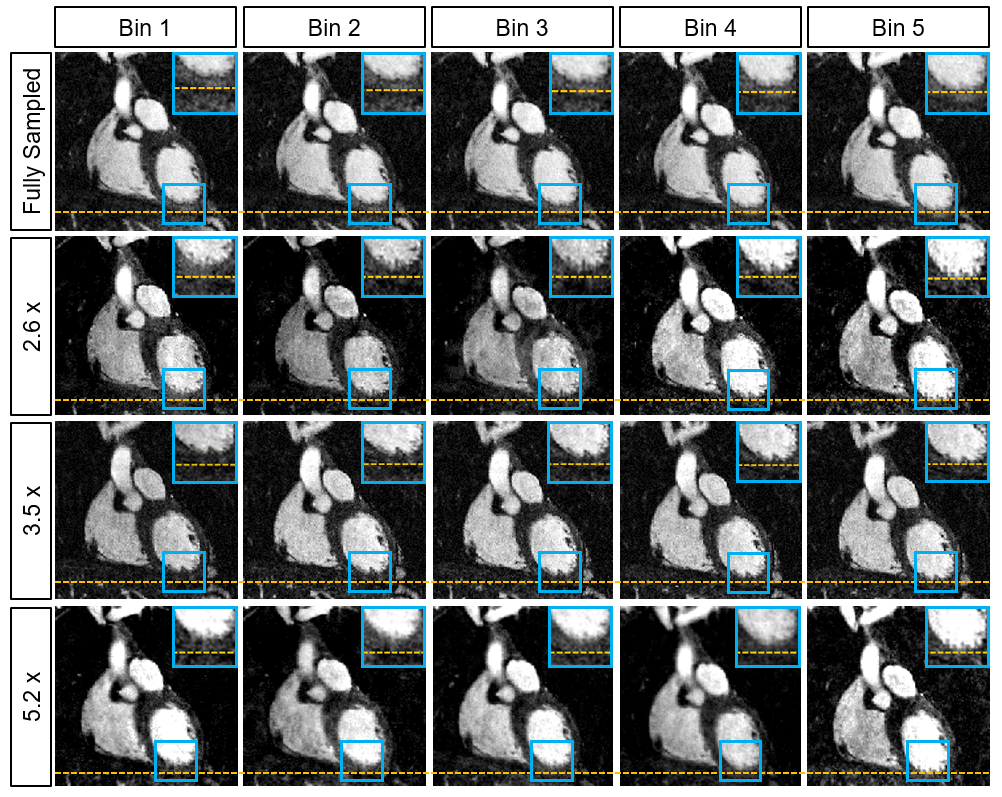
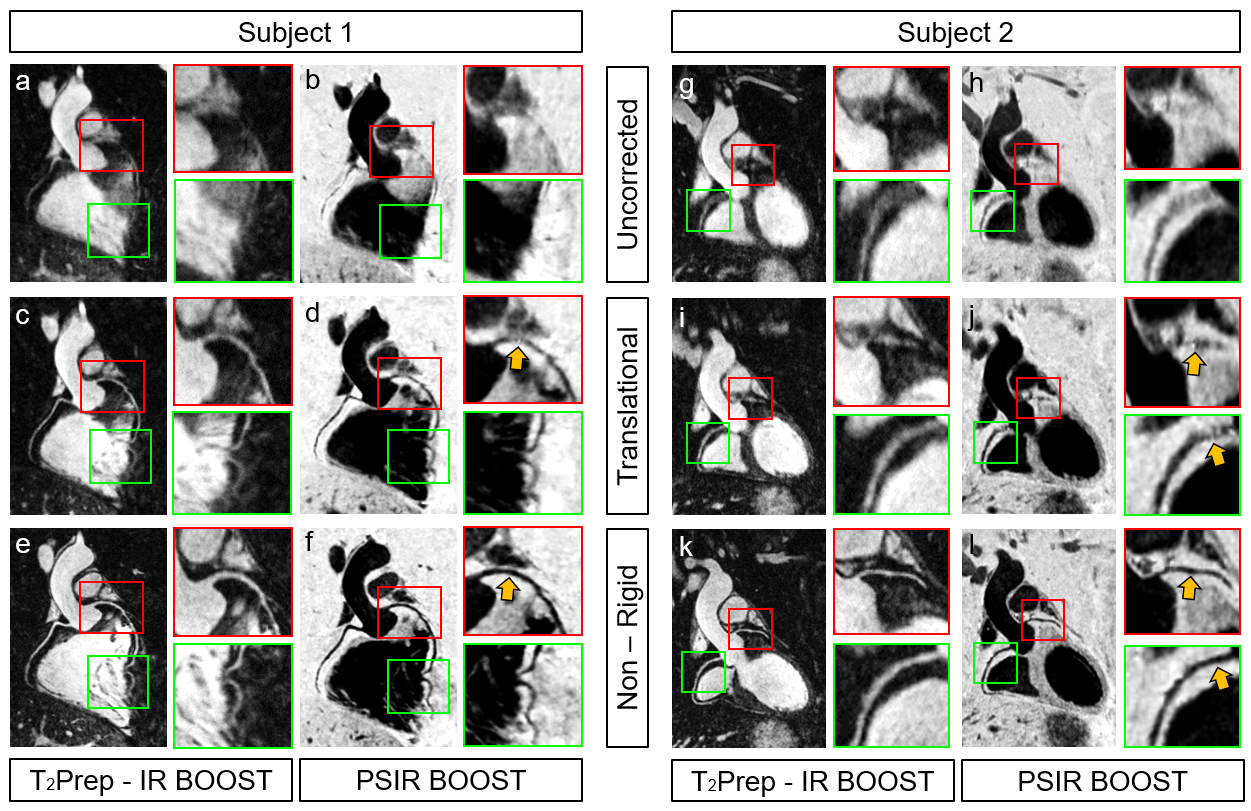
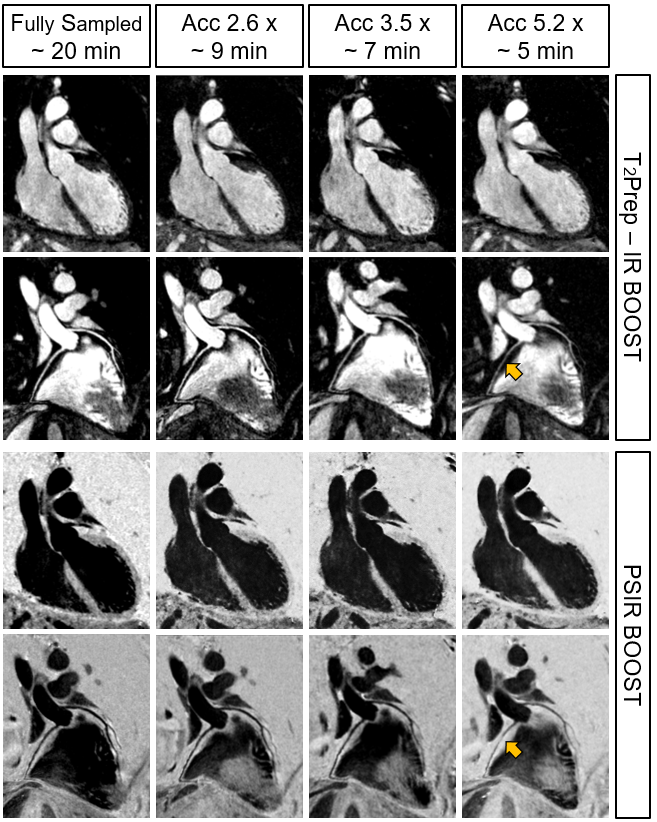
The use of VD-CASPR allowed for accurate estimation of 3D non-rigid motion fields from high quality respiratory-resolved reconstructions obtained from highly undersampled data (Fig2). Undersampled non-rigid motion corrected reconstruction led to improved vessel sharpness in the bright-blood T2Prep-IR BOOST datasets and reduced phase errors in the complementary black-blood PSIR BOOST datasets when compared to the uncorrected and translational motion corrected counterparts (Fig3, Table1). Different acceleration factors provided image quality without significant difference with respect to the fully sampled reference images (Fig4, Table1).Conclusion
A framework for accelerated BOOST data acquisition and undersampled non-rigid respiratory motion correction, leading to clinically feasible acquisition times (<10min), was successfully implemented. The use of VD-CASPR allowed for accurate estimation of 3D non-rigid motion fields from highly undersampled data, resulting in improved image quality and reduced phase computation errors. Clinical validation is foreseen; this framework will be tested in patients with acute coronary syndrome and coronary plaques. Furthermore, the framework will be also tested in post-contrast for accelerated black-blood assessment of late gadolinium enhancement and bright-blood depiction of coronary lumen as introduced in8.Acknowledgements
This work was supported by the following grants: EPSRC EP/N009258/1, EP/P001009/1, EP/P007619/1, and FONDECYT 1161051.References
1. Jansen CH, Perera D, Makowski MR, Wiethoff AJ, Phinikaridou A, Razavi RM, Marber MS, Greil GF, Nagel E, Maintz D, Redwood S, Botnar RM; Detection of intracoronary thrombus by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 2011 Jul 124(4):416-24.
2. Ginami G, Neji R, Phinikaridou A, Whitaker J, Botnar RM, Prieto C; Simultaneous bright- and black-blood whole-heart MRI for noncontrast enhanced coronary lumen and thrombus visualization. Magn Reson Med. 2017 Jul 19. doi: 10.1002/mrm.26815.
3. Prieto C, Doneva M, Usman M, Henningsson M, Greil G, Schaeffter T, Botnar RM; Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J Magn Reson Imaging. 2015 Mar; 41(3):738-46.
4. Cruz G, Atkinson D, Henningsson M, Botnar RM, Prieto C; Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn Reson Med. 2017 May; 77(5):1894-1908.
5. Henningsson M, Koken P, Stehning C, Razavi R, Prieto C, Botnar RM; Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magn Reson Med. 2012 Feb; 67(2):437-45.
6. Kellman P, Arai AE, McVeigh ER, Aletras AH; Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002 Feb; 47(2):372-83.
7. Etienne A, Botnar RM, Van Muiswinkel AM, Boesiger P, Manning WJ, Stuber M; “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magn Reson Med. 2002 Oct; 48(4):658-66.
8. Ginami G, Neji R, Ismail TF, Chiribiri A, Botnar RM, Prieto C; 3D whole-heart phase sensitive inversion recovery (PSIR) for simultaneous bright blood coronary angiography and black blood late gadolinium enhancement (LGE). 25th ISMRM Annual Meeting, 2017, Honolulu, Hawaii, USA, Abstract number 0525.
Figures